
Abstract
Abstract
Background:
More recently, robot-assisted adrenalectomy (RA) has emerged as an attractive alternative to laparoscopic adrenalectomy (LA), and many studies have shown the feasibility and safety of RA. However, the short- and long-term outcomes of RA versus LA have not been adequately assessed, and the advantage over the laparoscopic approach has not been demonstrated. The aim of this study was to compare the outcomes of RA versus LA by means of a systematic review and meta-analysis of the available literature in the early experience.
Materials and Methods:
A systematic search of PubMed, SCI/SSCI, CNKI, and the Cochrane Library was performed to identify prospective randomized controlled trials and retrospective observational studies that compared RA and LA and were published between January 2006 to the end of December 2012. Outcomes of interest included demographic and clinical characteristics, perioperative variables, and complications. The meta-analysis was prepared in accordance with the Quality of Reporting of Meta-analyses (QUOROM) statement.
Results:
Eight trials (232 cases and 297 controls) assessing RA versus LA were considered suitable for meta-analysis, including six prospective and two retrospective studies. There was a significant trend to choose patients for the performance of RA who were associated with a lower body mass index (weighted mean difference [WMD]=−2.78 kg/m2; 95% confidence interval [CI], −3.00 to −2.55; P<.001) and higher incidence of previous surgery (odds ratio=1.59; 95% CI, 0.99–2.54; P=.05). There were no significant differences between the two groups in any other of the demographic parameters. With regard to perioperative variables, although there was a significant difference in the operating time in favor of LA (WMD=17.52 minutes; 95% CI, 3.48–31.56; P=.01), patients having RA might benefit from significantly less blood loss (WMD=−19.00 mL; 95% CI, −34.58 to −3.41; P=.02) and shorter length of hospital stay (WMD=−0.35 day; 95% CI, −0.51 to −0.19; P<.001). There were no significant differences between RA and LA with regard to conversion rates and overall complications. Sensitivity analysis performed by two methods both showed a positive reversal in the operating time with the statistical significance removed compared with the original analysis.
Conclusions:
In the early experience, our data suggest that RA, compared with LA, may be a safe and feasible option associated with less blood loss and shorter hospital stay when performed by experienced surgeons in selected patients.
Introduction
S
In recent years, several investigators have begun to report case series of the robot-assisted approach to adrenalectomy compared with traditional laparoscopic techniques, which demonstrated the surgical feasibility of this procedure with lower surgical blood loss, shorter hospital stay, and even fewer complications.10–17 However, the short- and long-term outcomes of RA versus LA have not been adequately assessed, and no standard conclusive data are available. Therefore, we here performed a systematic review and meta-analysis of the available published literature to compare the outcomes between RA and LA in the early experience.
Materials and Methods
Study selection
A systematic literature search was performed using Medline (using PubMed as the search engine), Ovid, and the Cochrane Library to identify all studies published from January 2006 up to and including December 2012 that compared RA and LA. The following medical subject heading search terms were used: “comparative studies,” “robot-assisted adrenalectomy,” “laparoscopic adrenalectomy,” and “adrenal tumors.” The “related articles” function was used to broaden the search, and all titles, abstracts, studies, and citations scanned were reviewed.
Data extraction
Two reviewers (K.T. and H.X.) extracted independently the following data: first author, year of publication, country, study interval, study design, number of patients who underwent RA or LA, rate of conversion, matching/comparable variables of each study, and outcomes of interest. All disagreements about eligibility were resolved by a third reviewer (X.Z.) by discussion until a consensus was reached.
Inclusion criteria and exclusion criteria
In order to be included in the analysis, studies were required (1) to compare RA with LA, (2) to report on at least one outcome of interest mentioned below, and (3) to clearly document the technique as RA or LA. When two studies were published by the same institutions and/or authors with a potentially overlapping patient sample, the most recent and/or the most informative was included unless the articles were reporting on different outcomes or on different populations.
Studies were excluded from the meta-analysis if (1) the inclusion criteria were not met or (2) no outcomes of interest (specified later) were reported or it was impossible to calculate or extrapolate the necessary data for either RA or LA from the published results.
Outcomes of interest
The clinical outcomes that were analyzed and compared between RA and LA included patient baseline characteristics (age, proportion of males, body mass index [BMI], tumor laterality, operative approach, previous surgery, tumor size, and pathology results [primary hyperaldosteronism, pheochromocytoma, Cushing's syndrome, and nonfunctioning]) and intraoperative outcomes (operating time, estimated blood loss, length of hospital stay, conversion rate, and overall complications).
Study quality and level of evidence
The level of evidence of included studies was rated according to criteria by the Centre for Evidence-Based Medicine in Oxford, United Kingdom. 18 The methodological quality of all nonrandomized studies observational studies was assessed using the Newcastle–Ottawa Scale. 19 A score of 0–9 (allocated as stars) may be given to individual studies. Studies achieving a score of 7 or more stars indicated a higher quality. Two reviewers (K.T. and H.X.) independently assessed the quality of the studies, and disagreement was resolved by consensus.
