
Abstract
Abstract
Background:
With increasing laparoscopic surgery experience and improved new vessel-sealing equipment, single-incision laparoscopic surgery (SILS) for splenectomy has emerged as an alternative to multiport laparoscopy, but the application of SILS for splenomegaly is still challenging due to technical difficulties. The aim of this study was to describe the suture suspension technique contributing to SILS for hereditary spherocytosis (HS).
Materials and Methods:
A retrospective review was conducted to evaluate all SILS for splenomegaly performed by a single surgeon. On preoperative ultrasonography, the spleen size index ranged from 0.67 to 0.82. An umbilical incision was used for the placement of a multichannel single port. To provide excellent exposure of the splenic hilum, a needle with a 1-0 suture was percutaneously introduced from the left hypochondriac region and then penetrated out the anterior chest wall for suspending the enlarged spleen. Dissection was facilitated by the use of a 5-mm curved reusable grasper and a 5-mm Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH), and the splenic vessels were ligated with 5-mm Weck® Hem-o-lok® clips (Teleflex®, Morrisville, NC). The resected spleen was placed in an endosurgical bag, morcellated, and removed from the abdomen via the umbilical incision.
Results:
Nine children underwent SILS during the study period without conversion to open procedures or requiring additional ports. The suture suspension technique was successfully used and markedly improved the exposure of the splenic hilum. The operative time was 122.6±31.2 minutes, and the extracted spleen weight was 562±74.5 g (range, 420–1260 g). No intraoperative or postoperative complications were recorded. The umbilical incision healed well with a satisfactory cosmetic effect.
Conclusions:
Our outcome shows the suture suspension enables safe and feasible usage of SILS for the management of splenomegaly in children with HS. More experience is needed to assess advantages and disadvantages compared with the standard laparoscopic approach.
Introduction
L
Materials and Methods
Patients
Between June 2010 and December 2013, SILS was mainly performed instead of conventional multiport LS for HS with enlarged spleen except in 4 patients with massive splenomegaly defined as extension of the splenic margin below the umbilicus or to the right of the midline, and they were excluded because SILS for a huge spleen has generally been found to fail in children.
In this study, nine children with moderate splenomegaly underwent SILS for splenectomy using the suture suspension technique performed by a single surgeon. There were five boys and four girls, with a mean age of 6.8±2.3 years (range, 5–12 years). The preoperative diagnosis and indication for splenectomy were established by a pediatric hematologist. All patients received standard preoperative immunizations and perioperative antibiotic prophylaxis. 8 Institutional review board approval was obtained, and the parents gave informed consent for the procedure. Preoperative abdominal ultrasonography or multidetector raw spiral computed tomography was done to assess the size of the spleen and the splenic vascular anatomy. 9 The spleen-size index ranged from 0.67 to 0.82 in our series. This index is a relationship between body weight and height and spleen size. 10 Normally, the spleen index should be <0.2, so the present values indicated that our patients had quite significant splenomegaly. The operative times, need for conversion, operative findings, length of hospital stay, and complications were reviewed.
Surgical technique
Patients were placed in the dorsal decubitus position with the left side elevated. The surgeon and the camera holder stood on the right side of the patient, with the tug-assistant on the opposite side of the patient. A transumbilical “Z” incision was created (similar to the “yin-yang” incision described by Dutta 11 ). The abdomen was entered under direct vision. A multichannel single port was placed through the incision (Fig. 1). A 5-mm 30° longer laparoscope with a right-angled light cord adaptor was used. In addition to a 5-mm straight standard Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH), 5-mm reusable curved laparoscopic instruments were used to facilitate the single-incision approach when necessary (Fig. 2), which allowed the surgeon to separate and stagger the hands in a small space with improved ergonomics.

The multichannel single port in the umbilicus.

A transumbilical single port allows three varied laparoscopic instruments to be manipulated and avoids clashing between instruments and hands.
