
Abstract
Abstract
Background:
Although Roux-en-Y hepaticojejunostomy is considered the gold standard of biliary reconstruction after excision of a choledochal cyst, there is increasing popularity of hepaticoduodenostomy, as it is easier to perform laparoscopically and provides physiologic bile drainage into the duodenum. Our animal research study had the goal to develop and test a new biliary reconstructive procedure (the duodenotubular flap [DTF]), with the advantages of providing physiological bile flow into the duodenum, technical simplicity of duodenal conduit construction, and ability of endoscopic assessment in case of complications.
Materials and Methods:
The DTF procedure consists of transection of the common bile duct (CBD), construction of the DTF from the second part of the duodenum, and biliary-enteric anastomosis. The first group of 6 dogs underwent reconstruction as a single surgical procedure. The second group of 4 dogs underwent the DTF procedure after the preparatory step of laparoscopic clipping of the CBD (for 7 days), to simulate the pathology of the choledochal cyst (extrahepatic biliary obstruction) and to ease the anastomosis. Laboratory analyses were performed pre- and postoperatively.
Results:
From the first group, 3 dogs developed a postoperative leak at the biliary-enteric anatomosis. The leak was recognized on postoperative day 4 in 2 dogs. They underwent an emergency abdominal exploration with redo anastomosis and had a complete recovery. The third dog died suddenly on postoperative day 10. Autopsy revealed incomplete disruption of the biliary-enteric anastomosis. In the second group, 3 dogs had an uneventful recovery, but 1 died on postoperative day 3. Autopsy revealed intraperitoneal bleeding with intact anastomotic and staple sites. None of the dogs in either group experienced leak at the staple lines, and none of the 8 surviving dogs developed postoperative cholangitis during the follow-up period from 15 to 20 months.
Conclusions:
The DTF procedure is feasible, simple, and quick, simulating physiological anatomy. Regarding the safety, a wide anastomosis seems to be the core of success.
Introduction
T
To prevent the disease progression and development of complications, surgical management is the treatment of choice. Surgical techniques have evolved over the last few decades from the internal drainage procedures (cystoduodenostomy, cystojejunostomy) to the current standard of complete cyst excision and reconstruction using Roux-en-Y hepaticojejunostomy (RYHJ) or hepaticoduodenostomy (HD). Although HD is considered as a simple, quick, and more physiologic reconstructive procedure, RYHJ is still favored by most surgeons, mainly because of the high risk of HD-associated complications (duodenogastric reflux and cholangitis).3–5
In a trial to combine the benefits of HD physiological bile flow into the duodenum, the technical simplicity of duodenal conduit construction, and the ability of endoscopic assessment in case of complications, we started this animal research project on a new biliary reconstructive procedure, which we named the duodenotubular flap (DTF). The main goal of the study was to assess the feasibility and safety of the new procedure.
Here we are presenting technical details of the DTF procedure, early outcomes, and lessons learned.
Materials and Methods
The study was conducted in the Department of Comparative Medicine, King Faisal Specialist Hospital and Research Centre, Riyadh, Kingdom of Saudi Arabia, with institutional animal care ethics and Institutional Review Board approval (protocol number RAC 2120005). Ten healthy Beagle dogs, with a mean body weight of 12 kg, were involved in a prospective research study.
From the animal facility, the sedated animal is brought to the operating room, after a fasting period of 12 hours. Following intravenous induction, the animal is placed under general endotracheal anesthesia and positioned supine. The abdomen is shaved, prepped, and draped in the usual sterile manner. The laparotomy is performed through the supraumbilical midline incision, and the anatomy of the biliary tree is identified. The common bile duct (CBD) is transected, and its distal end is ligated. The DTF is created from the middle segment of the second part of the duodenum (Fig. 1), using an Auto Suture 3.5-mm Multi-fire Endo GIA™ 30 stapler (Covidien, Mansfield, MA), in either a peristaltic or an antiperistaltic fashion.
