
Abstract
Abstract
Gastrocutaneous fistula (GCF) occurs commonly in pediatric patients after removal of long-term gastrostomy tubes. Although open repair is generally successful, endoscopic approaches may offer benefits in terms of incisional complications, postoperative pain, and procedure time. In addition, endoscopic approaches may offer particular benefit in patients with varied degrees of skin irritation or erosion surrounding a GCF, making surgical repair difficult, or patients with significant comorbidities, making minimal intervention and anesthesia time preferable. Over-the-scope (OSC) clips are a new technology that enables endoscopic closure of intestinal fistulas up to 2 cm in diameter. Six pediatric patients underwent endoscopic GCF closure using OSC clips under Institutional Review Board approval. The procedure was technically successful in 5 of 6 cases with an average operating time of 29 minutes. The technical failure required an open revision, whereas all other patients reported full healing of the GCF site at 1 month. All successful cases were performed as outpatients without postoperative narcotics. In addition, all patients reported high satisfaction with the procedure and cosmetic results. Endoscopic GCF closure using an OSC clip is technically feasible in the pediatric population. Based on limited cases with a 1-month follow-up, the functional and cosmetic results of technically successful cases are excellent. Endoscopic GCF closure is a potential alternative to standard surgical closure in patients with skin irritation or erosion and/or significant comorbidities.
Introduction
O
Open incision with gastric repair and fascial closure is the standard technique for treatment of a persistent GCF. Open repair has a high success rate; however, local wound complications such as infection and dehiscence may occur, predisposing the patient for a recurrence of the fistula. With the ongoing development of endoscopic interventions, multiple techniques have been described for the closure of persistent GCFs in the adult population. Endoscopic banding was reported to be successful in 3 of 4 patients. 4 Cauterization of the GCF tract with placement of standard endoscopic clips was reported to be successful in 4 of 5 patients. 5 Over-the-scope (OSC) clips have been designed to enable closure of intestinal wall defects up to 2 cm in diameter (Fig. 1). 