
Abstract
Abstract
Background:
We designed a novel, spherical magnetic compression colorectal anastomosis device and established a swine model to assess the feasibility and safety, as well as advantages, of the device.
Methods and Materials:
Fifteen animals were divided into five groups (sacrificed on Days 3, 5 7, 9, and 14) with 3 in each group. In each group, a magnetic compression device was used in 2 animals (experimental animals), and a stapled device was used in 1 animal (control animal). Feeding status, bowel movements, the discharge time of the magnetic anastomosis device, burst pressure, and magnetic field strength were recorded. Gross anatomical and histological examinations were performed.
Results:
The average device discharge time was 7.5 days. The burst pressure increased over time for both the experimental and control animals. Both the gross anatomical and histological examinations suggested that the inflammatory reaction was milder. Healing occurred more quickly, and the incidence of complications was lower for the experimental animals than for the control animals.
Conclusions:
The potential benefits of the spherical magnetic compression colorectal anastomosis device, relative to the stapled device, were in terms of effectiveness and complication incidence, which encourages us to further study its application in gastrointestinal anastomosis.
Introduction
O
The principle behind those compression anastomosis devices is that they can produce a long-lasting pressure against the side wall at the mucosal surface that gradually blocks blood flow, causes tissue necrosis, and ultimately releases the anastomosis ring, so it is eliminated in the feces. On the serosal side, they maintain blood supply, gradually finish the contact-adhesion healing process, and ultimately achieve a complete anastomosis without a stapler4,5; these concepts explain the essential difference between a compression anastomosis and a stapled anastomosis. Magnetic compression anastomosis has been widely used in bile duct and vascular anastomoses.6,7 However, its application in the gastrointestinal tract is limited because of issues pertaining to device release.
On the basis of the principle of magnetic compression, we designed a novel, spherical magnetic compression device for colorectal anastomosis. The spherical design facilitates its elimination, which we verified in our swine model. In this study, we planned to evaluate the technical feasibility, safety, and advantages of this spherical magnetic compression colorectal anastomosis device and provided an experimental basis for additional application of the device in clinical settings.
Materials and Methods
Device design
The spherical magnetic compression anastomosis device consisted of two complementary hemispherical structures with a sliding device and an internal magnetic anastomotic ring in each hemisphere. During an intestinal anastomosis, the intestinal ends are affixed to a hemisphere and form a complete sphere. The magnetic attraction produces sustained pressure against the intestinal wall and completes the anastomosis. The cylindrical channel enables the intestinal space to be clear (Fig. 1). The spherical device was composed of a nontoxic, polyethylene material, and there were three specifications according to the diameter: 32 mm, 28 mm, and 26 mm. The respective internal diameters were 15 mm, 13 mm, and 11 mm, which were suitable for a colorectal or small bowel anastomosis. The magnetic anastomosis ring was composed of a neodymium-iron-boron magnetic material with outside diameters of 29 mm, 26 mm, and 24 mm and inside diameters of 25 mm, 22 mm, and 20 mm, respectively. The surface magnetic force was 2000 G. The sphere weighed 10 g, and the surfaces of the sphere and the internal drainage channel were smooth and not harsh to the intestinal mucosa, which allowed the intestinal content to move smoothly, so no damage to the intestinal tract would occur when the sphere was released and eliminated from the intestinal tract.
