
Abstract
Abstract
Introduction:
Anecdotal reports have demonstrated the feasibility of needle aspiration to deflate a distended bowel, but we do not know of any prospective study that has evaluated this technique. We designed a controlled study to evaluate the use of the selective transperitoneal needle aspiration of a bowel loop (STAB) in infants.
Materials and Methods:
Candidates were patients of less than 6 months of age, scheduled for laparoscopic Nissen fundoplication, in whom severe colonic distension was observed. We randomized the patients to the study drug or placebo in a 1:1 mode. The treatment group received STAB, whereas the control group was subject to conventional maneuvers. We performed 403 Nissen procedures laparoscopically: 102 were in infants ≤6 months old, but only 44 presented severe transverse colonic distension.
Results:
STAB facilitated the surgical procedure and drastically reduced surgical time. Thus, we calculated our sample size with use of the following inputs: 90% power, a critical P value of .05, and 50% reduction in surgical time. This resulted in a necessary sample size of 21 subjects per group, for a total required sample size of 42 subjects. STAB procedures were done in 23 patients, and conventional measures were used in 21. STAB was attempted a total of 45 times. Mean operative time was shorter in the STAB group.
Conclusions:
We propose the use of STAB as alternative therapy to decompress a dilated large-bowel loop during laparoscopic surgery. This maneuver is simple and efficient and has no clinical complications. Future studies are required to evaluate its role in the subset of other patients or procedures.
Introduction
C
An appropriate preoperative preparation usually limits or even prevents the development of bowel loop distension. On some occasions, though, bowel loop distension can be the result of insufficient bowel preparation (i.e., poor patient compliance or acute clinical presentation). Even after an optimal preparation technique, severe distension may also be observed in the setting of an underlying predisposing pathology. Prior studies have reported the use of rectal probes or the administration of dimeticone to reduce large-bowel loop distension, showing limited improvement, whereas other operators have simply decided on conversion to open surgery to improve visualization. 7
Anecdotal reports have demonstrated the feasibility of needle aspiration to deflate a distended bowel loop during open surgery, but we are not aware of any prospective study that has evaluated the safety and efficacy of this technique during laparoscopic surgery. Therefore, we designed a randomized controlled study to evaluate the use of the selective transperitoneal needle aspiration of a bowel loop (STAB) in infants undergoing laparoscopic Nissen fundoplication. We chose to perform the study in a single laparoscopic model (Nissen fundoplication) because the presence of colonic distension represents a common and relevant problem in this type of surgery. The primary outcome measure was surgical time, and secondary outcome measures were conversion rate and intraoperative and postoperative complications.
Materials and Methods
The present study received institutional review board approval, and informed consent was obtained for all patients. We enrolled patients in a consecutive prospective manner on a voluntary basis. The study was conducted between January 2010 and December 2013. Candidates for the study were infants ≤6 months of age with a diagnosis of severe gastroesophageal reflux scheduled for laparoscopic Nissen fundoplication, in whom severe colonic distension was observed intraoperatively. Gastroesophageal reflux disease was diagnosed by the presence of endoscopic esophagitis or positive pH monitoring in patients with typical reflux symptoms. Severe colonic distension was defined as the presence of a distended colonic loop that was interposed between the stomach and the abdominal wall, impeding optimal visualization of the surgical field. We excluded patients with severe comorbidities (complex cardiac disease or severe respiratory dysfunction) or sepsis.
We randomized the patients to the study drug or placebo in a 1:1 fashion. The treatment group received STAB, whereas conventional maneuvers were performed in the control group as per operator discretion. The randomization was performed on the day of surgery with computer generated random allocation.
Procedure
In both groups, infants fasted for 4 hours prior to the procedure and received ceftriaxone 100 mg/kg 2 hours prior the surgery. We did not place rectal probes or administer enemas or antiflatulent agents. We performed Nissen fundoplication according to standard laparoscopic technique through four ports (two ports of 5 mm and two of 3 mm) with a 30° laparoscope. The presence of severe colonic distension was defined after all ports were placed.