6 The clips are made of nitinol and loaded in a cap onto the end of an endoscope (Fig. 1). A trigger mechanism runs through the working channel to deploy the clip. The shape-memory metal enables the clips to spring closed, similar to a bear trap, resulting in the encircling and compression of tissue (Fig. 2). Evolving endoscopic technology may enable safer, faster, and more reliable endoscopic closure of GCFs. Endoscopic GCF closure is anticipated to offer the standard advantages of minimal access/natural orifice surgery, including reduced postoperative pain and wound complications. In addition, this approach may offer particular benefit in patients with varied degrees of skin irritation or erosion surrounding a GCF, making surgical repair difficult, or patients with significant comorbidities, making minimal intervention and anesthesia time preferable.

Over-the-scope clip system.
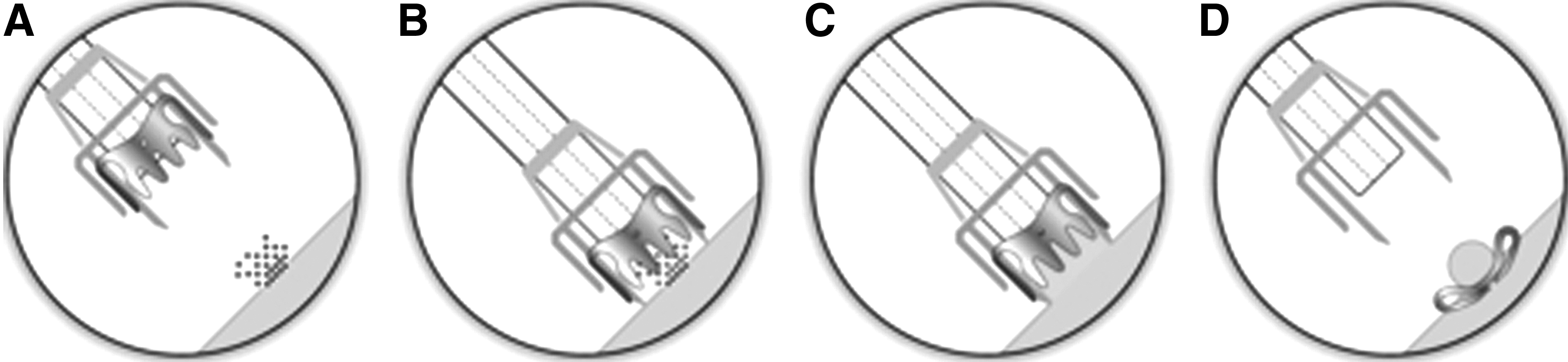
Use of the over-the-scope clip system for gastrocutaneous fistula closure:
Patients and Methods
Institutional Review Board approval (IRB #29689) was received to perform endoscopic GCF closure in the pediatric population using an OSC clip. GCF was defined as persistent leakage from the gastrostomy site after 1 month of nonoperative management. When a gastrostomy tube is removed in our practice, the site is typically cauterized with silver nitrate, and an occlusion pressure dressing is applied. In addition, a barrier cream may be applied to the surrounding skin to prevent skin breakdown from any gastric content leakage. An acid suppression medication is prescribed to decrease the effect of leakage. The family is instructed on providing small frequent meals throughout the day and to avoid carbonated beverages. Patients are seen after 1 month of nonoperative management and offered closure if there is a GCF. The target population for this study included patients at higher risk for open closure that might benefits from the endoscopic approach. Higher-risk patients were defined as having either skin irritation or erosion around a persistent GCF or significant comorbidities.
All procedures were performed in the operating room using a GIF-H180 high-definition gastroscope with a single 2.8-mm working channel (Olympus, Center Valley, PA). The internal opening of the GCF was identified on diagnostic endoscopy (Fig. 3A). A gold probe bipolar hemostasis catheter (Boston Scientific, Natick, MA) was used to cauterize the GCF tract from the inside (Fig. 3B). The OSC clip system was press-fit onto the end of the endoscope and delivered to the stomach. A reusable 2.8-mm or 2.0-mm alligator grasper (Olympus) was used to grasp the GCF and pull it into the cap of the OSC clip. The first case was performed with a Padlock Clip (Aponos, Kingston, NH), and the subsequent 5 cases were performed with the OVESCO 11/3-mm t-type clip (Ovesco Endoscopy AG, Tübingen, Germany).
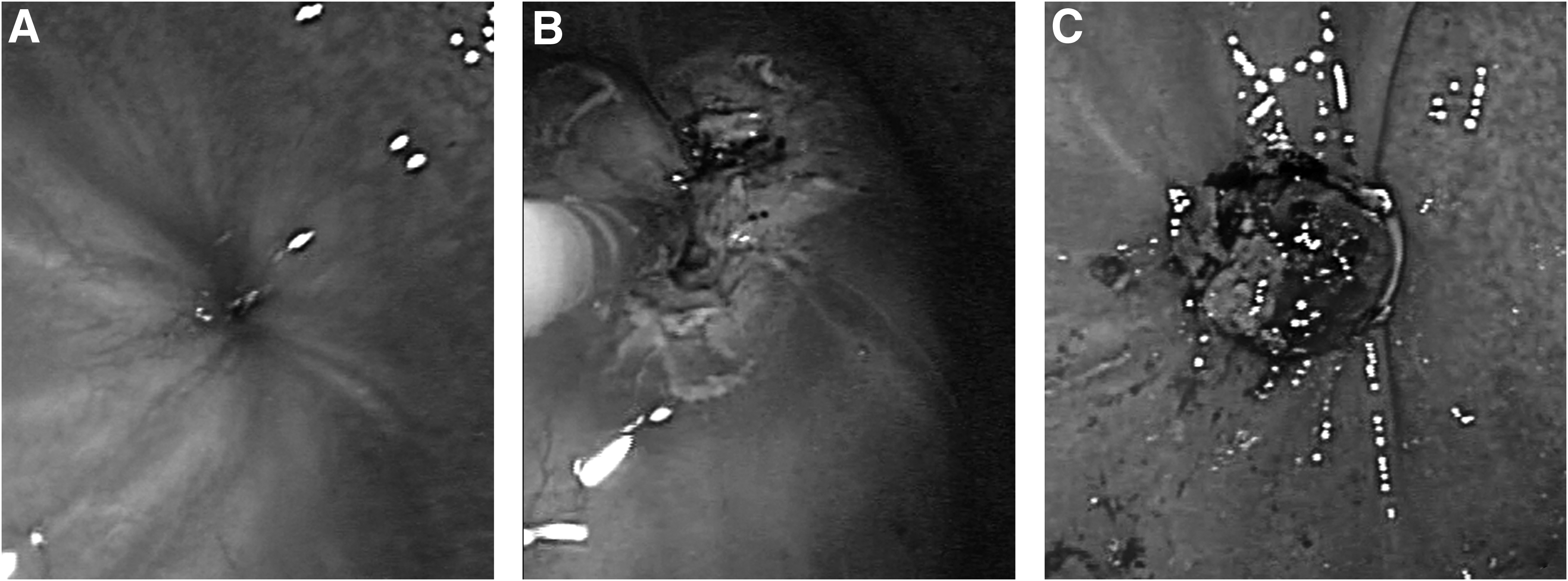
Endoscopic view of
At 1 month postclosure, the patients returned for a follow-up visit to assess leakage and pain. At the follow-up, patients also completed a questionnaire focused on functional and cosmetic satisfaction. All patient data were stored in RedCAP.