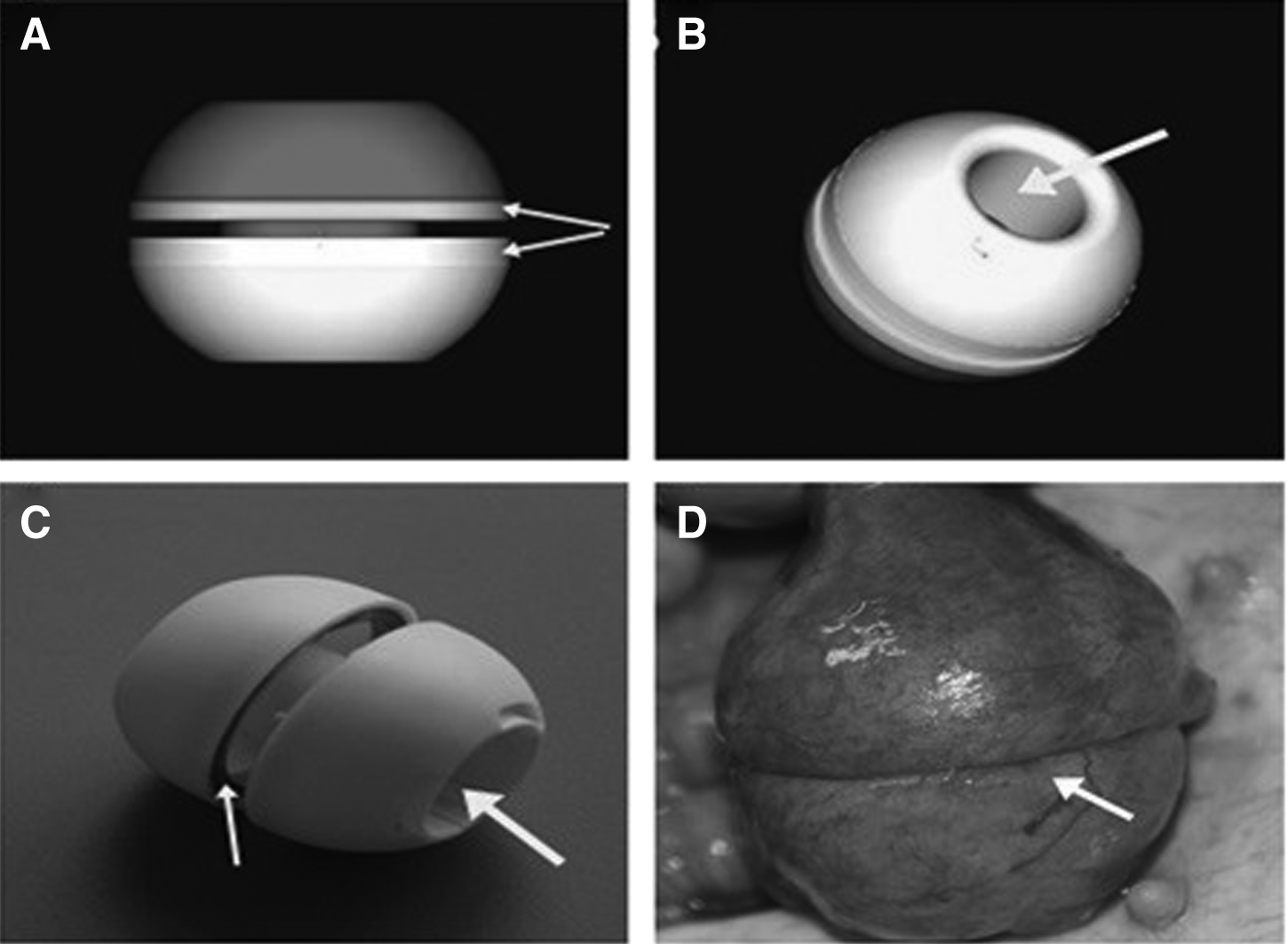
A complementary hemispherical structure:
Experimental animals
Fifteen healthy female pigs weighing 38–42 kg were provided by the Experimental Animal Center, Shandong University School of Medicine, Jinan, China, and the experimental procedure was approved by the Animal Ethics Committee, Shandong University School of Medicine. The 15 animals were divided into five groups, with 3 in each group, and each group had an average weight of 40 kg. They were fed a liquid diet 48 hours before surgery and began fasting 8 hours before surgery. During surgery, they were given 500 mL of a 5% glucose solution with metronidazole intravenously. After surgery, they were given a glucose solution on Day 1, a liquid diet on Day 2, and a semiliquid diet on Day 4, and they were gradually switched to a normal diet.
Experimental design
The 15 animals were divided into five groups, with 3 in each group. Two animals were designated as experimental subjects with a middle rectum magnetic compression anastomosis, and 1 animal was used as a control with a middle rectum stapled anastomosis. The postoperative feeding situation, defecation, and magnetic anastomosis device release time were recorded. Additionally, the animals were sacrificed on Days 3, 5, 7, 9, and 14 after surgery, and tissue samples were collected for further analysis.
Surgical procedures
All experimental animals had general anesthesia. A midline incision was created on their abdomen, and their rectum was exposed. For the experimental groups, the following procedures were performed: the mesorectum was isolated approximately 15 cm from the anal margin, the rectal bowel was cut in half, and the proximal and distal ends were anastomosed through a complementary magnetic anastomosis device. For the control group, the following surgical procedures were performed: the mesorectum was isolated approximately 15 cm from the anal margin, the rectal bowel was cut in half, and the proximal and distal ends were anastomosed by using a Johnson 29-mm round nail stapler (circular stapler, product number CDH29; Johnson & Johnson, Somerville, NJ) to complete an end-to-end nail rectal anastomosis. Neither the experimental group nor the control group was reinforced with silk thread. Each layer of the abdominal wall was carefully stitched to prevent the formation of an abdominal wall hernia, which may affect anastomotic healing. After awakening from the anesthesia, the animals were kept and fed separately until they were sacrificed.