The site for the percutaneous introduction of the needle was identified by soft palpation of the abdominal wall. We introduced a 30-gauge hypodermic needle into the abdominal wall on a perpendicular fashion. By laparoscopic vision (Figs. 1–4), we then pulled up the transverse colon closer to the abdominal wall with a surgical grasp that was operated from a lateral port. At that point, we advanced the needle into the transverse colon at its antimesenteric border and continued with gentle aspiration from the lumen using a 20-mL syringe. Care must be taken to avoid aspiration of solid material because it can rapidly block the needle. Without removing the needle, a full syringe was emptied and reused to aspirate as many times as needed in order to decompress the dilated loop and allow safe access to the targeted organs. In the case of a suboptimal result after the first attempt, aspiration could be performed at other sites if required. By protocol, three puncture attempts were permitted. Afterward, the procedure proceeded as planned. In the control group, the operators performed conventional maneuvers such as deviating the dilated loop downward using surgical tools and/or placing the patient on a high Fowler's position.

Illustration of the puncture going through the abdominal wall until the bowel and subsequent aspiration. Courtesy of Dr. Martínez Ferro.
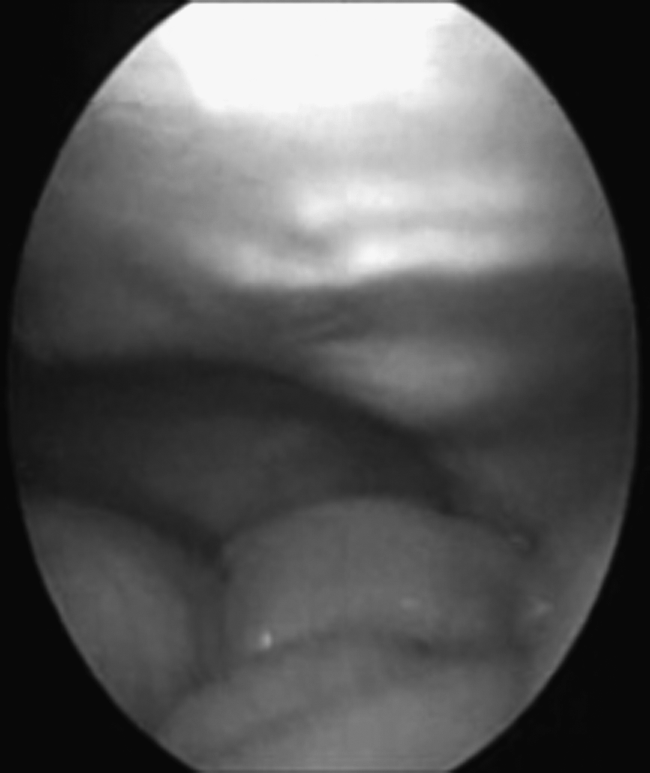
Colon dilatation at the beginning of the procedure.

Bowel puncture at the antimesenteric side.

After the puncture, with enough space and without an intestinal leak.
Surgical time only included the time needed to perform the Nissen procedure and its related complications. We did not include the time required to perform gastrostomies.
During the study period, we performed 403 Nissen procedures laparoscopically, 102 were in infants ≤6 months old, whereas only 44 presented severe transverse colonic distension. Twenty-four were girls, and 16 were boys. Surgical indications were as follows: recurrent bouts of pneumonia in 17 infants, apnea crisis in 16, and cyanosis crisis in 11. A concomitant gastrostomy was placed in 9 patients (6 in the STAB group and 3 in the control group).
Data collection and follow-up
We collected the following data: age, gender, weight, surgical time, intestinal leak, hemorrhage, conversion to open surgery, time to oral feeding, and presence of fever or sepsis. All patients (relatives or next of kin) were contacted at 1 and 4 weeks after the procedure.
Sample size
STAB will ease the surgical procedure and drastically reduce surgical time. Thus, we calculated our sample size with use of the following inputs: 90% power, a critical P value of .05, and 50% reduction in surgical time. This resulted in a necessary sample size of 21 subjects per group, for a total required sample size of 42 subjects. We added 2 more patients in case of improper collection of data.
Statistical analysis
We analyzed group differences in the study baseline and procedural characteristics along with primary and secondary end-point parameters (surgical time, conversion rate, complication rates). Data were expressed as mean±standard deviation. A two-tailed unpaired t test (or Mann–Whitney U test for nonparametric data) was used to assess differences in continuous variables. Comparisons between continuous variables were performed with paired t test or analysis of variance. Chi-squared or Fisher's exact test was used between groups. A value of P<.05 was considered significant.