Patients' characteristics
The average age was 10.7 years (standard deviation=6.3; range, 5–22). The average weight was 32.97 kg (standard deviation=20.71; range, 13.1–66.4 kg). All patients had skin irritation or erosion and/or significant comorbidities that increased the risk of open GCF closure (Table 1).
Results
Endoscopic GCF closure was technically successful in 5 of 6 cases. The average operating time was 29 minutes, with the most recent case taking 16 minutes. All successful cases were sent home on the day of surgery. The technical failure was due to a clip deployment that did not completely cover the internal fistula opening. An attempt was made to salvage this case by placing standard through-the-scope Resolution clips (Boston Scientific) over the residual defect, and the patient was monitored for 1 day in the hospital. The patient had significant decrease in fistula output that enabled resolution of skin irritation and erosion. However, the GCF site continued to leak at 1 month after endoscopic closure so open closure was offered.
One-month follow-up was completed in all 5 patients in whom the procedure was technically successful. Minor leakage from the external GCF site that resolved at a maximum of 2 weeks was reported by 3 patients. One patient had mild discomfort with swallowing in the first week postoperatively that was self-limited. With regard to cosmetic satisfaction, 4 patients reported their scars remained dimpled at 1 month. One patient was not completely satisfied with the residual dimple, but no patients desired scar revision. Three patients required no postoperative pain medication, whereas 2 patients took acetaminophen only in the immediate postoperative period.
Discussion
Endoscopic GCF closure using an OSC clip is technically feasible in the pediatric population. The current size of the OSC systems requires at minimum a 9-mm-diameter endoscope with a cap that adds additional diameter and limits the use of this device in small children. In addition, the cap extends between 3 mm and 6 mm beyond the tip of the endoscope. Although a longer cap has benefits in accommodating more tissue under suction to be clipped, it is more difficult to navigate through the oropharynx of small children. OSC clips are more expensive that standard endoscopic clips; however, the cost becomes relatively equivalent if one OSC clip can be used in place of a few standard clips.
Existing OSC clips cannot be repositioned. The one technical failure was due to a malpositioned clip that did not fully cover the internal GCF orifice. Standard endoscopic clips were partially successful in salvaging this procedure in that the fistula output was decreased enough to allow resolution of skin irritation or erosion prior to open revision.
Overall satisfaction with the procedure was high. The single case of self-limited postoperative throat pain was likely due to trauma from the manipulation of the system through the oropharynx. The minimal postoperative leakage that resolved in the early operative period was likely from residual secretion of the mucosa above the closure.
Conclusions
Endoscopic GCF closure is technically feasible in the pediatric population weighing over 10 kg. The inability to reposition OSC clips is a limiting factor that could potentially be solved in future generations of this technology. Based on a limited case number with 1-month follow-up, the functional and cosmetic results of technically successful cases are excellent. Endoscopic GCF closure is a potential alternative to standard surgical closure in patients with skin irritation or erosion and/or significant comorbidities.
Footnotes
Acknowledgments
RedCAP was funded by the Stanford CTSA award number UL1 RR025744 from the National Center for Research Resources, National Institutes of Health.
Disclosure Statement
No competing financial interests exist.