
Abstract
Abstract
Objective:
Endoscopic thoracic sympathectomy or sympathicotomy, for the treatment of palmar, axillary, and plantar hyperhidrosis, is generally performed at one or two levels, between T2 and T5. Compensatory sweating (CS) is a severe and undesirable side effect of this procedure. Here, we describe the success of treatment and degree of postoperative CS in sympathicotomy patients.
Subjects and Methods:
This study included 80 patients treated by uniportal (5-mm) thoracoscopic sympathicotomy (electrocautery) for primary hyperhidrosis over a 6-year period (2007–2013). Sympathicotomy was performed bilaterally at T2 for blushing (n=2), T2–T3 for palmar-only hyperhidrosis (n=34), T2–T4 for palmar and axillary hyperhidrosis (n=39), and T3–T4 for axillary-only hyperhidrosis (n=5). Outcome was assessed 2 weeks postsurgery at the clinic and annually thereafter by telephone questionnaire. Mean follow-up time was 35.2±23.3 months. Questionnaires assessed patients' degree of sweating, postoperative CS, overall satisfaction, and complications.
Results:
Seventy-one patients (88.7%) were very satisfied, whereas only 9 (11.3%) were dissatisfied with the procedure. Complication incidence was 7.5%, and CS occurred in 77.5% of patients. Therapeutic success rate was 97.5%; complete relief of hyperhidrosis was achieved in 72 (90%) patients, whereas 8 (10%) experienced recurrence.
Conclusions:
CS is a frequent side effect of thoracoscopic sympathicotomy. We recommend all patients undergoing this procedure should be warned of the potential risk of developing severe CS.
Introduction
I
Subjects and Methods
From July 2007 to November 2013, bilateral thoracoscopic sympathicotomy was performed for palmar and/or axillary hyperhidrosis in 80 patients. Forty-three patients were males, and 37 were females. Their median age was 22.75±5.57 (range, 13–39) years. The most frequent presenting complaint was palmar and axillary sweating in 39 (48.7%) patients, followed by palm alone in 34 (42.5%), axilla alone in 5 (6.2%), and blushing in 2 (2.5%). Thirty-five (43.7%) patients had tried different treatments (oral medications, botox injections, topical agents, iontophoresis) before undergoing surgery.
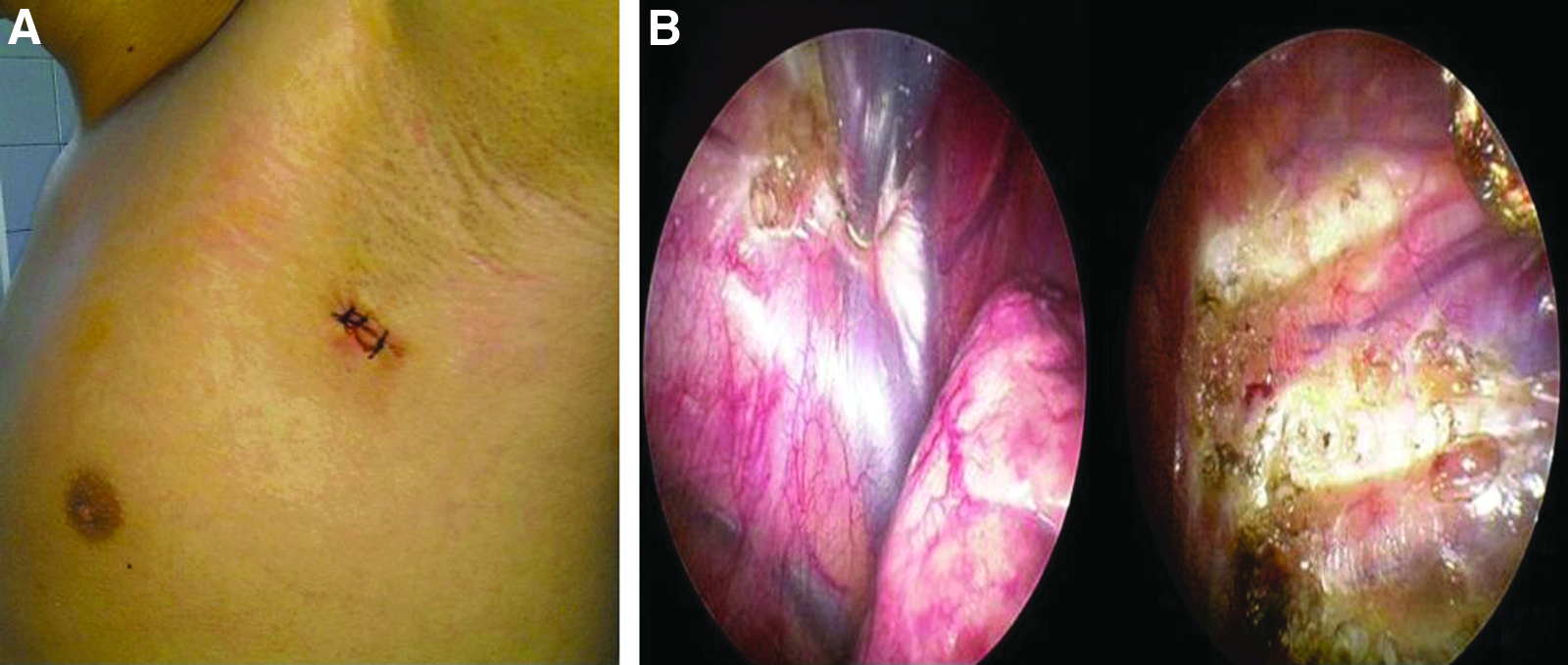
A preoperative chest radiograph was evaluated to exclude lung or pleural disorders for all patients. All procedures are performed with the patient under general anesthesia using a double-lumen endotracheal tube for isolated lung ventilation; patients were placed in the lateral decubitus and slightly forward position with the arm at 90° abduction and elevation. The patient was turned onto the other side after one side was finished. A 5-mm single port was made for insertion of the thoracoscope at the midaxillary line at the level of the third intercostal