
Abstract
Abstract
As a new surgical technique, extralevator abdominoperineal excision (eLAPE) is recommended for the treatment of low rectal cancer. The patient's position is changed to a prone jackknife position before extralevator excision is performed via the perineal approach. Whether the extralevator excision can be completed through a transabdominal route under laparoscopy is controversial. This study was designed to introduce a modified technique of laparoscopic-assisted eLAPE and to evaluate the feasibility and safety of this technique. With no change of position, laparoscopic eLAPE was performed in 12 patients with low rectal cancer through a transabdominal route between February 2012 and August 2013. There was no case with bowel perforation and positive circumferential resection margins among these 12 patients. The mean operative time was 177.1 minutes, and the mean intraoperative blood loss was 92.5 mL. The mean time to passing of first flatus was 2.3 days, and the mean postoperative hospital stay was 7.5 days. There was no case with bladder dysfunction. No patients suffered from sexual dysfunction during the follow-up period. Without the change of the patient's position, eLAPE can be performed through a transabdominal route by the laparoscopic approach. The procedure of the former eLAPE is simplified without compromising oncologic outcome.
Introduction
S
At our institution, between February 2012 and August 2013, 12 rectal cancer patients received the eLAPE operation through a transabdominal route completed by the laparoscopic approach successfully. By not changing the patient's position, this technique was simplified. The technique we performed is introduced, and the results are presented here.
Materials and Methods
Twelve patients with low rectal adenocarcinoma within 3 cm of the anal verge underwent laparoscopic eLAPE in the cancer hospital of the Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, China. Definite diagnosis was made by colonoscopy with biopsy. Physical examination, abdominal computed tomography scan, abdominal ultrasound, and barium enema were routinely used for preoperative evaluation. Distant metastasis was excluded by imaging examination. Details of each patient's demographics and preoperative pathology are shown in Table 1. Choice of this surgical procedure was strictly based on the patient's individual decision after providing informed consent concerning the method and risks of the procedure. The protocol was approved by the ethics committee of our hospital.
ASA, American Society of Anesthesiologists; BMI, body mass index; F, female; M, male; nCRT, neoadjuvant chemoradiotherapy.
Surgical technique
The patient was positioned in the modified lithotomy position. Four trocars were used: a 12-mm superumbilical port was created to introduce the laparoscopy, and the other three trocars were created in the right lower quadrant (12-mm port), right upper quadrant (5-mm port), and left lower quadrant (5-mm port). The surgeon stood at the patient's right side, the first assistant at the left, and the camera holder at the patient's cranial side. Pneumoperitoneum was created with a pressure of 14–15 mm Hg.
The mesorectum was opened along the Toldt line by an ultrasonic knife. By dissociating the mesorectum along the Toldt's space, the inferior mesenteric artery could be exposed perfectly, and the left ureter could be protected. Then, the inferior mesenteric artery was ligated and cut by an endoscopic linear cutter-straight (model YZB/USA 3859-2010; Ethicon Endo-surgery, LLC, Cincinnati, OH). Lymph nodes of the inferior mesenteric artery pedicle and the mesentery lymph nodes were removed. The mesorectum was mobilized to the edge of the sacropromontory, and the pelvic autonomic nerves should be protected carefully during this procedure.
The posterior side of the rectum was dissociated to the apex of the coccyx bone along the presacral space. The anococcygeal ligament was cut by the ultrasonic knife (Fig. 1a). The right lateral ligament of the rectum was separated first down to the peritoneal reflexion. Then, the left lateral ligament was separated down to the same position. About 0.5 cm above the line of peritoneal reflexion, the peritoneum was opened in an arc line. For male patients, the anterior side of the rectum was dissociated to the lower edge of the prostate. For female patients, the anterior side of the rectum was dissociated to the superior border of the anal aperture.

Transabdominal excision of coccyx rectal ligament and levator ani by the laparoscopic approach:
The next step was to dissociate the bilateral side of the rectum further to the starting points of the levator muscles (Fig. 1b). The right side was dissociated first as before. The levator muscles inside the tendinous arch of the levator ani were cut vertically down to the foot side of the body under direct laparoscopic visualization 13 (Fig. 1c). The two incision lines of the bilateral levator muscles met at the apex of the coccyx bone (Fig. 1d). The sigmoid colon was transected by the endoscopic linear cutter-straight.
After the pneumoperitoneum was released, the perineal operative procedure was started without changing the patient's position. An elliptical incision was made outside of the anus after the anus was closed by double purse-string sutures. Fatty tissue of the ischioanal fossa was dissected. The dissection was continued upward until reaching the pelvic procedure plane completed by laparoscopy (Fig. 2). Then the cylindrical specimen could be removed from the perineal incision.