Statistical analysis
The present meta-analysis was performed according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUOROM) guidelines. 20 The weighted mean differences (WMDs) and the odds ratios (ORs) were used to compare continuous and dichotomous variables, respectively. If continuous variables were measured in different units, the standardized mean differences were used. All outcomes were reported with 95% confidence intervals (95% CIs). For continuous variables, we calculated the difference in mean values and the 95% CI between LA and open adrenalectomy. This method requires that the study report the standard errors of the mean, the standard deviations, or the CIs. However, some studies that did not report any of these parameters but presented continuous data as medians and ranges; under this circumstance we made an approximate transformation using the technique described by Hozo et al. 21 For dichotomous variables derived from contingency tables, the ORs and 95% CI were computed. An OR significantly <1 favored RA, whereas an OR significantly >1 favored LA. All P values are two-tailed with a significant level at .05.
A fixed-effects meta-analysis was performed, and the quantity of heterogeneity was assessed using chi-squared and I2 statistics with significance set at P<.05 providing evidence of significant heterogeneity. For outcomes detected with higher values of I2 and the chi-squared statistic signified increasing levels of inconsistency between studies and significant interstudy heterogeneity, then a random-effects meta-analysis model was adopted. Egger's test was used, and funnel plots were explored to determine the presence of publication bias.
Sensitivity analysis was carried out by considering studies with randomized controlled trials or high-quality studies that achieved a score of ≥7 stars that were conducted before and published in 2012/2013. Variables were pooled only if outcomes reported by three or more studies in the overall meta-analysis.
Statistical analysis was performed using Review Manager (RevMan) version 5.1 software (The Cochrane Collaboration, London, United Kingdom) and the metareg procedure STATA version 12.0 (StataCorp, College Station, TX).
Results
Characteristics of eligible studies
Eight studies including 459 cases (232 cases and 227 controls) assessing RA versus LA fulfilled the predefined inclusion criteria and were considered suitable for meta-analysis, including six prospective and two retrospective studies (Fig. 1).

Flow chart of studies identified, included, and excluded. RCT, randomized controlled trial.
Quality of the studies and level of evidence
For the nonrandomized controlled trial studies, the Newcastle–Ottawa Scale quality assessment method 19 and the U.S. Preventive Services Task Force grading system 18 were used to assess the quality of every study included in our meta-analysis. Only one randomized controlled trial 15 scored Level 2b; the remaining prospective and retrospective studies were all Level 3b. Seven studies10–16 scored ≥7 stars and were considered to be of high quality. Also, the demographics, rate of conversion, comparable variables of RA versus LA, and follow-up time were extracted individually from each study and are listed in Table 1.
Level of evidence (LOE) based on the U.S. Preventive Services Task Force grading system. 18
Matching/comparable variables: 1=age, 2=gender, 3=body mass index, 4=previous surgery history, 5=laterality, 6=approach, 7=indication, 8=tumor size, 9=conversion.
Mean±standard deviation or median (range).
Based on the Newcastle–Ottawa Scale. 19
LA, laparoscopic adrenalectomy; NA, data not available; RA, robot-assisted adrenalectomy; RCT, randomized controlled trial.
Outcomes of demographics and clinical characteristics
There was a significant trend to choose patients whose procedure was performed with RA who were associated with a lower BMI (WMD=−2.78 kg/m2; 95% CI, −3.00 to −2.55; P<.001) (Fig. 2) and higher incidence of previous surgery (OR=1.59; 95% CI, 0.99–2.54; P=.05) (Fig. 3). The patients in the two groups were similar with respect to age (WMD=0.36 years; P=.69), proportion of male patients (OR=1.00; P=.99), proportion of right sided (OR=0.79; P=.21), proportion of left sided (OR=1.34; P=.11), lateral transabdominal approach (OR=0.79; P=.40), posterior retroperitoneal approach (OR=1.31; P=.32), tumor size (WMD=0.05 cm; P=.85), and pathological results, as shown in Table 2.