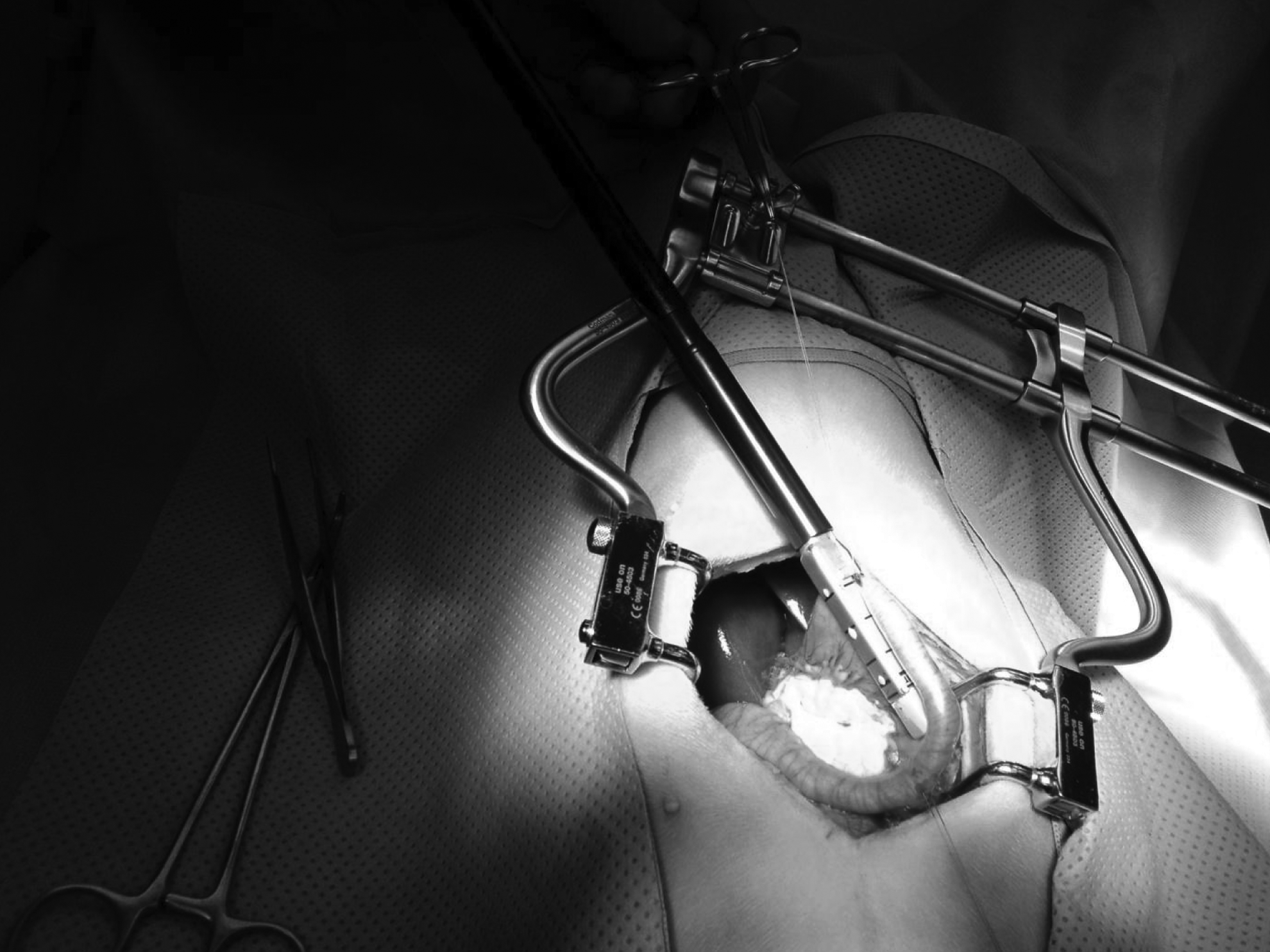
Construction of the duodenotubular flap using an Endo GIA stapler.