Postoperative follow-up
The animal feeding situation, defecation, and magnetic anastomosis device discharge time were recorded. After each animal was sacrificed, an anatomical examination was performed to check whether any local infection, anastomotic fistulas, adhesions, or bowel obstruction existed. The anastomotic pressure and magnetic field strength were measured, and all the anastomotic tissues were subject to hematoxylin–eosin staining for observing histological changes during healing.
Statistical analysis
Using the SPSS version 16.0 statistical software (SPSS, Inc., Chicago, IL), Student's t test was used to compare the differences between groups, and a value of P<.05 was considered statistically significant.
Results
Rectal anastomoses in the experimental and control groups
There was no significant difference in rectal anastomosis operation time between the two groups (P>.05), and no significant difficulties occurred during the operations. The time for a rectal anastomosis operation was 10.5±0.5 minutes in the experimental animals and 10.2±0.5 minutes in the control animals.
Magnetic anastomosis device discharge time
There was no significant difference in magnetic anastomosis device discharge time. The average time for bowel movement resumption was 4 days. The average time for a magnetic anastomosis device discharge was 7.5 days (range, 6–9 days); the anastomotic ring was intact, and no necrotic tissue or bleeding was found. In the Day 7 group, 1 animal eliminated the device on Day 6, whereas another animal had her device release and was close to being eliminated. In both animal groups, the anastomoses healed well.
Postoperative complications
Postoperative complications were found during an anatomical exploration. In the control animals, we observed that 1 case (1/5) had an anastomotic fistula, and 2 cases (2/5) had visible adhesions around the small intestine but no anastomotic stricture. In the experimental animals, there was no anastomotic fistula or stricture, but adhesions were found in 2 cases (2/10).
Maximal magnetic field strength
The magnetic field strength was maximal at the anastomotic site. As the distance increased, the magnetic field strength decreased. The magnetic field strength was measured with a gauss meter (model 5180; F.W. Bell, Pacific Scientific-OECO, Orlando, FL). The average magnetic field strength was 132.67 G at the anastomotic site, and 1.5 cm distal to the anastomosis, the average strength was 9.75 G; 3.0 cm distal to the anastomosis, the average strength was 1.25 G. It was difficult to detect the magnetic field strength at the abdomen, back, and chest (Table 1).
Distance between the magnetic probe and the anastomosis.
Burst pressure
The burst pressure increased with time after an anastomosis operation. The burst pressure is the instant intraluminal pressure during an intestinal anastomotic leak or rupture and was measured with a calibrated pressure gauge that was connected to the intestines. For the experimental animals, the burst pressure was 117.5±2.5 mm Hg on Day 5, which was the lowest pressure, followed by 280±7.5 mm Hg on Day 7, and reached 300±5.0 mm Hg and 307.5±5.5 mm Hg on Days 9 and 14, respectively. For the control animals, the burst pressure was 72.5 mm Hg, 200 mm Hg, and 180 mm Hg on Days 5, 7, and 9, respectively, and reached 300 mm Hg on Day 14 (Table 2).
By chi-squared test.
Gross and histological examinations
There was more severe inflammation around the anastomotic site in the control animals than in the experimental animals. On Day 3, in the experimental animals, we found inflammatory swelling and a good anastomotic closure with no proximal intestinal congestion or anastomotic fistula. A histological examination showed an inflammatory exudation, a small amount of fibroblast infiltration, and new blood vessels, with no collagen increase. In the control animals, there was a large area of inflammatory exudates but no anastomotic fistula or stricture. A histological examination showed a more severe inflammatory exudation, but no significant fibroblast infiltration or blood vessels (Fig. 2).