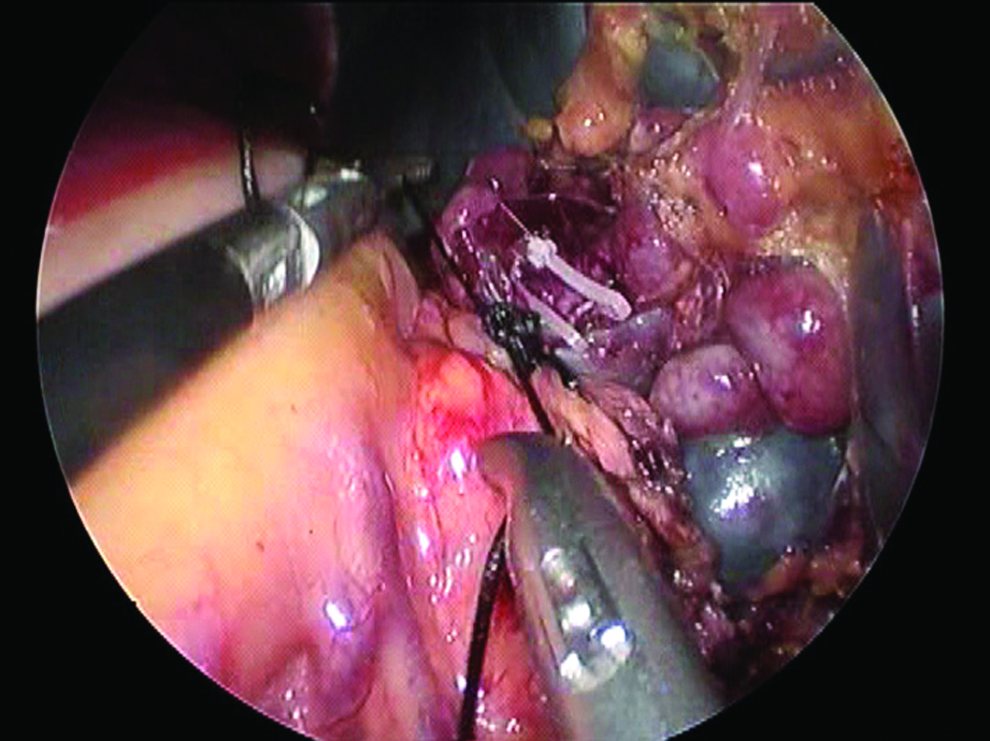
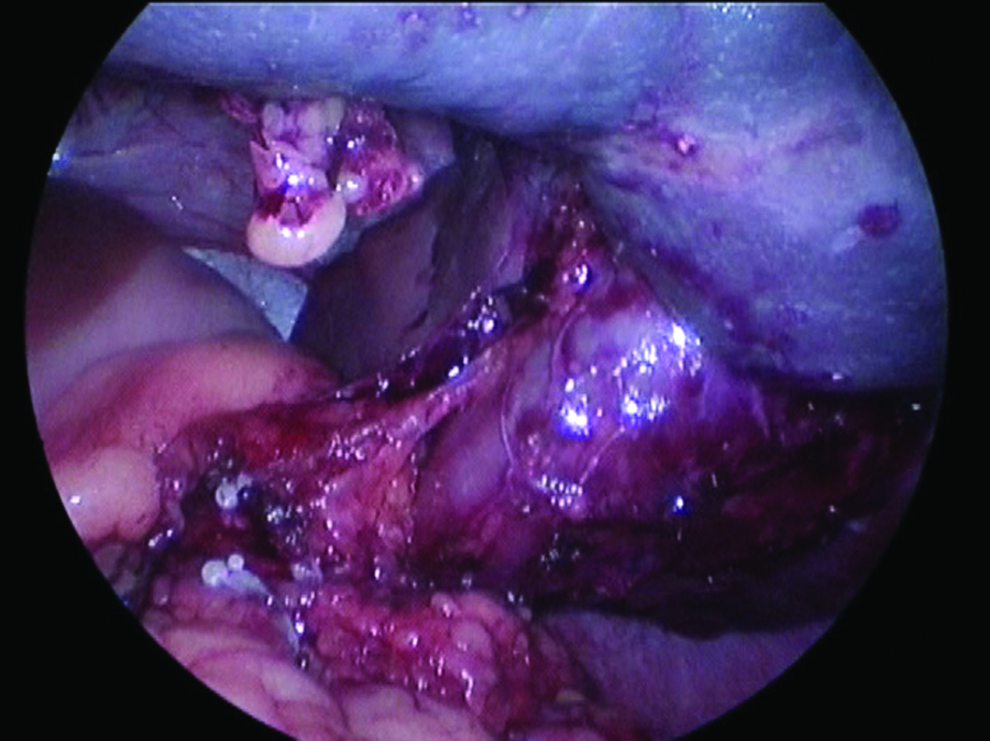
The overall procedures were similar to the standard LS. To facilitate exposure of the main vascular pedicle and the short gastric vessels, the splenomegaly was retracted with a traction suture placed around the lower pole of the spleen. A needle with a 1-0 polydioxanone suture was percutaneously introduced from the left hypochondriac region at the midaxillary line into the abdomen, encircled the inferior pole of the spleen, and then penetrated out from the anterior chest wall at the midclavicular line for suspending the enlarged spleen (Fig. 3). With the suture pulled both ends, the vascular pedicle was well visualized and isolated carefully, which allowed for progressive selective clipping of the main artery with a 5-mm clip applier (Fig. 4). The tail of the pancreas, which can lie very close to or even into the posterior splenic hilum, had to be mobilized if it existed (Fig. 5). After the artery was ligated, the splenic vein could be then dissected free and controlled with clips as well (Fig. 6), or a silk string was used to ligate the pedicle (Fig. 7).