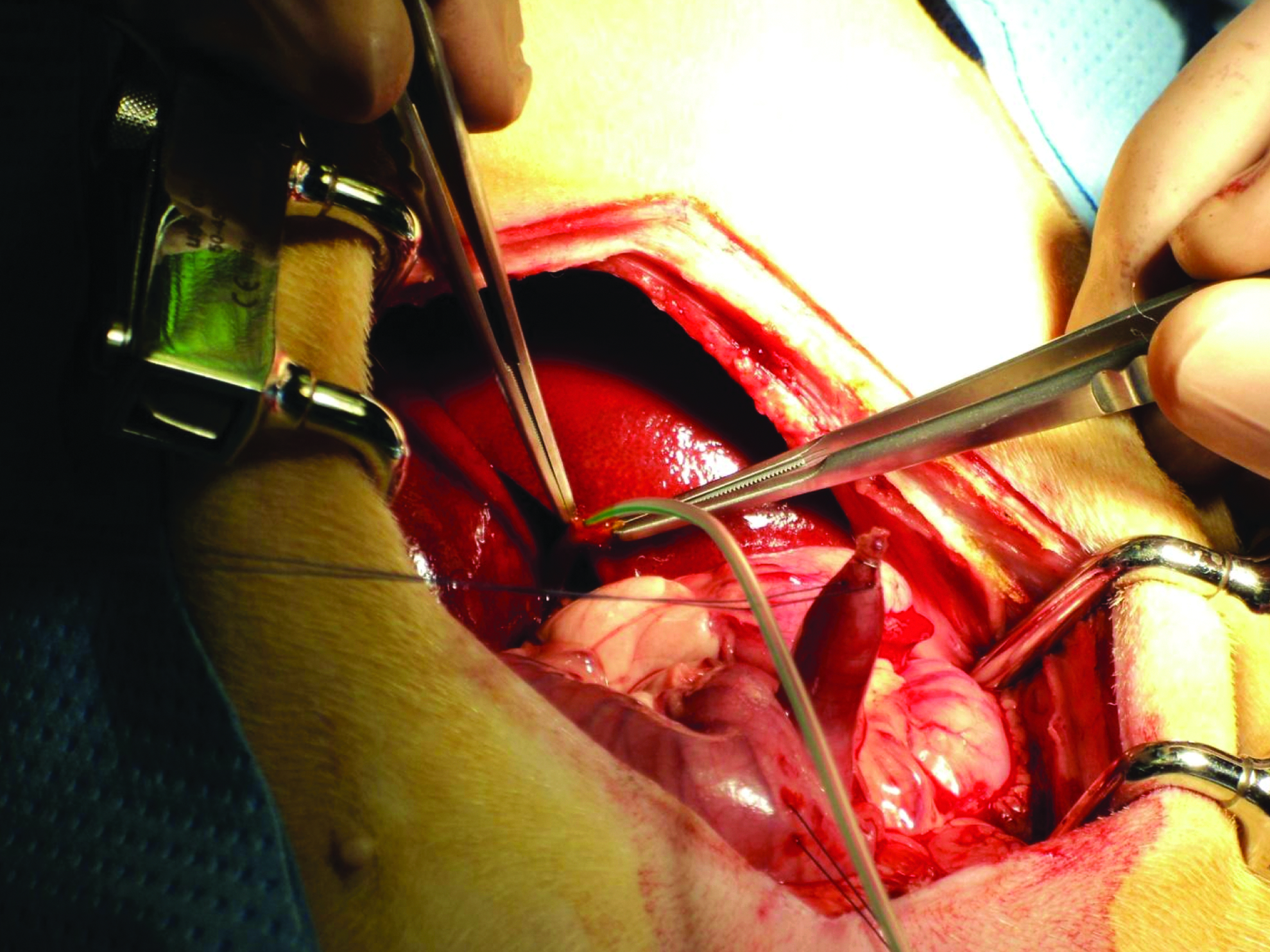
After creation of the DTF, the second part of the duodenum will attain a “V” shape appearance (Fig. 2). The DTF was created in an antiperistaltic way for 5 dogs and in the isoperistaltic way for the remaining 5 dogs. The biliary-enteric anastomosis was completed using Maxon™ 5-0 sutures (Covidien) over a 5 French stent (feeding tube) (Figs. 3–5). The abdominal cavity was closed in layers using absorbable sutures. The dressings applied included topical antibiotic, Steri-Strip™ closures (3M, St. Paul, MN), or Duo-Derm® dressing (ConvaTec, Bristol-Meyers Squibb Co., Skillman, NJ).
