
Abstract
Abstract
Introduction:
We describe our experience with the use of a modified technique for laparoscopic internal inguinal ring closure (peritoneal incision and double “N” stitch placement). We evaluate the technique in terms of feasibility, efficacy, and safety.
Materials and Methods:
From November 2003 to March 2014 we performed 1700 herniorraphies by laparoscopy. We selected 123 patients treated with the “double N” technique by the same surgical team, and we reviewed their notes analyzing demographic data, operative times, intra- and postoperative complications, and recurrence rate. The technique used is a modification of the Schier technique. Our technique consists of a partial lateral peritoneal 180° incision around the internal inguinal ring and in the placement of a double stitch. The first stitch is used to approximate the muscles with the inguinal ligament, and the second one is used to close the peritoneum above them.
Results:
The female to male ratio was 22:101. Mean age at surgery was 4.3 years (range, 1 month–12 years). Mean operative time was 30 minutes (range, 20–50 minutes). There were 60 bilateral cases. There were no intraoperative complications. Two patients had reactive hydrocele treated conservatively, and 1 patient developed umbilical infection. We did not identify any recurrence.
Conclusions:
Our early results suggest that the “double N” laparoscopic technique to close the internal inguinal ring in children is safe and efficient. We therefore suggest using this approach in children with a patent internal inguinal ring of >1 cm. The recurrence rate is low, but it should be better assessed by studies with longer follow-up.
Introduction
I
In this article we describe a modified laparoscopic technique that provides for internal inguinal ring closure with a double “N” stitch after partial lateral peritoneal incision.
Materials and Methods
We retrospectively reviewed all medical charts of patients affected by inguinal hernia who underwent laparoscopic correction by the “double N” technique between November 2010 and March 2014 in a single pediatric center. We considered 123 patients who are part of a larger series of 1197 patients (1700 herniorraphies) who were operated on for the same pathology between November 2003 and March 2014. The subsample was created on the basis of selected criteria adopted to evaluate the new technique. Selection criteria were as follows: all the procedures performed by the same surgical team that had experience with laparoscopy and at least 6 months longer follow-up to detect possible