Results
We performed STAB in 23 patients and conventional measures in 21. STAB was attempted 45 times: 8 (36.4%) patients required one puncture, 8 (36.4) required two punctures, and 7 (27.3%) required three. Mean age was 66.9±38.1 days (range, 17–175 days) in the STAB group and 64.7±36.2 days (range, 18–178 days) in the control group (P=not significant). Female gender was prevalent in both groups (65% for treatment and 56% for the control group; P=.95). Mean weight was 4.3±1.5 and 4.3±4.3kg, respectively, for the STAB and control groups (P=.95). There were no significant differences between the groups with regard to surgical indication (P=.819) or need for additional gastrostomy (P=.709). Mean operative time was shorter in the STAB group than in controls (34.6±6.1 versus 70.8±7.1 minutes; P<.001), which constituted a 50.7±9.1% absolute reduction. Open conversion (n=3, 14.3%) only occurred in the controls because of bowel loop lacerations during surgical manipulation that required surgical revision and in 1 case intraoperative suturing. There were no additional intraoperative complications. Time to oral feeding was also shorter in the STAB group (15.2±5 versus 23.4±11 hours; P=.003). There were no added in-hospital or late (at 1- and 4-week follow-up) complications.
Discussion
It is common in adult and/or pediatric surgery to face severely distended bowels during laparoscopy, impairing the surgical view and precluding safe surgical manipulation. In most cases, the operators opt for a conservative approach (moving the distended loop away from the visual field or just accepting suboptimal visualization), whereas others simply convert to open surgery. For many years, the surgical community has been reluctant to puncture the colon because of the expected risk of peritoneal spill of colonic contents as well as gas resulting in peritonitis.
In a previous study, 14 patients who were scheduled for an interventional radiology procedure (i.e., gastrostomy or gastrojejunostomy tube insertion, liver biopsy, or cholangiography) underwent STAB. The technique in that study, however, varies from our report because bowel puncture was guided radioscopically and correct placement was confirmed with contrast material. The authors punctured the transverse colon in 12 cases and the small intestine in 2, without experiencing complications related to the STAB procedure.8,9
In line with this radiological study, we found that in a selected population of pediatric patients undergoing laparoscopic Nissen fundoplication, in whom severe colonic distension was observed, the adjunctive use of STAB was feasible, safe, and effective. In all cases, targeted bowel loops were successfully deflated, allowing for a safe access and an optimal surgical view. Furthermore, we performed 45 punctures in unprepared bowels, which took from 2 to 5 minutes, time that was considered in the overall surgical time, without any signs or symptoms of peritoneal spill or any other complications. In this regard, it was possible to successfully decompress all of the bowels.
Most likely, the absence of complications is because of the small puncture site, which tends to seal immediately when the needle is withdrawn. Still, postprocedural surveillance for signs of peritonitis remains essential after STAB. Patients remained in the hospital from 3 to 5 days and began oral feeding without evidence of complications. In contrast to the encouraging results of the STAB maneuver, conventional maneuvers were associated with bowel loop laceration and the need for conversion to open surgery.
It is important that performing STAB dramatically reduced surgical time (primary end point) compared with the use of more conventional maneuvers against colonic distension. Reduction in surgical time is of the essence because prolonged surgeries are usually at risk for infection and metabolic derangements. The presence of more than 50% reduction in surgery time with STAB suggests that this maneuver is simple and efficient and, thereby, reproducible.
Study limitations
Our data need to be interpreted in light of the following: owing to the limited sample size, the study was only powered for the comparison of surgical time and not for robust clinical outcomes assessment. In addition, the study comprised infants with severe gastroesophageal reflux disease undergoing a laparoscopic Nissen fundoplication, and therefore our results should not be generalized to other subsets of patients or different laparoscopic procedures. Nonetheless, the present study may be considered hypothesis-generating for other surgical settings.
In addition, the conversion rate was high (14.3%) in small infants with severe colonic distension from the control group. Such conversion rate was concordant with a large Australian experience with the laparoscopic Nissen procedure (12%), which was eventually lowered to 2%. Consequently, conversion rates can be minimized with increasing levels of experience performing these operations. In this regard, we cannot exclude a potential bias from possible interindividual differences in surgical skill and experience that could have affected surgical time results; however, all procedures were performed by senior staff members.
Conclusions
We propose the use of STAB as alternative therapy to decompress a dilated large-bowel loop during laparoscopic surgery. This maneuver is simple and efficient and has no clinical complications. Future studies are warranted to evaluate its role in other subsets of patients or procedures as well as the safety of STAB in dilated small-bowel loops.
Footnotes
Acknowledgments
We appreciate the cooperation of Dr. Martinez Ferro and Dr. Mariano Albertal in the revision of this article.
Disclosure Statement
No competing financial interests exist.