
Abstract
Abstract
Introduction:
Some degree of inadequate weight loss or recidivism is seen with all bariatric surgical approaches. To combat this, some authors have suggested placing a reinforcing ring around gastric bypass pouches or gastric sleeves. The aim of this study was to assess the initial feasibility and efficacy of silicone-banded laparoscopic sleeve gastrectomy (LSG).
Materials and Methods:
All cases of silicone-banded LSG performed at our center were retrospectively identified. Patient demographics, perioperative parameters, and postoperative outcomes were extracted and analyzed.
Results:
Thirteen patients (7 females, 6 males) were identified and analyzed. Preoperatively, patients had a mean age of 56.0±8.3 years, a mean body mass index (BMI) of 53.7±8.5 kg/m2, and a median of seven comorbidities. All cases were completed laparoscopically by one surgeon, with a mean operative time of 140.7±25.7 minutes and a mean estimated blood loss of 56.9±30.6 mL. There were no mortalities. The only intraoperative complication was a respiratory arrest after extubation, and this patient recovered fully. Postoperatively, 2 patients (15.4%) experienced a complication: one had a pulmonary embolism requiring brief re-admission, and the other had a syncopal episode from a second-degree atrioventricular block. No long-term complications were encountered. One patient was lost to follow-up. At a median follow-up of 16 months (range, 6–27 months), the mean BMI of the cohort was 38.7±7.9 kg/m2, which corresponded to a mean excess weight loss (EWL) of 54.8±19.6%.
Conclusions:
This report provides initial evidence that silicone-banded LSG is feasible and can be performed with minimal morbidity and significant EWL at short-term follow-up.
Introduction
I
Laparoscopic sleeve gastrectomy (LSG) is rapidly emerging as a popular primary bariatric procedure, especially in the superobese or those with high perioperative risk. Studies continue to suggest that LSG is an effective approach to weight reduction and comorbidity improvement.4–7 However, LSG also suffers from an inherent degree of inadequate weight loss and recidivism, postulated by some to be caused by sleeve dilation over time. Using the same principles that govern the banded Roux-en-Y gastric bypass (RYGB) approach, some surgeons have reported preliminary experiences placing various types of reinforcement material around the gastric sleeve to promote superior weight loss and minimize the effect of gastric sleeve dilation over time.8–14 Unfortunately, there are few data addressing this novel approach. The aim of this study was to assess the feasibility and short- to medium-term outcomes of nonadjustable silicone-banded LSG.
Materials and Methods
After Institutional Review Board approval was obtained, we retrospectively identified all cases of silicone-banded LSG performed at our center. Patient demographics, perioperative parameters, and postoperative outcomes were extracted and analyzed. Patient demographics identified included age, sex, height, weight, body mass index (BMI), associated comorbidities, medications, number and type of previous abdominal surgeries (including bariatric), and American Society of Anesthesiologists score. Operative parameters extracted included operative time, estimated blood loss, intraoperative events, and complications. Perioperative outcomes used were length of stay, complications, need for re-admission, duration of follow-up, postoperative gastroesophageal reflux disease (GERD) parameters (subjective reflux, antireflux medications, objective studies), weight, BMI, and complications at follow-up. These data were then used to calculate the percentage of excess weight loss (EWL) of the cohort. The EWL was defined as the operative weight minus the follow-up weight, divided by the excess weight, multiplied by 100. Excess weight was defined as the operative weight minus ideal body weight based on a BMI of 25 kg/m2. Categorical variables were reported as frequencies (%). Continuous variables with normal and non-normal distributions were presented as mean±standard deviation and median (range), respectively.
Operative approach
The set-up and trocar placement for sleeve gastrectomy have previously been described. 15 After liver retraction, the greater curvature of the stomach from the angle of His down to the pylorus is mobilized by dividing omental attachments. A green load (Echelon Endopath™; Ethicon, Somerville, NJ) of the stapler is then applied about 4 cm from the pylorus parallel to the lesser curvature. Next, we pass the flexible endoscope (or 34-French bougie) down the esophagus along the lesser curvature of the stomach and into the pylorus. Two or more applications of the stapler (green load) are then fired parallel to the endoscope, and then multiple blue loads (Echelon Endopath) are applied parallel to the endoscope up toward the angle of His. The excised gastric specimen is placed in a sterile bag and removed through the right upper quadrant port site. The staple line is oversewn in an invaginating fashion from the angle of His to the end near the pylorus.