recurrences. In particular, during follow-up, all patients were invited for an interview and for a visit at our outpatient clinic 1 month after surgery. This is a routine practice at our Department after inguinal hernia repair surgery. In order to identify late recurrences, we then contacted again by phone all our patients, and we invited them back for another clinical evaluation or for a telephone interview at least 6 months after surgery. The interview and the clinical examination aimed at collecting information regarding the postoperative course and identifying signs of recurrence.
Technique
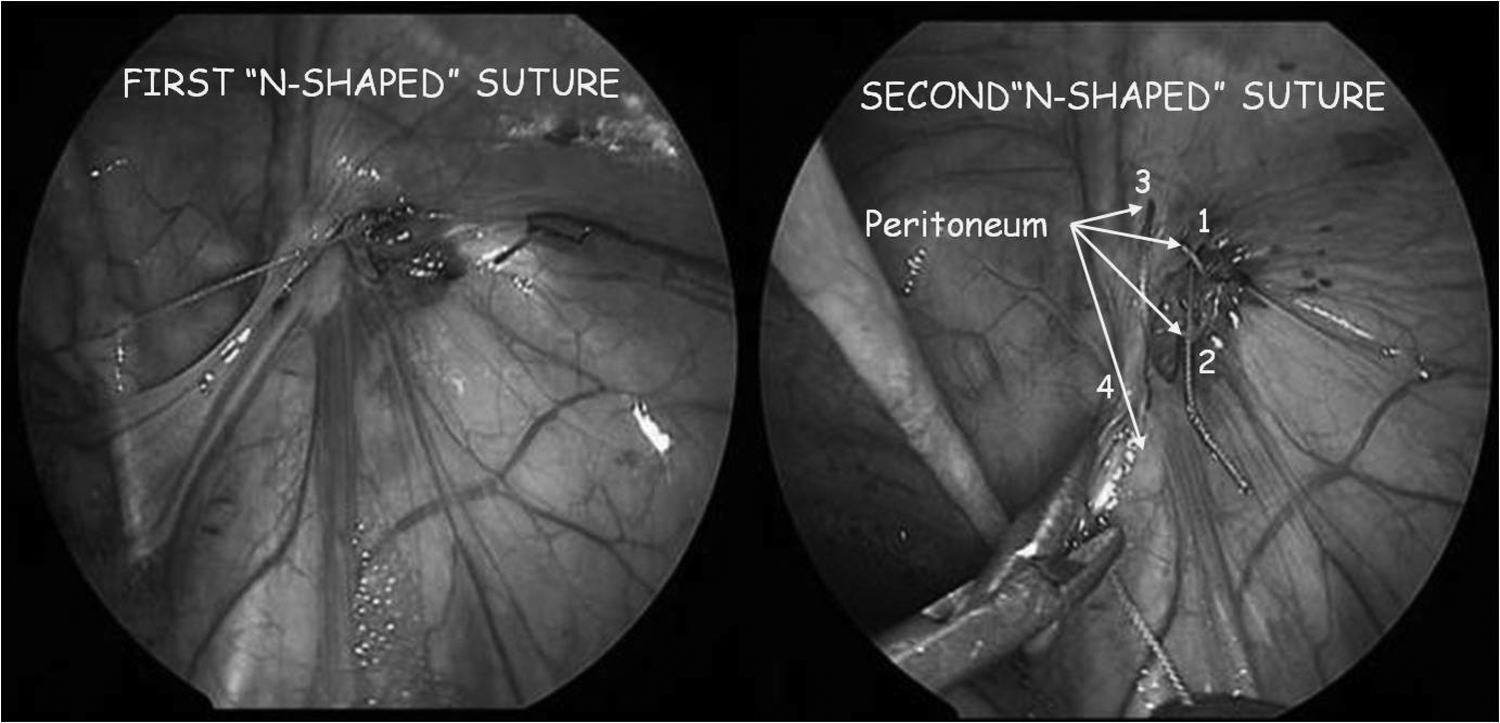
A subumbilical incision is created, and a 5-mm port (with or without pneumatic anchorage) for the scope (5 mm, 0° lens) is inserted using an open technique. The pneumoperitoneum is created with CO2 (0.5–1 L/minute of flow and 6–10 mm Hg of pressure, depending on the patient's size). Two additional 2- or 3-mm trocars for instruments are inserted under direct vision in the left and right flanks. The anterior abdominal wall (in particular, the internal inguinal ring) is carefully inspected on both sides. We reduce herniated organs, if present, and we check for their viability. We perform a 180° peritoneal incision to promote the scarring. In order to do so, we lift up the peritoneum on the lateral margin of the open internal inguinal ring with an atraumatic grasper, and we cut it with scissors. A 2-0, 3-0, or 4-0 nonabsorbable suture, introduced through the abdominal wall, is used to close the ring (Fig. 1).

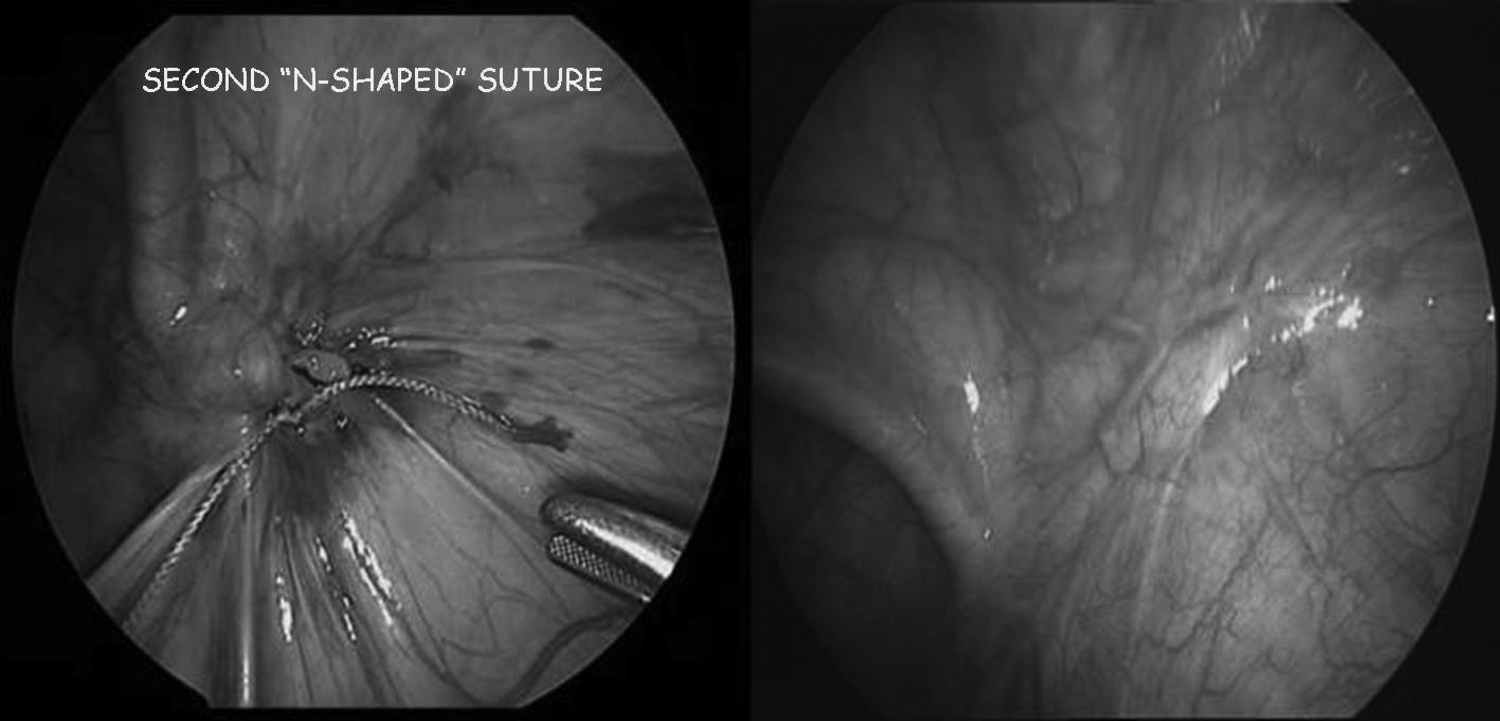
We perform two N-shaped running sutures. The deepest one is used to approximate the conjoint tendon that is exposed after the peritoneal dissection, with the opposite side (the inguinal ligament); then the peritoneal defect is closed upon the first knot with another “N” suture (Fig. 2).
In males, it is important to make a passage between the vas and the spermatic cord. In females, we usually anchor the uterine ligament. External pressure on the inguinal canal is exerted during knot closure to reduce tension over the margins. At the end of the maneuver (Fig. 3), the needle is removed along with the trocars under direct vision.
The umbilicus is closed with a purse-string suture made at the beginning to keep the port fixed during the procedure (in the case of a port without pneumatic anchorage). Steri-Strip™ closures (3M, St. Paul, MN) are used to close the trocar wounds. Feeding starts 2 hours after surgery (postoperative management is the same as for other laparoscopic herniorraphies [LHs]).