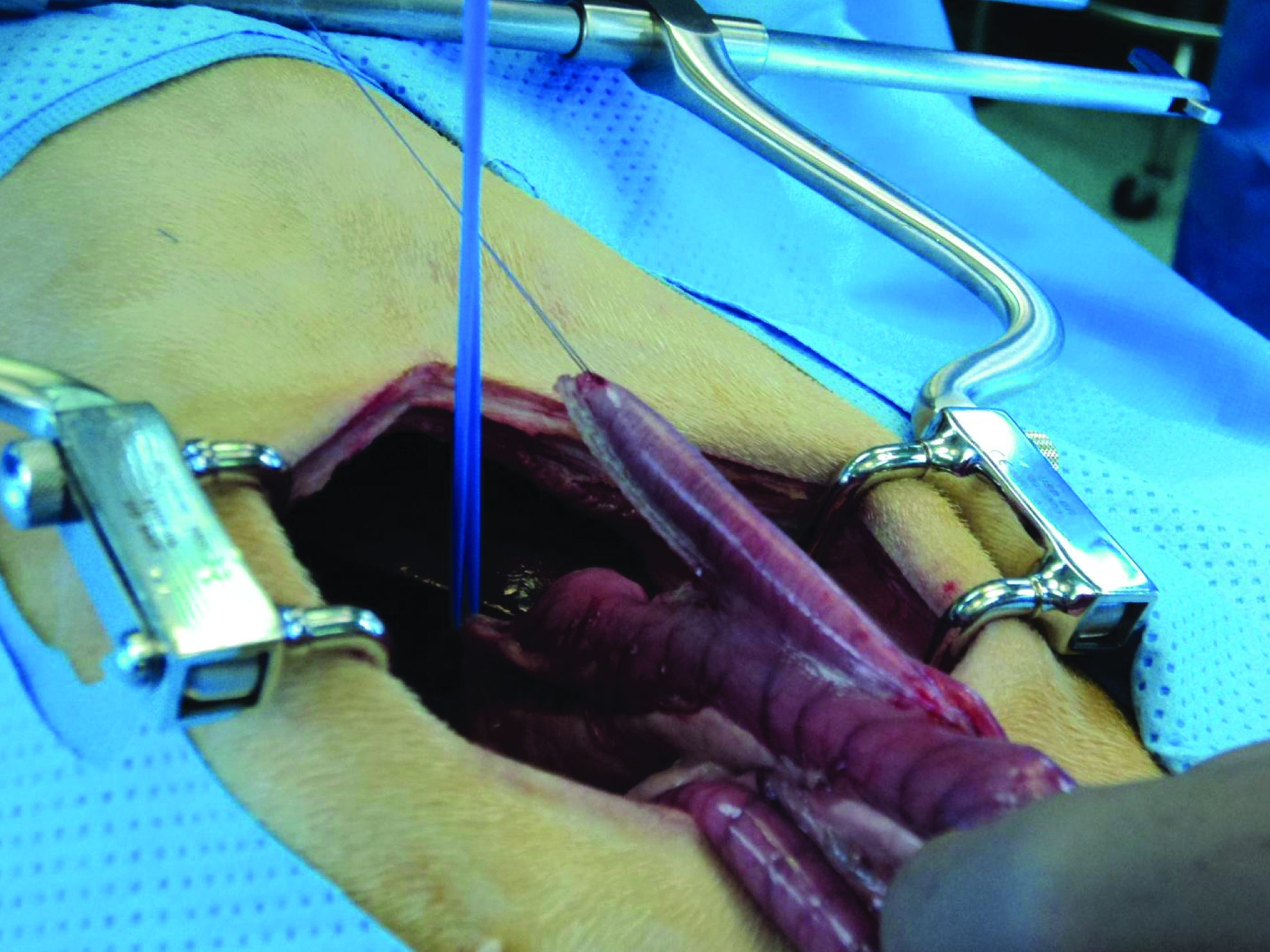
The “V”-shaped appearance of the isoperistaltic duodenotubular flap.
