
Abstract
Abstract
Purpose:
Congenital and acquired chylothorax presents a unique management challenge in neonates and infants. A failure of conservative therapy requires surgical ligation to prevent continued fluid and protein losses. This article examines a 15-year experience with thoracoscopic ligation of the thoracic duct.
Patients and Methods:
From June 1999 to December 2013, 21 patients presented with chylothorax refractory to conservative management. Sixteen patients presented following cardiac procedures, 1 after tracheoesophageal fistula repair, 1 after extracorporeal membrane oxygenation cannulation, and 1 after trauma, and 2 had congenital chylothorax. Ages ranged from 3 weeks to 5 years, and weights ranged from 2.6 to 12.7 kg. All procedures were performed in the right chest with three ports. All cases consisted of sealing of the duct at the level of the diaphragm, a mechanical pleurodesis, and fibrin glue.
Results:
All cases were completed successfully thoracoscopically. Operative time ranged from 20 to 55 minutes. There were no intraoperative complications. One patient with congenital bilateral chylothorax required a left partial pleurectomy. The chest tube duration postoperatively ranged from 4 to 14 days. Ligation failed in 2 patients, requiring a subsequent thoracoscopic pleurectomy and chemical pleurodesis, respectively.
Conclusions:
Thoracoscopic thoracic duct ligation is a safe and effective procedure even in post–cardiac surgery patients. The site of the leak can be identified in the majority of cases, and tissue-sealing technology appears to be effective. The minimally invasive nature of the procedure has led to more expedient operative repair to avoid the morbidity associated with chyle leak.
Introduction
C
Patients and Methods
A retrospective review of 21 patients who presented with chronic chylothorax refractory to conservative management from June 1999 to December 2013 was performed. Sixteen patients presented following cardiac procedures, 1 patient after tracheoesophageal fistula repair, 1 patient after extracorporeal membrane oxygenation cannulation for meconium aspiration, and 1 patient after trauma, and 2 patients had congenital chylothorax. All of the patients were initially managed by chest tube drainage, making them NPO, and the addition of the medication octreotide. The duration of chylothorax preoperatively was approximately 2 weeks with chest tube outputs of approximately 20–30 mL/kg/day. Ages of the patients ranged from 3 weeks to 5 years old, and weights ranged from 2.6 to 12.7 kg.
Surgical procedures were performed with the patient under general anesthesia and either left main-stem intubation or tracheal intubation and CO2 insufflation. All procedures were performed in the right chest with three ports. The patients were placed in a modified prone position with the right side elevated 30%–45%. An axillary roll and padding at all bony prominences were placed in all cases. Initially a 5-mm port was needed to insert a 5-mm tissue-sealing device (5-mm LigaSure™; Covidien Energy, Boulder, CO), but the last two procedures were performed with 3-mm ports as a 3-mm sealer became available (Justright Surgical, Boulder). The initial 4-mm port for the camera was placed in the seventh intercostal space in the posterior axillary line. A 3-mm port was placed in the midaxillary line approximately two to three interspaces below the camera port for a 3-mm Maryland dissector. The final port (3 or 5 mm) was placed in the midaxillary line approximately at the level of the camera port (Fig. 1). All intrathoracic adhesions and the inferior pulmonary ligament were divided to allow the lung to completely expand at the end of the procedure and allow adequate exposure. All cases consisted of sealing of the duct at the level of the diaphragm with the tissue sealer (Fig. 2) and/or sutures, a mechanical pleurodesis, and insertion of fibrin glue. A chest tube was left in all cases. The chyle leak was noted to significantly diminish during the procedure in all cases. The length of time until removal of the chest tube was recorded.

Port placement for thoracoscopic thoracic duct ligation.