Results
We identified 101 boys and 22 girls. Mean age at operation was 4.3 years (range, 1 month–12 years). The defect was on the right side in 37 patients, on the left side in 26 patients, and bilateral in 60 patients. Intraoperative findings differed from preoperative diagnosis in 51 patients (incidental bilateral findings). Mean operative time was 30 minutes (range, 20–50 minutes). There were no conversions or intraoperative complications. After surgery we identified 2 patients with self-limited hydrocele and 1 patient with umbilical infection that required prolonged antibiotic therapy. All patients were discharged the day after surgery (according to the anesthesiology policy). Mean follow-up was 14.8 months (range, 6–40 months).
Discussion
Herniorrhaphy procedures have been increasing in the last decades in pediatric surgical centers. 1
In the same way, laparoscopy has gained popularity also in patients of young ages thanks to the development of instruments and video technologies. 2
Nevertheless the laparoscopic approach for pediatric inguinal hernia correction is controversial. 3 Doubts have been expressed regarding the high recurrence rates, longer learning curve, high costs, and longer duration of surgery.
However, a recent meta-analysis that took into consideration three randomized controlled trials and four observational clinical studies shows that LH has similar operative time, length of hospital stay, recurrence and complications rates compared with open herniorraphy. 4
The main problem is that a uniform laparoscopic technique has not been identified yet (more than 15 different techniques have been described in the literature). On the contrary, there is an open herniorraphy procedure that has been codified and accepted for over 50 years. 5
LHs differ in methods of ligation of the patent vaginal canal (PVC) at the internal inguinal ring. The aim is to improve the outcome. The various techniques can be grouped on the basis of four elements
6
:
1. Type of knotting (intracorporeal and extracorporeal) 2. Number of ports (three or single) 3. Sac management (inversion and ligation; resection with or without ligation; flip-flap) 4. Use of tissue adhesives.
The critical steps to obtain a definitive open inguinal hernia repair seem to be proper high ligation and excision (or transection) of the hernia sac. 7 Wheeler et al. 8 advocated the use of these technical aspects also for LH to avoid recurrences.
The paradigm “high ligation and sac excision equals no recurrence” is fairly uniformly accepted.