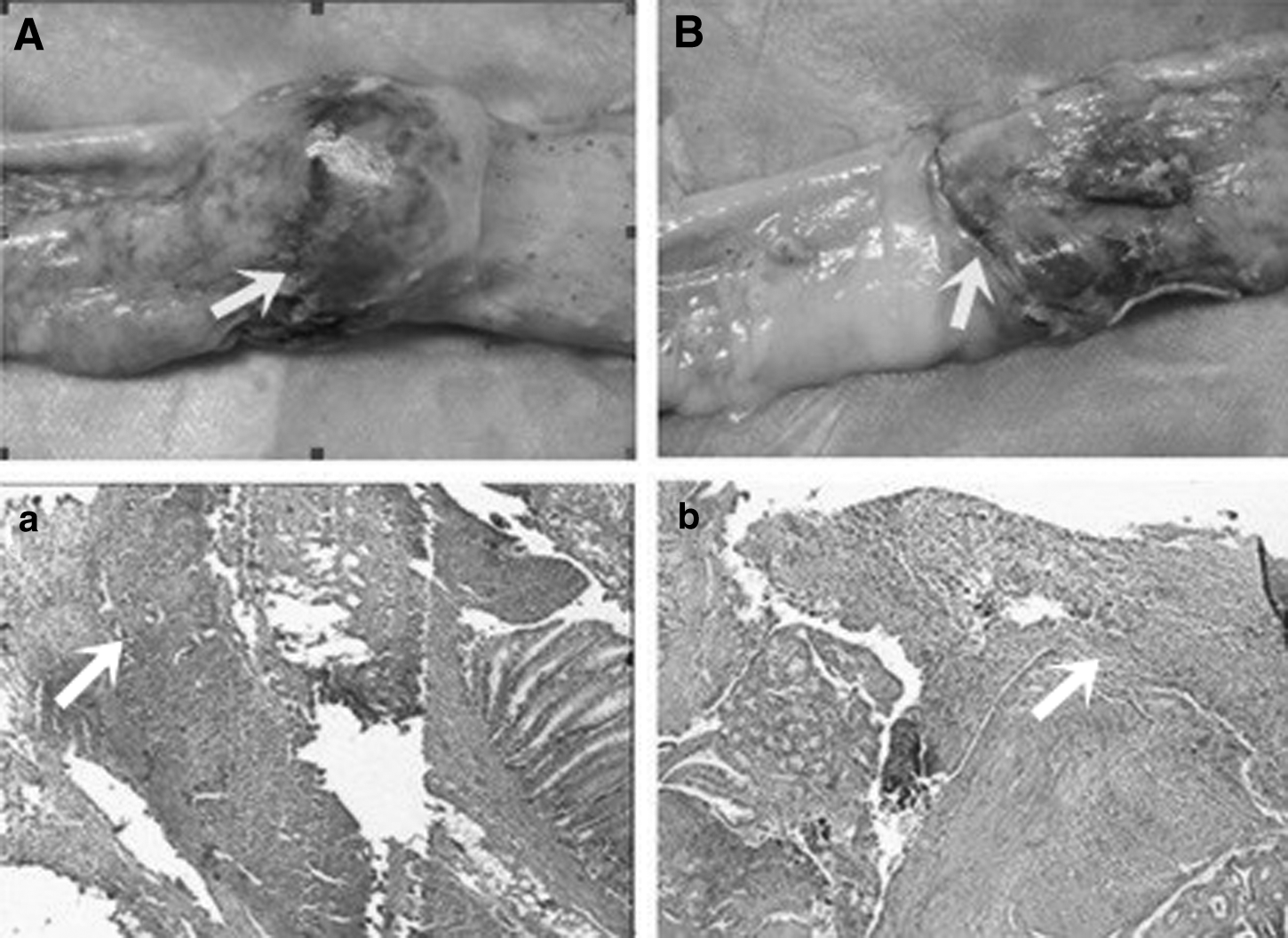
Gross anatomical and histological examinations on (Fig. 2) Day 3, (Fig. 3) Day 5, (Fig. 4) Day 7, (Fig. 5) Day 9, and (Fig. 6) Day 14: a gross anatomical examination of
On Day 5, in the experimental animals, the inflammatory exudates were significantly reduced, and the serosal side was smooth. There was no anastomotic fistula. A histological examination showed fibroblast proliferation, capillary proliferation, a reduced inflammatory exudate, and a small amount of collagen fibers. The control animals still had a severe inflammatory exudation, and the serosal side was rough. A histological examination showed obvious fibroblasts and capillary proliferation, and the inflammatory exudate was reduced but was still more severe than that in the experimental animals. A small amount of collagen fibers could be seen (Fig. 3).
On Day 7, in the experimental animals, the serosal membrane that was around the anastomosis had healed, and the anastomotic cracks and inflammatory exudates had disappeared. A histological examination showed hyperplastic granuloma formation, accompanied by an inflammatory exudate and collagen fibers. In the control animals, the inflammatory exudation, visible cracks, and serosal roughness were still notable. A histological examination showed inflammatory cell infiltration such as fibroblast and endothelial cells, as well as collagen fibers (Fig. 4).