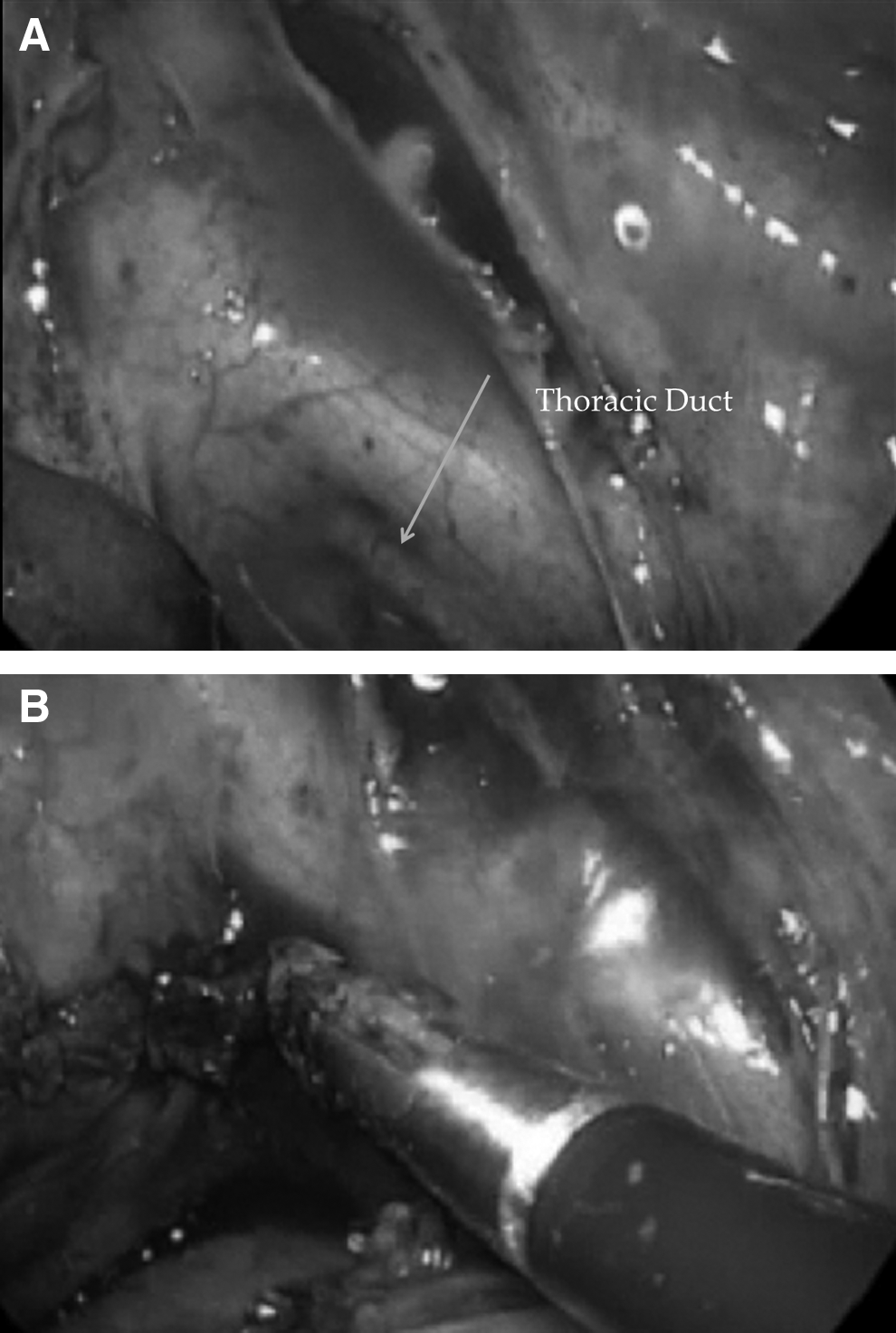
Intraoperative photograph of
Results
All cases were completed successfully thoracoscopically. Operative time ranged from 20 to 55 minutes. There were no intraoperative complications and no conversions to open thoracotomy. One patient with congenital bilateral chylothorax required a second procedure with a left partial pleurectomy. The chest tube drainage dropped significantly in the majority of patients immediately after the procedure. Indication for chest tube removal consisted of having daily output less than 20 mL/kg/day and clear output after initiation of feeds. The chest tube duration postprocedure ranged from 4 to 14 days. Ligation failed in 2 patients, requiring a second procedure: a thoracoscopic pleurectomy in 1 patient and a chemical pleurodesis in the other.
Discussion
Cylothorax is a fairly rare disorder with a high morbidity and mortality rate if left untreated. 2 The etiologies are variable, consisting of both congenital and acquired causes (usually traumatic or postoperative). Post–cardiac surgery accounts for 65%–80% of chylous effusions in children. Initial management typically consists of placement of a chest tube to drain chyle from the pleural space and reduce compression of the lungs, keeping the patient NPO to decrease production of lymphatic flow, and possibly adding medication such as the somatostatin anolog octreotide. 5 However, medical therapy is associated with a high failure rate, and the chyle loss can lead to serious metabolic, nutritional, volume, and immunologic abnormalities. T-cell depletion leads to cell-mediated and humoral impairment, increasing the risk of bacterial and viral infections. 6
Chylothorax is a complex problem to manage, and treatment can be difficult. Although conservative therapy with chest tube drainage may be successful, it may be prolonged, resulting in long-term hospitalization and associated morbidity. Continued drainage and complications from loss of chyle are the main indications for surgery in children with chylous effusions. Although there have been a variety of surgical procedures proposed for treatment, ligation of the thoracic duct has led to repeatedly successful results and is the most frequently performed surgical procedure.7,8 Historically, ligation has been performed through an open thoracotomy, which leads to significant postoperative pain and potential for future chest wall deformity. Recently, authors have published case reports and series demonstrating the safety and efficacy of the thoracoscopic approach to thoracic duct ligation.3,4,9 A combination of direct sealing, local pleurodesis, and fibrin glue application has resulted in successful sealing of the leak in all cases in our series. In a few of the cases, drainage did persist for up to a week, but then it diminished and sealed. There is little morbidity from this minimally invasive approach. In addition, this approach affords excellent visualization and magnification of the posterior thorax, decreased postoperative pain, and less pulmonary dysfunction. The success of this technique may warrant earlier surgical intervention, particularly when it is performed quickly and efficiently to avoid a prolonged anesthetic. If the site of the leak is not readily apparent, a blind ligation and pleurodesis may be performed. Fibrin glue may also be added to provide a complete seal. Even if the procedure is unsuccessful, there is little to be lost by an initial thoracoscopic approach.
Conclusions
Thoracoscopic thoracic duct ligation is a safe and effective procedure even in sick, post–cardiac surgery patients. The site of the leak can be identified in the majority of cases, and tissue-sealing technology appears to be effective in sealing the duct. The minimally invasive nature of the procedure allows for early operation to avoid the often chronic and debilitating fluid and protein losses associated with a major chyle leak.
Footnotes
Disclosure Statement
S.S.R. is a member of Justright Surgical, the company that makes the 3-mm tissue sealer used in 2 cases for this series. B.J.S. declares no competing financial interests exist.