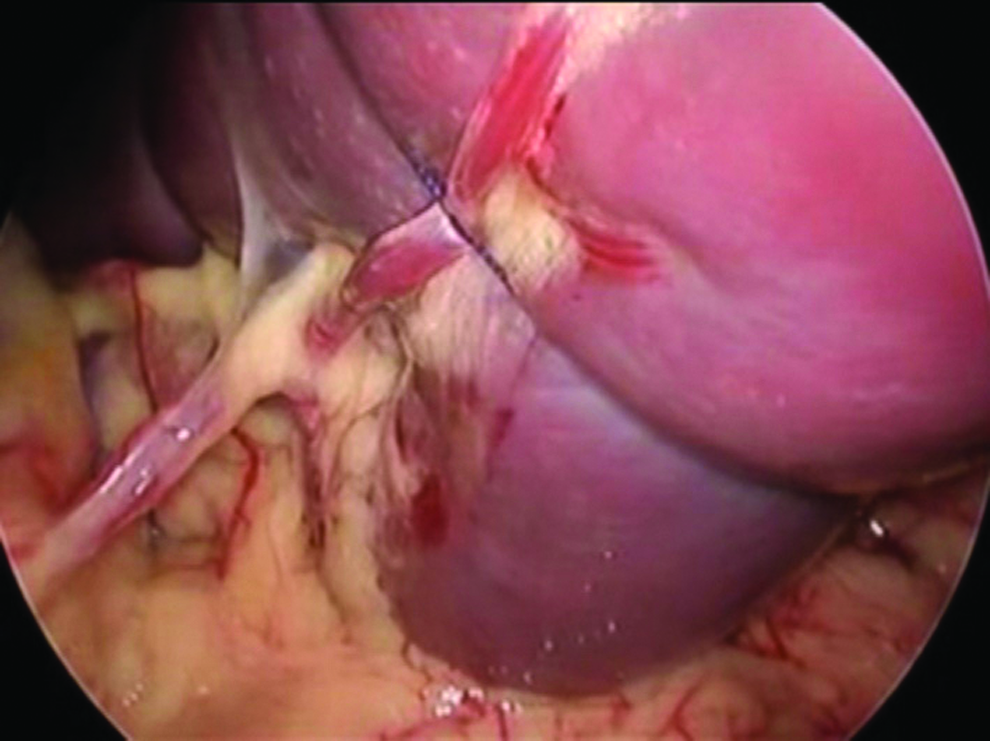
Lifting the lower pole of the spleen with a suture.