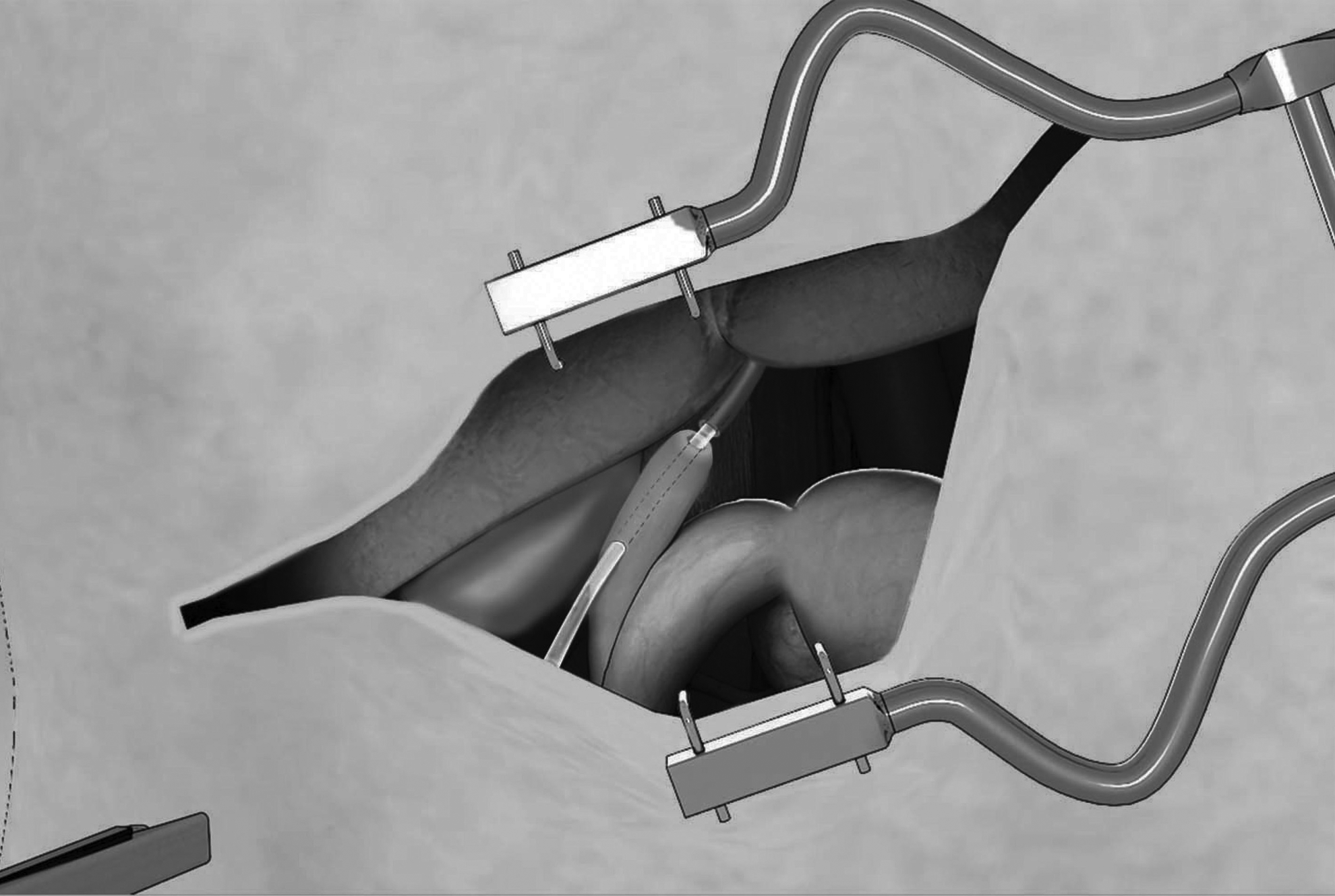
The duodenotubular flap with the transected common bile duct.