An 8-French, 4-inch (10.16-cm) medical-grade silicone tubing is then used to reinforce the resulting gastric sleeve. The ring is created on the back-bench in the operating room under sterile technique by inserting 2-0 silk suture (8 cm) on either end to facilitate closure of the ring. The suture is secured to the tubing by passing the suture needle through the tubing and then wrapping the suture around the tubing and tying it in place. Each suture is placed 6.5 cm apart and approximately 1.8 cm from each end (Fig. 1). A tunnel is created posterior to the stomach 1–2 cm inferior to the esophagogastric junction (Z-line) and superior to the pars flaccida. The tubing is then passed through the tunnel, and both ends are brought anteriorly and placed side by side to create a circular, 6.5-cm-circumference, wrap around the proximal stomach (Fig. 2). Clips are placed to hold the tubing in place while the silk sutures are tied together at the 12 o'clock position as an endoscope or 34-French bougie remains in place in the stomach (to ensure lumen size). Seromuscular sutures are placed at the 10 and 2 o'clock positions (Fig. 3).

Back-bench creation of the ring from 8-French medical-grade silicone tubing.
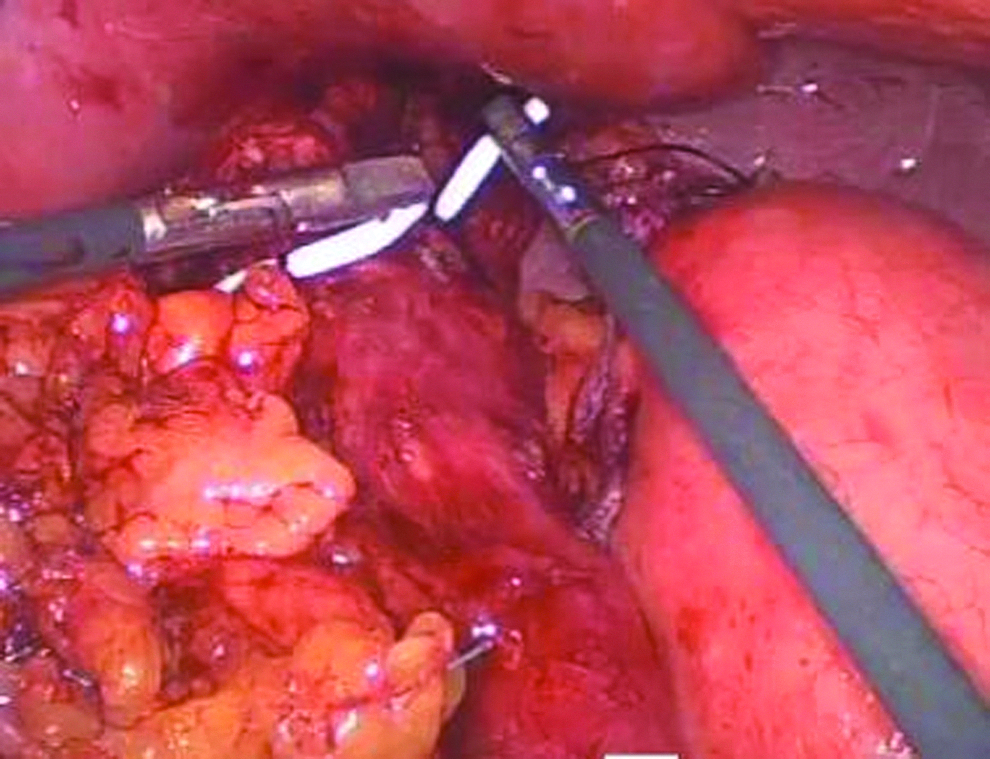
The tubing is passed through the posterior tunnel, and both ends are brought anteriorly and placed side by side to create a circular (6.5-cm-circumference) wrap around the proximal stomach.