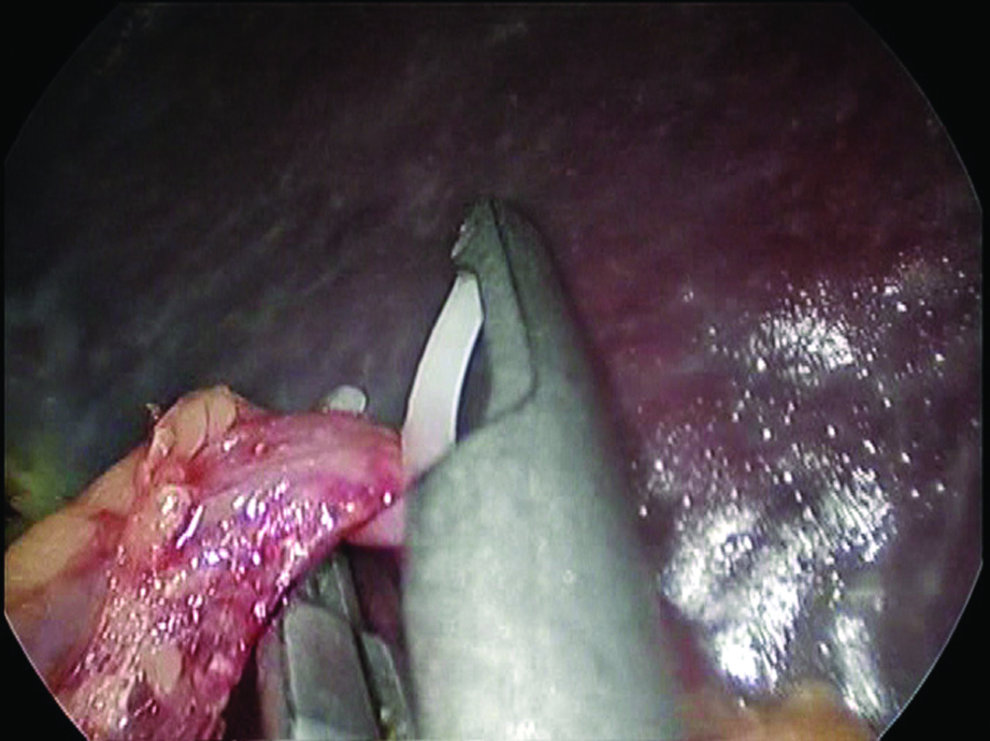
The splenic artery is clipped first.
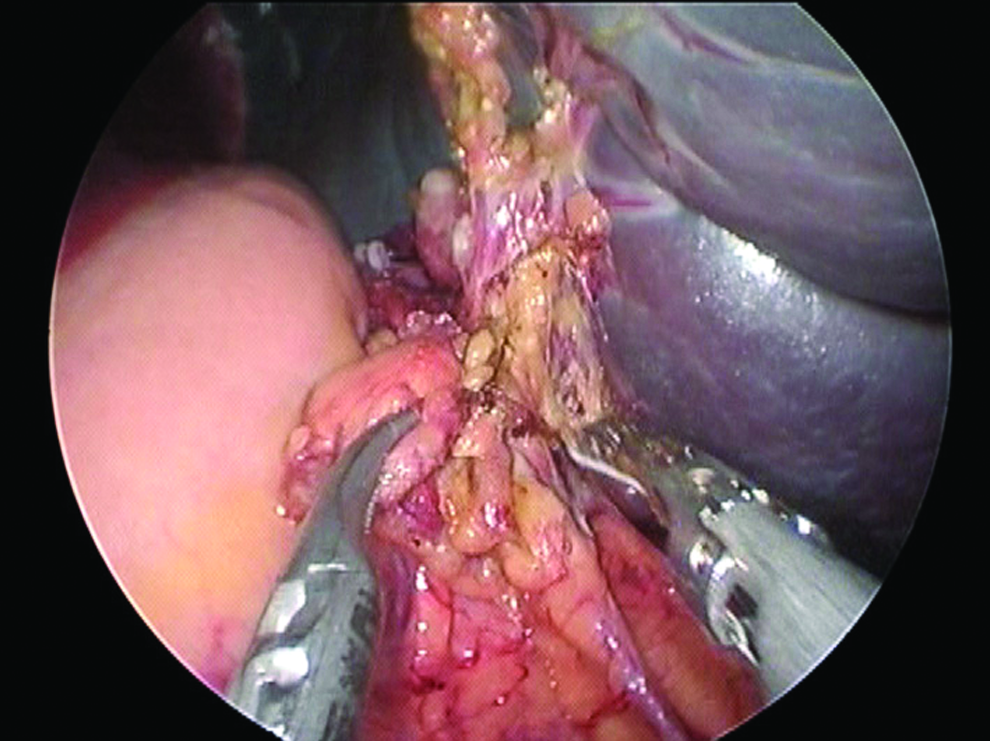
The pancreatic tail is dissected for better exposure of the splenic hilum.