Creation of the anastomosis between the common bile duct and the duodenotubular flap.
Creation of the anastomosis between the common bile duct and the duodenotubular flap with the aid of a stent (a 5 French feeding tube).
Upon completion of the surgical procedure, the animals are observed in the recovery room and then housed for 2–3 days in individual cages, to ease clinical observation. Parenteral antibiotics and intravenous fluids are stopped once oral feeding is resumed. In case of complications, the management protocol is prolonged according to the clinical status.
Relevant pre- and postoperative clinical assessment and laboratory work-up are performed for all animals. The laboratory work-up protocol included the baseline study, followed by weekly blood work for 3 weeks and then every third week to complete 12 weeks of follow-up and/or normalization of laboratory results. The laboratory analysis included a complete blood count, the renal profile, and the hepatic profile (bilirubin, albumin, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, and gamma-glutamyl transferase).
Besides laboratory analysis, data on intraoperative technical issues, operative time, blood loss, incidence of postoperative leak, site of the leak (anastomosis versus staple line), and time of return to regular diet were collected.
Results
Between October 2012 and February 2013, 10 healthy Beagle dogs were treated in a prospective animal research study. Preoperative laboratory analysis values for all involved animals were within the physiologic range. Mean operative time was 45 minutes (ranging from 30 minutes to 1 hour).
The first group of 6 animals (60%) underwent a one-stage DTF procedure. The construction of the conduit was technically simple and quick, easily providing the required length and width of the duodenal conduit and leaving sufficient diameter of the remaining duodenum (usually one-half to two-thirds of the initial diameter). Following creation of the conduit, the biliary-enteric anastomosis was performed. To ease the construction of the biliary-enteric anastomosis, a 5 French feeding tube was used as a stent, which stayed in for 4 days and needed to be removed upon exploration for an acute abdomen with biliary-enteric anastomotic partial disruption in only 2 of the dogs. The diagnosis of anastomotic leak was established based on signs of clinical deterioration: decreased level of activity, loss of appetite, dehydration, fever, abdominal distention (ascites), and leukocytosis. An emergency exploration was performed, and the findings were free biliary fluid (approximately 1 L), partial to complete disruption of the biliary-enteric anastomosis, and intact duodenal staple lines. The abdomen was washed out, and anastomotic revision was done, with insertion of a Jackson–Pratt 10 French drain. Parenteral antibiotics and analgesics were continued, and both dogs recovered completely. One dog from the first group (the first animal in the study) died suddenly on postoperative day 10 secondary to an unrecognized anastomotic leak.
The second group of 4 dogs (40%) underwent a two-stage reconstructive procedure. The first procedure was laparoscopic clipping of the CBD for a period of 1 week, followed by the definitive biliary-enteric reconstructive procedure (DTF). The aim of the clipping was to enlarge the diameter of the CBD (simulating pathological biliary duct obstruction) and to ease the biliary-enteric anastomosis, without need for stenting. Three dogs from this group had an uneventful recovery, but 1 dog died on postoperative day 3. The autopsy revealed intraperitoneal bleeding and omental hematoma, with an intact biliary-enteric anastomosis and staple lines.
Intraoperative blood loss for all operated-on animals during the DTF procedure was minimal.
In the first group (dogs 1–6), bilirubin and gamma-glutamyl transferase levels were significantly increased postoperatively, peaking in the second week, and followed by a gradual but consistent decrease to normal values (Tables 1 and 2, respectively).
Died.
Died.
GGT, gamma-glutamyl transferase.
In the second group (dogs 7–10), levels of bilirubin and gamma-glutamyl transferase showed a sharp rise after clipping, followed by a steep drop after the DTF procedure toward normal levels (Tables 1 and 2, respectively).
All 8 surviving animals are clinically in good general condition and with normal laboratory parameters on follow-up ranging from 15 to 20 months.