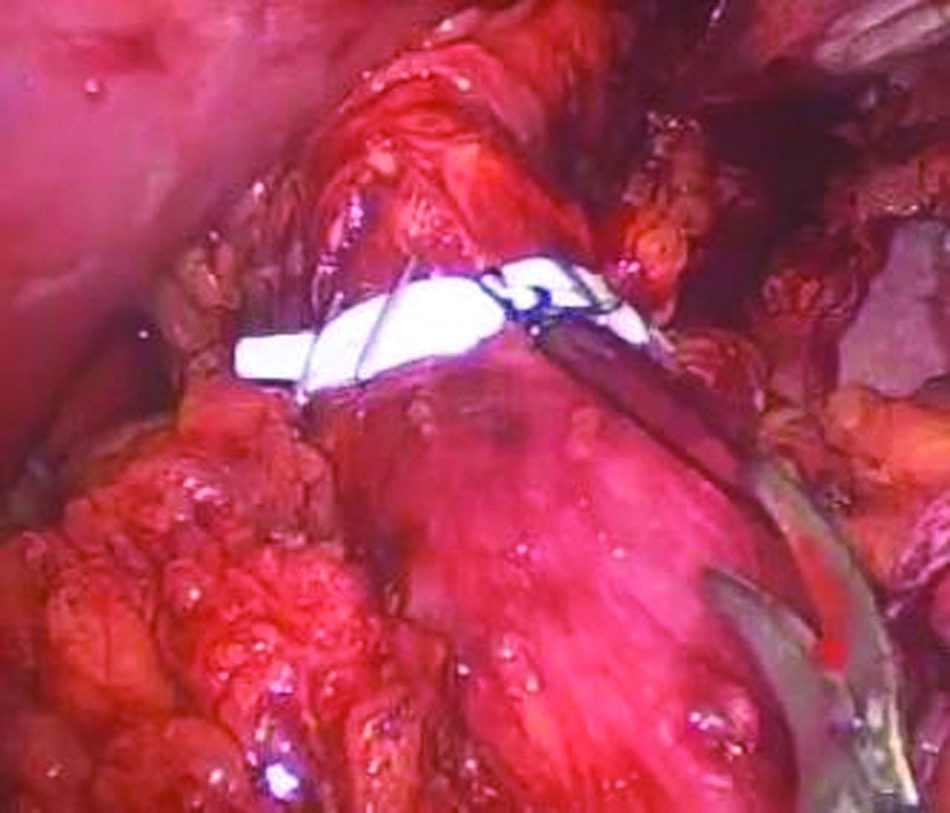
Final ring placement 1–2 cm inferior to the esophagogastric junction (Z-line) and superior to the pars flaccida.
Results
In total, 13 patients (7 females, 6 males) were retrospectively identified and analyzed. Preoperatively, patients had a mean age and BMI of 56.0±8.3 years and 53.7±8.5 kg/m2, respectively. The cohort had a median of seven comorbidities (range, 1–12), a median American Society of Anesthesiologists score of 3, and 46.2% (n=6) had previous abdominal surgery. Two patients (15.4%) did report preoperative GERD symptoms: one with mild reflux without the need for antireflux pharmacotherapy, and the other with moderate reflux on daily omeprazole. Neither patient had objective studies confirming reflux before surgery.
All cases were primary bariatric procedures, and all were completed laparoscopically by one surgeon without the need for conversion to laparotomy. The mean operative time and estimated blood loss were 140.7±25.7 minutes and 56.9±30.6 mL, respectively. The only operative complication was a respiratory arrest after extubation, which did require cardiopulmonary resuscitation, re-intubation, and a brief intensive care unit stay (the patient recovered fully). There were no mortalities.
Postoperatively, 2 patients (15.4%) experienced a complication: one had a pulmonary embolism requiring brief re-admission 2 weeks postoperatively, and the other had a syncopal episode from a second-degree atrioventricular block during the primary admission (resolved without the need for invasive intervention). No other complications were identified in this cohort. One patient was from overseas and was lost in follow-up. Of the remaining subjects, the proportions achieving 12, 16, and 24 months of follow-up were 9 (75.0%), 7 (58.3%), and 4 (33.3%), respectively. At a median follow-up of 16 months (mean, 16.8; range, 6–27), the mean BMI of the cohort was 38.7±7.9 kg/m2, which corresponded to a mean EWL of 54.8±19.6%. Seven (58.3%) patients achieved an EWL of ≥50%; 10 (83.3%) subjects had EWL of ≥40%. Recurrent emesis and dysphagia were absent in the cohort. The patient with preoperative GERD necessitating daily omeprazole experienced subjective improvement of reflux symptoms and was off medication at follow-up; the patient with mild reflux reported no change in GERD symptoms. Two of the subjects without preoperative subjective/objective evidence of GERD did experience mild reflux at follow-up (one without the need for antireflux pharmacotherapy, the other on daily famotidine). Dietician assessment revealed intolerance to meat (mild) in one patient. There were no other complications identified at the median follow-up period of 16 months.