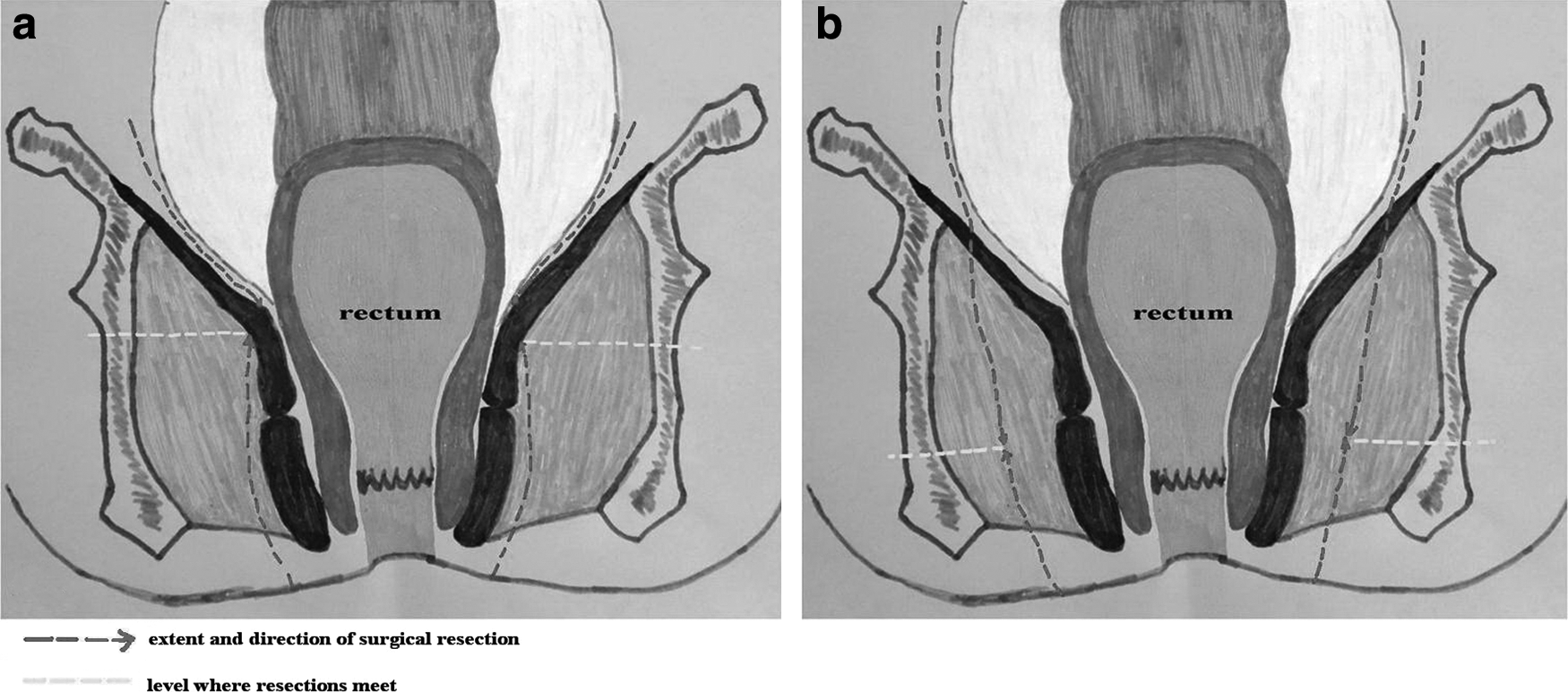
Schematic diagram showing the different surgical extent and plane for
There was no need to close the pelvic peritoneum for female patients with a normal uterus, as the uterus is the natural cover for blocking the intestines from falling. For male patients or female patients whose uterus had been removed owing to various reasons, the pelvic peritoneum was sutured routinely under laparoscopy. The perineal incision was sutured.
Follow-up
All patients were followed up every 3 months with physical examination and laboratory tests, including tumor markers (carcinoembryonic antigen, carbohydrate antigen 19-9). Abdominal computed tomography scan was performed every 6 months after the operation, and endoscopy was performed 1 year postoperatively. For male patients who were younger than 60 years old, sexual function was asked about during a telephone interview.
Results
There was no conversion to open surgery in our study (Table 2). Of these 12 patients, there was no case with bowel perforation and positive CRM. The mean operative time was 177.1 minutes, and the mean intraoperative blood loss was 92.5 mL. The mean time to passing of first flatus was 2.3 days, and the mean postoperative hospital stay was 7.5 days. Bladder function training was started on the second day after the operation, and all catheters were removed on Day 7. There was no case with bladder dysfunction in our study. Sutures of perineal incision were removed on Day 14 after the operation. All perineal wounds were healed by initial treatment. No major complications were found during the perioperative period. Five male patients were followed up for sexual function; no erectile or ejaculatory dysfunction was found in these 5 patients. The follow-up time ranged from 4 to 22 months. During the follow-up time, there was no case with ileus, perineal hernia, local recurrence, or distant metastasis.
CRM, circumferential resection margin.