space. The sympathetic chain was identified at the level of the crossing of the second, third, and fourth costal heads under the pleura. The parietal pleura and the sympathetic chain were transected using unipolar electrocautery (Fig. 1). The transection was extended laterally for approximately 3 cm along the costa to include any accessory nerve fibers. We transected T2–T3 ganglia for palmar hyperhidrosis in 34 patients, T2–T4 ganglia for palmar and axillary hyperhidrosis in 39 patients, T3–T4 ganglia for axillary hyperhidrosis only in 5 patients, and T2 ganglia for facial blushing in 2 patients. A chest drain was inserted bilaterally through a 5-mm trocar and was subsequently removed the day after the operation; patients were discharged on the first postoperative day. Postoperative chest radiography was performed routinely. No conversion to thoracotomy was needed, and there was no operative mortality.
Patients were routinely assessed at a hospital visit 2 weeks postsurgery and then on an annual basis. Clinical information was obtained from medical records and by standardized telephone questionnaire. Mean patient follow-up time was 35.2±23.3 months (range, 1–76 months). The questionnaire assessed patients' degree of sweating, postoperative CS, overall satisfaction with surgical outcome, and complications. Statistical analysis of data was performed using chi-squared and Student's t tests.
Results
There was no operative mortality, and average hospitalization time was 1 day. Permanent anterior chest pain postoperatively was observed in 8 (10%) patients. The main postoperative complications were pneumothorax in 1 patient (1.25%) and hemothorax in 2 patients (2.5%), requiring chest tube insertion. Other complications included wound infection in 1 patient (1.25%) and dysesthesia of the arm in 2 patients (2.5%), which resolved after 1 and 7 months, respectively. These complications developed after discharge and required a second admission to the hospital for treatment. Complete relief of hyperhidrosis was achieved in 72 (90%) patients, whereas 8 (10%) experienced recurrence.
The response rate for the telephone questionnaire assessment was 100%. Overall, 71 patients (88.7%) were very satisfied, whereas only 9 (11.3%) were dissatisfied with surgical outcome. CS occurred in 62 (77.5%) patients and was mainly evident around the back, upper thighs, and legs. The degree of CS according to level of sympathicotomy is summarized in Table 1. CS was more frequent after two-level (T2–T4) sympathicotomy, although there was no significant difference between the one- and two-level procedures (P=.23). Overall, CS was greater with T2–T4 resection than with T2, T2–T3, or T3–T4 resection. However, no statistically significant difference was observed between resection at these levels (P=.81).