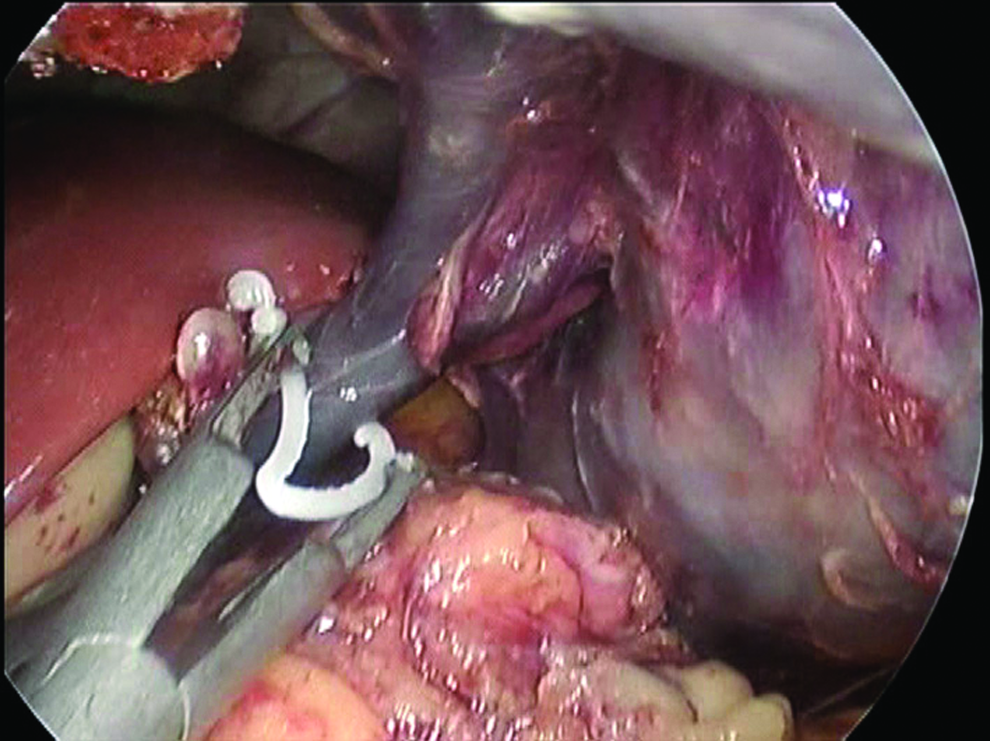
The splenic vein is clipped second.
The splenic pedicle is ligated using a suture.
After the hilar vessels had been divided by the use of the 5-mm Harmonic scalpel, the completely devascularized spleen was suspended by a small cuff of avascular superior pole splenophrenic attachments, which were divided in the end (Fig. 8). The resected spleen was placed in an endosurgical bag, morcellated, and removed from the abdomen via the umbilical incision (Fig. 9). After hemostasis was ensured, fascial defects were carefully closed with absorbable sutures, and the umbilical stump was reattached to the fascia.
The suspension technique also provides excellent exposure of the remnant ligaments.

Using a single port is helpful for specimen retrieval without the need to connect separate fascial incisions for multiple individual low-profile ports.
Results
In nine children with moderate splenomegaly SILS was successfully completed without conversion to open procedures or requiring additional ports. The suture suspension technique was used and markedly improved the exposure of the splenic hilum and the short gastric vessels. The average operative time was 122.6±31.2 minutes (range, 75–175 minutes), and the mean extracted spleen weight was 562±74.5 g (range, 420–1260 g). There were no intraoperative or postoperative complications. No patient received a blood transfusion for hemorrhage. The average hospital stay was 4.4±1.2 days. During a postoperative follow-up period of 5 months to 4 years, neither wound-related complications nor overwhelming postsplenectomy infection occurred. Children and parents were satisfied with the cosmetic outcomes, and all parents were amazed at the absence of any appreciable visible scar.