Discussion
The eLAPE technique for low rectal cancer, reported first by Holm et al. 6 in 2007, was aimed at reducing the incidence of positive CRM and improving the prognosis of low rectal cancer. According to the procedure recommended by Holm et al., 6 a cylindrically shaped specimen could be ensured, and the Morson's waist could be avoided. Advantages of eLAPE have been confirmed by several studies. For example, a study designed by Stelzner et al. 14 verified that the rates of inadvertent bowel perforation, of circumferential margin involvement, and of wound abscesses were 15.2% versus 0% (P=.04), 4.9% versus 0% (P=.511), and 17.4% versus 10.7% (P=.518), respectively, in the conventional abdominoperineal excision versus eLAPE groups. A meta-analysis designed by Yu et al. 15 also showed that eLAPE had a lower intraoperative bowel perforation rate, positive CRM rate, and local recurrence rate than abdominoperineal excision.
Meanwhile, disadvantages produced by the eLAPE technique recommended by Holm et al. 6 cannot be ignored. First, the change of the patient's position from the lithotomy position to the prone jackknife position during the operation would prolong the operation time. 6 We think this process may also result in an increase of wound infection. Second, all levator muscles and coccyx bone should be removed when performing eLAPE. Perhaps some patients will suffer from unnecessary trauma. Third, removal of a large portion of ischiorectal fat in an attempt to create a cylindrical specimen may actually create a large dead space of perineal wound that increases the chances of morbidity. 7 Fourth, excision of the levator muscles via the perineal approach cannot protect the pelvic nerves and vascular structures, and surgeons may enter the pelvic cavity blindly. 13
The laparoscopic approach has been used for the treatment of mature rectal cancer. Based on the advantages of the laparoscopic technique and the experiences of eLAPE performed by different centers, we modified the procedure of eLAPE. Using the laparoscopic technique, we performed this innovative eLAPE for all selected patients successfully.
Avoiding the change of the patient's position may simplify the operative procedure and shorten the operative time. As reported by Holm et al., 6 the prone jackknife position was necessary for transecting the levator muscle through the transperineal approach. Transecting the levator muscle successfully through a transabdominal approach is crucial for the realization of an unchanged position. However, Marecik et al. 12 reported that a transabdominal approach to levator muscle transection could not be realized either through an open or a laparoscopic approach. A different conclusion has been reached by Chi et al., 13 whose study confirmed that making the transabdominal levator transection via the laparoscopic approach to perform eLAPE was feasible. Based on our experience, we thought that an experienced laparoscopic surgeon had the ability to transect the levator muscle through the transabdominal route. Meanwhile, the laparoscopic approach can dissociate perirectal tissue to a lower plane, which makes the perineal operation easier.
The necessity of removing all of the levator muscles and coccyx bone is suspected when the principle of eLAPE, which requires the extra-excised levator muscles encase the mesorectum and make the CRM negative, is followed.6,16 Meanwhile, many experts disapprove of the term “cylindrical,” as this may encourage the removal of a large portion of ischiorectal fat in an attempt to create a cylindrical specimen, 7 and it will make a perineal defect that is more difficult to close.17,18 Excision of the ischioanal fat is not oncologically necessary unless the tumor invades the fatty tissue of the ischioanal fossa. 7 West et al. 7 thought that surgeons were encouraged to follow the extralevator muscle plane and deviated into ischiorectal fat only if absolutely necessary. We thought that the removal of all levator muscles and coccyx bone was unnecessary if no invasion had been found in these tissues by preoperative imaging examination. In our study, we performed controlled levator excision and preserved the coccyx for all 12 patients. Also, we removed different volumes of ischiorectal fat according to the location of tumor. More ischiorectal fat should be removed if a stage T3–T4 tumor is located in the sidewalls of the rectum; otherwise, there is no need to remove too much. All of the 12 specimens had no Morson's waist, and all CRMs were negative in our study.
Performing eLAPE through the transabdominal route by the laparoscopic approach can preserve the pelvic autonomic nerves better because of the clear field of vision and amplification. 13 No case of bladder dysfunction was found in these 12 patients. For the 5 male patients who were younger than 50 years old, there was no case with sexual dysfunction resulting from nerve damage.
In our study, we closed the pelvic peritoneum under laparoscopy without any difficulty for male patients and females without a uterus. For female patients with a normal uterus, this procedure was avoided. But for this kind of patient, at least 7 days were needed for lying in bed.
In conclusion, without the change of the patient's position, eLAPE can be performed through a transabdominal route by the laparoscopic approach successfully. Without compromising oncologic outcome, the former eLAPE procedure 6 is simplified as we reported. No change of the patient's position, relatively minor trauma, and better preservation of pelvic nerves are the advantages of our modified technique. With the limitation of small sample size, a more large-scale study is required to draw a conclusion on the outcome of this modified technique.
Footnotes
Acknowledgments
The authors thank Wei Zheng and Wei Tan for collecting and arranging data of patients. Their support was the key factor in completing this article.
Disclosure Statement
No competing financial interests exist.