Discussion
Although RYHJ is considered the gold standard surgical procedure for the management of choledochal cyst, there is increasing popularity of HD in the context of more extensive use of laparoscopy.3–6
Generally, even though HD is argued to be more physiologic, requires less operative time, and allows faster recovery of bowel function, RYHJ still seems favored by the majority of surgeons, with minimal support in the literature for this preference.4–6 The main concern related to HD includes its potential for cholangitis and reflux bile gastritis. 4 Regarding other surgical complications (bile leak, anastomotic stricture, bleeding, cholangitis, re-operation rate, and adhesive intestinal obstruction), a recent systematic review and meta-analysis showed no significant difference between the procedures. 5
Our research study aimed to assess feasibility and safety of the new DTF biliary reconstructive procedure, which integrates a few important demands: technical simplicity, physiological drainage of bile into the duodenum, and interposition of the conduit (DTF) simulating the normal anatomy may also decrease the potential of having recurrent cholangitis, with an additional advantage for an endoscopic surveillance in case of complications (leak/stricture).
The construction of DTF was technically simple and quick. In the first group of dogs, the demanding part was creation of the biliary-enteric anastomosis, due to the small diameter of the CBD. To overcome this problem, the anastomosis was done over a 5 French feeding tube as a stent. In the second group, the definitive procedure was preceded by the preparatory step of laparoscopic clipping of the CBD to enlarge its diameter and to ease anastomosis.
A wide biliary-enteric anastomosis is expected to provide free bile flow via the conduit into the physiologic environment of the duodenum. A sufficient length of conduit is expected to reduce the frequency and seriousness of the complications associated with duodenal reflux into the biliary tree and may have a positive impact on prevention of cholangitis.
It is interesting that the stricture on the flap has not developed in any of the dogs. This is probably related to an optimal length of the DTF, not compromising the duodenal diameter, and preserving an adequate vascularization.
The high mortality is related to our learning curve and the experience gained in animal care.
In our experimental study we opted to transect the CBD instead of the common hepatic duct because our main goal at this phase of research was to test the feasibility and safety of the new biliary reconstructive procedure. We also consider that the DTF procedure could potentially find its use for other biliary pathologies, other than the choledochal cyst.
Anatomically, the DTF provides adequate length and width of the duodenal conduit, without compromising the functionality of the remaining duodenum, and theoretically with an antireflux mechanism. Physiologically, DTF provides direct bile drainage into the duodenum, an important element in regard to intestinal hormonal production and fat absorption, aiming to simulate normal anatomy, physiology, and perhaps an antireflux mechanism.
In the line with these expectations, none of the 8 surviving dogs had ascending cholangitis during the follow-up period of 15–20 months.
After finalizing our first phase of research, which aimed mainly to assess the feasibility and safety of the new procedure, we expanded our study to the currently ongoing endoscopy (endoscopic retrograde cholangiopancreatography) evaluation of DTF to assess accessibility to the conduit and biliary tree.
Conclusions
The construction of the DTF is technically feasible, simple, and easy to perform. The newly described biliary-enteric anastomosis simulates physiological anatomy.
The next step of our research will be clinical application of this technique in human subjects with any extrahepatic biliary pathology in a controlled research study to ascertain its feasibility and safety.
Footnotes
Acknowledgments
This study is the result of the kind, attentive, and considerable contributions of many people over the past 2 years. The authors would like to extend their sincere gratitude for the persistent help and support to all members of the Department of Comparative Medicine at the King Faisal Specialist Hospital and Research Centre, in particular to Dr. Rafat ElSayed, Dr. Abdullah Assiri, Dr. Falah AlMohanna, and Dr. Asma Ali, to the King Faisal Specialist Hospital and Research Centre operating room nurses, Ms. Chahla Fares, Ms. Keng See Wong, Ms. Chewbang Chuah, Ms. Jossie Taipin, and Ms. Ebtisam AlMwanes, and to Dr. Mohamed Shoukri for the statistics assistance. We are very grateful to Dr. Andrea Hayes Jordan from the University of Texas Medical School of Houston for her help, guidance, and support throughout the process of our research.
Disclosure Statement
No competing financial interests exist.