Discussion
HS is an autosomal dominant inheritance disorder. The main clinical features include hemolytic anemia, variable jaundice, and splenomegaly. Splenectomy is recommended for children with moderate to severe HS. It should also be considered for children with significant splenomegaly because of the risk for traumatic rupture. 8
LS is a well-accepted approach for HS with splenomegaly. With the evolution of laparoscopic techniques and instrumentation, the concept of minimally invasive surgery has progressed since the early 1990s from standard multiport LS to SILS for splenectomy. Recent studies have proved that the new technique can be a safe alternative to multiport laparoscopy; therefore it is becoming more and more popular. Since first being described in 2009, SILS for splenectomy has been described in a limited number of case reports and small case series,2–7 but no studies have evaluated single-incision splenectomy for considerable splenomegaly in children. We started our program of SILS in children without the availability of specially designed single-port devices or reticulating instruments. After we had successfully performed SILS in children with normal or slightly enlarged spleens, 12 we decided on using the suture suspension technique to perform SILS for our patients suffering from HS with a moderately enlarged spleen. Our results illustrate the feasibility of SILS for splenomegaly, and using the suture to suspend the enlarged spleen for operative visualization and splenic vascular pedicle dissection can be considered a safe technique.
The core surgical steps for SILS for splenectomy are very similar to the standard LS. The main differences are in the way the abdominal cavity is accessed, port placement, and the laparoscopic instruments that are used during the dissection. There is great variability in the umbilical configuration for each patient. However, we have found that it is usually possible to use the umbilical "Z" incision and achieve a very good to excellent cosmetic outcome. Many surgeons have described different ways of accessing the abdominal cavity through the umbilicus. In our experience, we prefer to use a multichannel single port, which allows multiple varied laparoscopic instruments to be worked simultaneously through separate flexible channels sited within its atrial valve. Using a multi-access port appeared to minimize fulcrum effects and facilitated specimen retrieval without the need to connect separate fascial incisions. The curved instruments helped to simulate triangulation as well, although several reports have been published demonstrating the feasibility of performing SILS with standard laparoscopic instruments. 5 We have found that using a longer laparoscope as well as instruments of different lengths prevents bothersome clashing between instruments and the hands of the surgeon and assistant.
In LS, bleeding from the splenic hilum is not only the most important complication, but also the most common reason for conversion to open surgery. 13 Therefore, a good exposure of the splenic hilum has to be considered as an essential step in SILS for splenectomy. However, in attempting SILS, no trocar is available for splenic hanging because the number of accesses is limited. Difficulty with retracting the spleen can be solved by the external traction suture placement. 14 In our series, a suture was placed percutaneously through the left hypochondriac region. By pulling the traction suture extracorporeally to lift the lower pole of the splenomegaly, the suture suspension technique could provide excellent exposure of the splenic hilum, the pancreatic tail, the splenic pedicle, and the short gastric vessels, thus facilitating their dissection. This technique is helpful for dissecting the remnant ligaments around the spleen as well. By suspending the enlarged spleen with our technique, an excellent exposure of the phrenosplenic ligament was also obtained.
Challenges in LS when significant splenomegaly is present arise from the decreased working space and the increased risk of bleeding due to large vessels. As with any new procedure, emphasis should be placed on patient safety. In our series, there were no intraoperative or postoperative complications attributable to SILS. Concerns regarding intraoperative safety in SILS for splenectomy focus on early ligation of the splenic artery. 15 In order to decrease splenic engorgement and lower the risk of bleeding in SILS for splenomegaly, we suggest first isolating and clipping the splenic artery. This step is essential to perform bloodless for the following procedures; it also provides some degree of autotransfusion and allows a partial reduction of the spleen volume. If the distal segment of the splenic pedicle is located behind the pancreatic tail, we must carefully remove the arterial sheath and separate the tail of pancreas first and then reveal and clip the splenic artery. 16 Because we used 5-mm Hem-o-lok clips to clamp the vessels or a silk string to ligate the pedicle, and then the main vessels were sectioned at the splenic hilum and not by a linear stapler, no enlargement of the incision was required. In addition, it should be noted that the suspending suture may perhaps bring about cutting the splenic capsule, so a thicker thread should be used for the traction technique. Of course, to avoid a possible cut and consequent bleeding, the tugging force should be controlled to prevent such an injury.
The major benefit of SILS in our series was that patients and parents were satisfied with the cosmetic outcomes, and all parents were amazed at the absence of any appreciable visible scar.
In conclusion, SILS with splenic hilar dissection for an enlarged spleen is feasible. Our preliminary experience shows the suture suspension technique that enables SILS is quite safe for the management of splenomegaly in children with HS. More experience is needed to assess advantages and disadvantages compared with the standard laparoscopic approach.
Footnotes
Disclosure Statement
No competing financial interests exist.