On Day 9, in the experimental animals, the anastomotic incision had healed with no significant inflammatory exudate. A histological examination showed increased numbers of fibroblasts and collagen fibers, decreased numbers of capillaries, the appearance of scar tissue, and the absorption of inflammatory exudates. In the control group, we observed scar healing, along with the remaining staples and local tissue necrosis. A histological examination showed increased numbers of fibroblasts and collagen fibers, decreased numbers of capillaries, and the absorption of inflammatory exudates (Fig. 5).
On Day 14, in the experimental animals, scar healing was observed. A histological examination showed obvious fibroblast proliferation and collagen fiber production with scar formation. Along with mucosal hyperplasia, the wound was mostly covered. In the control animals, scar tissue of a greater width and a narrow intestinal space were observed (Fig. 6).
Discussion
We designed a new type of spherical magnetic compression colorectal anastomosis device and established a swine model in order to assess the technical feasibility, safety, and advantages of the device in a colorectal anastomosis. The device was designed for use as two complementary hemispherical structures. Accompanied by a magnetic compression ring, they automatically complete the match, with a cutting and anastomosing process, and restore intestinal continuity. Meanwhile, after the completion of an anastomosis, the internal space of the sphere forms a drainage channel with inner diameters of 11 mm, 13 mm, and 15 mm, which allows the intestinal content to pass easily and to reduce pressure at the anastomosis. The overall weight of the sphere was about 10 g, which was equal to the weight of stool with a similar volume. Therefore, the downward pressure generated by the weight of the device itself would be significantly reduced. The surface of the anastomotic sphere was smooth, so it would not damage the intestinal wall upon release and could be easily eliminated with a bowel movement.
Studies have shown that a postoperative anastomotic fistula in the lower rectum occurred with an average time of 6 days, 8 which was consistent with our findings. Our results showed that at an early anastomotic stage, the magnetic compression device could withstand more pressure than a stapled device. At this stage, elastin and collagen were lacking, and the rectum was prone to an anastomotic fistula. The submucosa was the main component of the anti-tension system, and the magnetic compression device could obtain direct contact with this layer. Meanwhile, it could obtain complete contact with the serous membrane that maintained the blood flow and reduced the occurrence of an anastomotic fistula.9,10 In this study, there was no anastomotic fistula in the experimental animals, and the control cases had an anastomotic fistula (1/5).
In clinical settings, there is a high incidence of adhesion in gastrointestinal surgery, which is related to an inflammatory reaction in the surgical field.11,12 In this study, the experimental group had demonstrated that it had apparent advantages on gross and histologic examination. In both the experimental and control groups, there was no anastomotic stricture, but on Day 14, there was scar tissue, which was less visible in the experimental group than in the control group. During the healing process, a mild inflammatory reaction occurred with a magnetic compression device anastomosis, along with a small amount of scar tissue that was helpful in order to reduce the incidence of an anastomotic stricture.5,13
Research has shown that the greater the magnetic force is, the greater the compression strength, and the shorter the excision time is, the earlier the release of the device, so the greater the effect on the surrounding area. If a magnetic force of 3000–6000 G is applied, the anastomotic ring releases as early as 48 hours because of necrosis, accompanied by an anastomosis fistula. 14 In this study, we used a magnetic force of 2000 G, ensuring tight contact and a quick release after healing, so as to avoid interference with the surrounding area (Table 1). Magnetic compression produces a long-lasting, yet gradually increasing, pressure against the intestinal wall. With a decrease in the distance between the two magnetic rings, the magnetic force gradually increases and accelerates tissue necrosis, ensuring that the device will release within 7 days and that the anastomosis would completely heal.
Magnetic compression anastomosis devices have shown significant advantages over stapled devices in terms of the anastomotic effect and the complication incidence. Currently, MAGNAMOSIS IV, which was designed by Wall et al., 15 achieved a promising result in colorectal anastomoses. We made innovative changes in the following aspects: a complementary structure to facilitate anastomosis and to avoid dislocation; an appropriate magnetic strength in order to ensure smooth anastomotic healing and to avoid interference with the surrounding area; a large central drainage channel so intestinal contents could smoothly pass; and a lighter and less expensive device that would be more affordable. Although it takes several days for the device to be eliminated in the feces, which is a major concern for most surgeons, the device has been demonstrated to be superior to a stapled device.
In summary, in terms of anastomosis result, burst pressure test, healing status, the degree of inflammatory reaction, and the complication incidence, we have demonstrated potential benefits of the novel spherical magnetic compression colorectal anastomosis device. These advantages encourage us to further study its application in gastrointestinal anastomosis.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Development Plan of Shandong (grant 2008GG10002054) and the Natural Science Foundation of Shandong (grant ZR2010HL024).
Disclosure Statement
No competing financial interests exist.