Some authors have proposed a laparoscopic approach that includes sac resection without suture.9,10 This technique is based on the assumption that inguinal hernias in children are persistence of the sac rather than an aponeurotic defect. 11 Sac resection is therefore sufficient for the treatment, and it does not require laparoscopic suture skills. 9 We should say “complete sac excision equals no recurrence.” Unfortunately, this technique is associated with a high risk of adhesions between the gut and the peritoneal defect.11,12
Borkar et al. 13 questioned the need for partial resection of the sac during LH. They randomized 50 patients (25 received inguinal hernia repair with sac partial resection, and 25 without it) and showed that omitting the resection step during LH does not affect the outcome. This is probably related to the fact that the hernia is tackled at its origin. We could make a simplification and say “high ligation equals no recurrence” or, even better, “ high effective closure equals no recurrence.” But how do we make a closure effective?
The ligature alone has been proposed, 14 but it has a high recurrence rate. 11 Causes of recurrence might be the use of absorbable suture or the peritoneal continuity. 11
At our institution the use of laparoscopy to close internal inguinal rings was introduced in 2003. At the beginning of our experience we adopted the Schier technique (“Z suture”) to correct inguinal hernias regardless of the diameter of the defect.15,16 In order to reduce recurrences we decided to include muscles and the inguinal ligament in the suture in the case of large defects (>1 cm). The technique was further modified in order to obtain a two-plane closure that is performed after peritoneal lateral incision (180° peritoneal incision). The idea is to simplify the procedure, avoiding the complete dissection and resection of the sac and taking advantage of a partial incision that leads to adhesions that seal the ring. The addition of this injury to the ring was demonstrated to work in an animal model. Blatnik et al. 17 speculated that the addition of minor peritoneum trauma on the internal ring may induce sufficient scarring to provide a more durable repair also in children. Partial lateral peritoneal incision is also safer because it is performed far from the vas and the vessels that may be damaged during complete dissection. 8 In addition, it avoids iatrogenic ascent of the testis. The maneuver is facilitated by the lifting of the peritoneal sheet, as suggested by Montupet and Esposito. 3 We prefer using cold scissors for the peritoneal incision to avoid potential diathermy-spread injuries.
At the same time the two “N” stitches (one that approximates the muscles to the inguinal ligament and the other that closes the remaining peritoneal hedges) make the closure more efficient. In particular, the approximation of the muscles to the inguinal ligament decreases the nonoccluding locus minoris resistentiae, where a new herniation could develop and where recurrences usually occur. 18 The approximation of the conjoint tendon with Poupart's ligament (the Bassini repair) or the use of other modified muscular darns is occasionally required and described in cases when there is a direct hernia or when the internal ring is excessively large in open hernia repair. The aim is to reconstruct and reinforce the floor of the inguinal canal and to reduce the posterior wall weakness that predisposes to recurrences.19–21 The floor reinforcement was part of the repair steps included in the original description by Ladd and Gross. 22 A survey by Levitt et al. 23 showed that 10% of pediatric surgeons perform this step during open inguinal hernia repair.
Back in 1999 a similar approach was proposed in case of a very large internal inguinal orifice. 3 According to Montupet and Esposito, 3 the use of a nonresorbable suture to approach the conjoint tendon to the crural arch and a second peritoneal closure may reduce the recurrence rate.
More recently Shah et al. 12 suggested assessing the approximation of the conjoint muscle with the inguinal ligament in order to perform a double suture when required. In their article the suture between the conjoint tendon and the inguinal ligament is advocated as an explanation for the absence of recurrences, together with the use of the purse-string or Z suture and the authors' laparoscopic experience. Compared with our “double N,” in their “IDES technique” the peritoneal incision is aimed for the complete dissection and excision of the sac.
We suggest using the “double N” technique for patients with defects larger than 1 cm, independently of age and sex.
Conclusions
Laparoscopic repair of inguinal hernia in children carries with it the advantages of a minimally invasive technique with excellent cosmetic results. In addition, it permits the evaluation of both internal inguinal rings and peritoneal folds and thus the identification of bilateral asymptomatic internal rings with minimal patency of the processuss vaginalis and of rare inguinal hernias (such as a direct hernia). Laparoscopy also allows the safe reduction of incarcerated viscera and the diagnosis of associated anomalies. This series shows that our approach is feasible and efficient for laparoscopic inguinal hernia repair in children. Nevertheless, longer follow-up is required for better assessment of the recurrence rate. In addition, prospective comparative studies might be useful to evaluate the efficacy of the “double N” technique compared with other laparoscopic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.