Discussion
The sleeve gastrectomy procedure was originally devised as a first step in the staged duodenal switch for severe obesity, as described by Hess and Hess 16 and Marceau et al. 17 Many patients were enjoying substantial weight loss and improvement of obesity-related comorbid conditions after the first stage, and this led to consideration of LSG as a primary procedure. The popularity of LSG continues to grow, especially in the superobese and those with substantial perioperative risk, as it offers significant weight reduction potential and a morbidity/risk profile positioned between laparoscopic RYGB and laparoscopic adjustable gastric banding. 4
Despite the recent surge in popularity, LSG is not without its complications and nonresponder rates. Much like RYGB and laparoscopic adjustable gastric banding, LSG suffers from an inherent degree of inadequate weight loss or recidivism, a phenomenon seen in all bariatric approaches and accentuated in the superobese.18,19 While the exact cause of therapeutic nonresponse is unknown, many postulate it is related to inadequacy or dilation of the gastric sleeve and the resulting decrease in restriction over time. To combat this, some surgeons have suggested placing either adjustable or nonadjustable material over the gastric sleeve at the primary operation, an approach extrapolated from ever-growing data and experience with primary and salvage-banded RYBG.8–14
There is at least one case report of adding a laparoscopic adjustable band to a failed sleeve gastrectomy in a patient unable to undergo malabsorptive surgery with good results. 20 Unfortunately, there are few data regarding primary banded LSG, with significant variation in operative approaches (and material used) among the few published reports. Agrawal et al. 8 first proposed laparoscopic adjustable banded sleeve gastrectomy as a stand-alone procedure in their case report of a 39-year-old super-superobese patient. Karcz et al. 9 subsequently described their technique of banded LSG using the prefabricated GaBP Ring Autolock™ (Bariatec Corp., Palos Verdes Peninsula, CA) system to calibrate the sleeve and prevent distal dilation. Alexander et al. 10 published results on 27 patients who underwent biologic tissue (AlloDerm®; LifeCell, Bridgewater, NJ)-banded LSG with at least 3 months of follow-up. This group was compared with 54 patients who had standard RYGB matched for age, sex, and BMI. The study found no difference in comorbidity resolution (resolution or improvement in all patients in both groups) or BMI reduction between the groups, and the authors theorized that the approach could avoid the potential long-term complications of malabsorptive procedures. It should be noted that this report did include one case of presumed staple-line leak and subsequent subphrenic abscess, but there were no mortalities in the series. 10
To our knowledge, there are only two studies that have addressed outcomes of primary nonadjustable silicone-banded LSG. Miguel et al. 11 first reported results after 33 consecutive cases (females only) of a 6.5-cm silicone ring–banded LSG. At 12 months of follow-up, the cohort achieved a mean EWL of 86.5±14.2%, and resolution of diabetes/glucose intolerance was observed in all patients. They did report two (6%) staple-line leaks: 1 patient survived after re-operative gastrectomy, and the other died. 11 Recently, Karcz et al. 12 published retrospective data comparing 25 banded LSG cases using a European-made prefabricated nonadjustable product called the MiniMizer® (Bariatric Solutions GmbH, Stein am Rhein, Switzerland) ring (not yet available in the United States) with previously performed standard LSG cases. At 12 months of follow-up, there was no significant difference in the EWL achieved by the two approaches, but the MiniMizer ring group did experience more postoperative emesis. However, this comparative analysis was matched 1:1 retrospectively, and comparative results must be interpreted accordingly. The banded group did require more postprocedural revisions (n=3), and this is a potential drawback of the banded LSG approach. 12
In the present study, we report significant mean EWL (54.8±19.6%) without mortality and only minimal morbidity at a median follow-up of 16 months. The results are more modest than those reported by Miguel et al., 11 but their mean EWL is rather high for a primary bariatric procedure. The one intraoperative complication (respiratory arrest postextubation) and two postoperative complications (pulmonary embolism and syncopal episode) were more related to the inherent perioperative risk of operating on the morbidly obese and not the technical approach. One patient was lost to follow-up, but this was an international patient who was flown back overseas after discharge who has not been contacted despite multiple attempts.
We believe that the greatest potential benefit of this approach may be in the weight loss achieved at long-term follow-up with potential reduction in recidivism rates, but this can only be assessed with longer follow-up, an obvious limitation of this study. Other limitations included retrospective design, small case number, and the fact that it is a single-surgeon, single-center study. Further prospective and comparative research is needed to assess the efficacy of primary banded LSG and its effect on obesity-related comorbidities. Furthermore, an attempt to standardize silicone-banded LSG using prefabricated medical-grade rings may potentially reduce surgeon-to-surgeon variability and associated complications. Although the efficacy and safety of the “back-table” nonadjustable silicone ring appear promising, a standardized approach to this novel procedure could eliminate heterogeneity in both application and outcomes.
Conclusions
This report provides initial evidence that silicone-banded LSG is feasible, with minimal morbidity and significant EWL at short-term follow-up. Further longer-term prospective comparative studies are needed to better assess this adjunctive procedure that aims to combat ineffective weight loss and recidivism. Furthermore, a more standardized approach to ring reinforcement should be explored to potentially eliminate heterogeneous outcomes derived from back-bench/surgeon-fabricated rings.
Footnotes
Disclosure Statement
No competing financial interests exist.