Patient satisfaction rate was 100% for operations at the T2 level (for blushing), 91% at the T2–T3 level (for palms, only), 87% at the T2–T4 level (for palms and axilla), and 80% at the T3–T4 level (for axilla, only). No statistically significant difference between levels was detected (P=.81) Subjectively, the esthetic outcome using a 5-mm uniport was considered positive by patients, and because of overall satisfaction and improvement in sweating, most would recommend sympathicotomy as the treatment of choice for hyperhidrosis, regardless of side effects.
Discussion
Thoracoscopic sympathectomy or sympathicotomy is a well-established treatment for severe primary hyperhidrosis when conservative treatment has failed. Different treatment modalities are generally used before surgery, including oral medications, botox injections, topical agents, and iontophoresis. However, these conservative treatments can have significant side effects, including drowsiness, dizziness, dry mouth, and blurred vision, and may not resolve symptoms. VATSE has been carried out as an alternative treatment in recent decades because of good symptomatic relief, improved patient quality of life, and low morbidity. There is little information regarding the long-term outcome of one- and two-level thoracic sympathicotomy and its effect on postoperative CS. In this study, we analyzed the early and mid-term follow-up of palmar, axillary, and facial hyperhidrosis treated by one- and two-level sympathicotomy.
The aim of surgical intervention is to interrupt communication between sympathetic nerve ganglia supplying the eccrine sweat glands. Several techniques have been used to accomplish this. First is sympathectomy, the resection of the sympathetic chain and ganglia.3–5 Second is sympathicotomy, which involves transecting the connections of the sympathetic trunk at one or more levels without resection.1,6,7 Diathermic ablation and ultrasonic dissection may also be used for both methods, whereas clipping is used only for sympathicotomy.4,8,9 Some authors have advocated ablating the ganglia because the surgical procedure is quicker and simpler and results in fewer cases of recurrence or complications, such as Horner's syndrome.10,11 Our experience in this study supports this hypothesis.
VATSE, which is generally performed at one or two levels (T2–T4), is an effective treatment approach for primary hyperhidrosis; however, postoperative CS is the most common unwanted side effect.1,3,12 The incidence of CS varies from 30% to 90%.13,14 CS was reported in 77.5% of our patients, and this compares favorably with reports in the literature. In spite of the high incidence of CS, overall patient satisfaction with the procedure was 88.7%, and the majority of our patients would recommend it to others.
Previous studies have found that CS was more common in T2–T4 resection than with T2, T3, or T2–T3 resection. 15 Similar results were obtained here after bilateral T2–T4 sympathicotomy, although the difference was not statistically significant (P=.81). We also observed that the extent of thoracic sympathicotomy could determine the severity of postoperative CS and the degree of postoperative palmar and axillary sweating, although this difference was not significant. Season appeared to exert an influence on CS symptoms: the frequency of CS was highest in the summer and lowest in the winter. Cerfolio et al. 16 reported that the highest success rate was seen when interruption is applied at the T3 or T4 level for palmar-only hyperhidrosis, and therefore T4 interruption is recommended for a lower incidence of CS. T4–T5 interruptions are also suggested for palmar and axillary, palmar, axillary, pedal, and axillary-only hyperhidrosis. 16 CS has also been found to be more common in T2/T3 sympathectomy than T4/T5, although the severity of clinical CS decreases during the first 3 years postoperatively. 17
One explanation for postoperative sweating is “reflex sweating”: the positive signal (reflex sweating) of the autonomic nervous system is blocked by the negative signal (sympathectomy). 18 Cutting at the level of T2 suppresses negative signals from T2 and below and sends the strongest positive signal. Therefore, positive signals are much weaker in T4 cutting than in T2 cutting. 18
In our study, there was an inverse correlation between the degree of patient satisfaction and severity of CS, but this correlation was not significant statistically (P=.41). Similar results have been previously reported. 19 We did not observe severe dry hands in our patients. Scognamillo et al. 20 reported no significant difference between T2–T4 sympathectomy and T3–T4 sympathicotomy in terms of compensatory hyperhidrosis, and both methods showed high efficacy for treatment of palmar hyperhidrosis.
The complication incidence in this study was 7.5% (n=6) and resolved with appropriate treatment. There were no observed cases of Horner's syndrome.
Conclusions
Uniportal transaxillary thoracoscopic sympathicotomy is an effective and simple method for treating hyperhidrosis with excellent cosmetic and functional results and good patient satisfaction levels. However, the high rate of CS is an undesirable and inconvenient side effect. We therefore recommend that it is important to inform patients before surgery about the potential risk of severe CS.
Footnotes
Disclosure Statement
No competing financial interests exist.