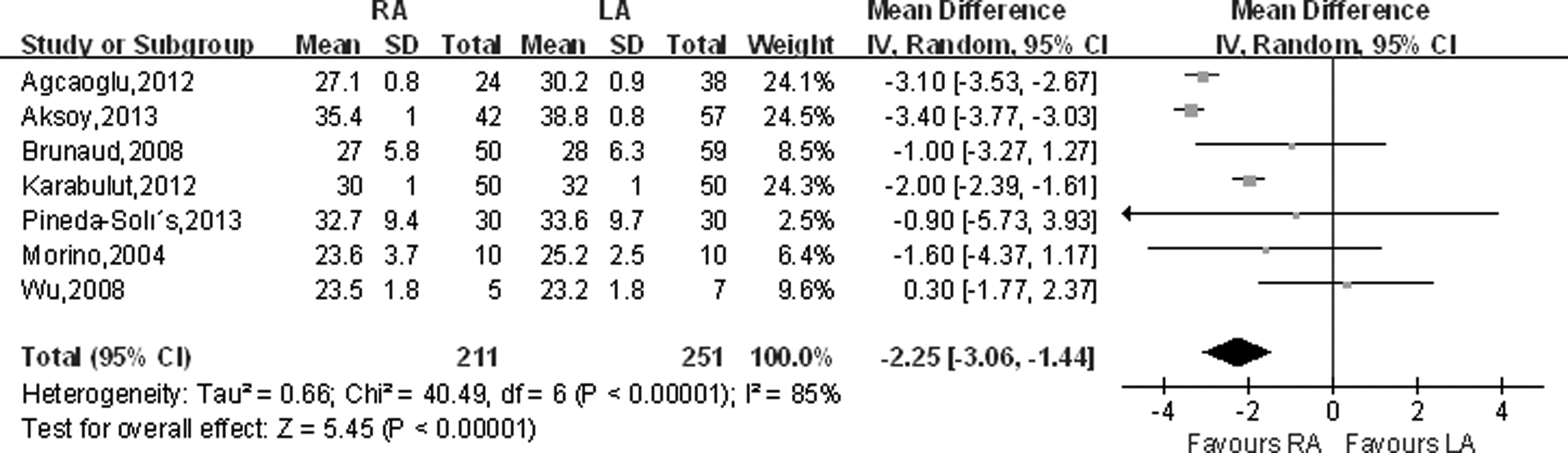
Forest plot and meta-analysis of body mass index. CI, confidence interval; IV, inverse variance; LA, laparoscopic adrenalectomy; RA, robot-assisted adrenalectomy; SD, standard deviation.
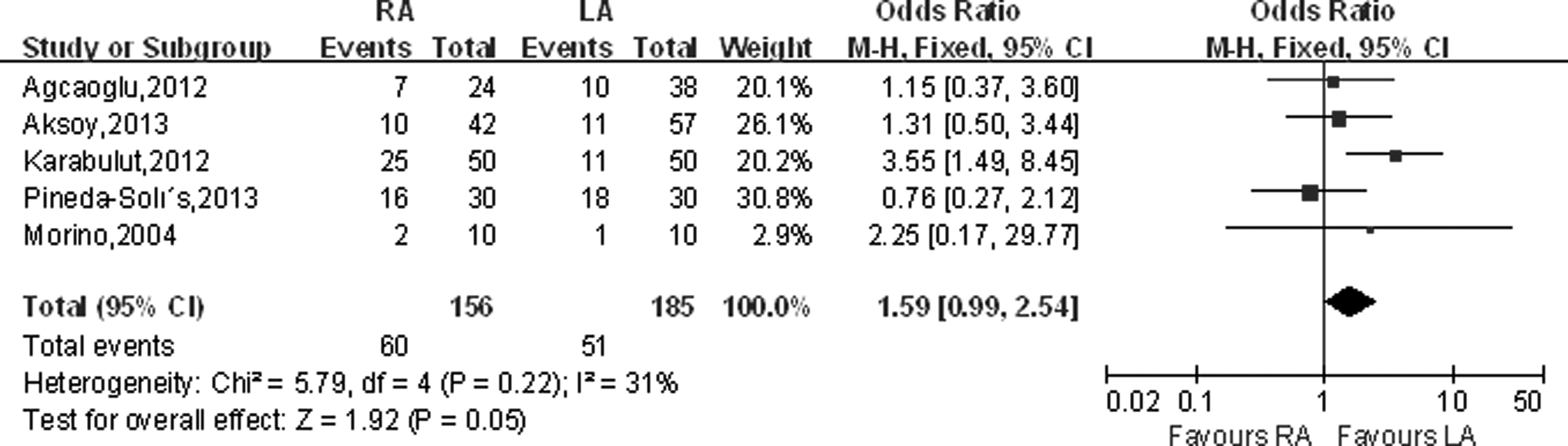
Forest plot and meta-analysis of previous surgery. CI, confidence interval; LA, laparoscopic adrenalectomy; M-H, Mantel–Haenszel; RA, robot-assisted adrenalectomy.
Values of weighted mean difference (WMD).
Statistically significant result.
ACA, adrenocortical adenoma; ACC, adrenocortical carcinoma; BMI, body mass index; CI, confidence interval; LA, laparoscopic adrenalectomy; OR, odds ratio; RA, robot-assisted adrenalectomy.
Outcomes of perioperative variables
With regard to perioperative variables (Table 3), pooled data from the eight studies11–18 that reported operating time between RA and LA showed a significant difference (WMD=17.52 minutes; 95% CI, 3.48–31.56; P=.01) (Fig. 4). Patients having RA might benefit from significantly less blood loss (WMD=−19.00 mL; 95% CI, −34.58 to −3.41; P=.02) (Fig. 5) and shorter length of hospital stay (WMD=−0.35 days; 95% CI, −0.51 to −0.19; P<.001) (Fig. 6). There were no statistically significant differences between RA and LA in terms of conversion rate (OR=0.88; 95% CI, 0.39–1.95; P=.74) (Fig. 7) or overall complications (OR=0.69; 95% CI, 0.32–1.51; P=.35) (Fig. 8).
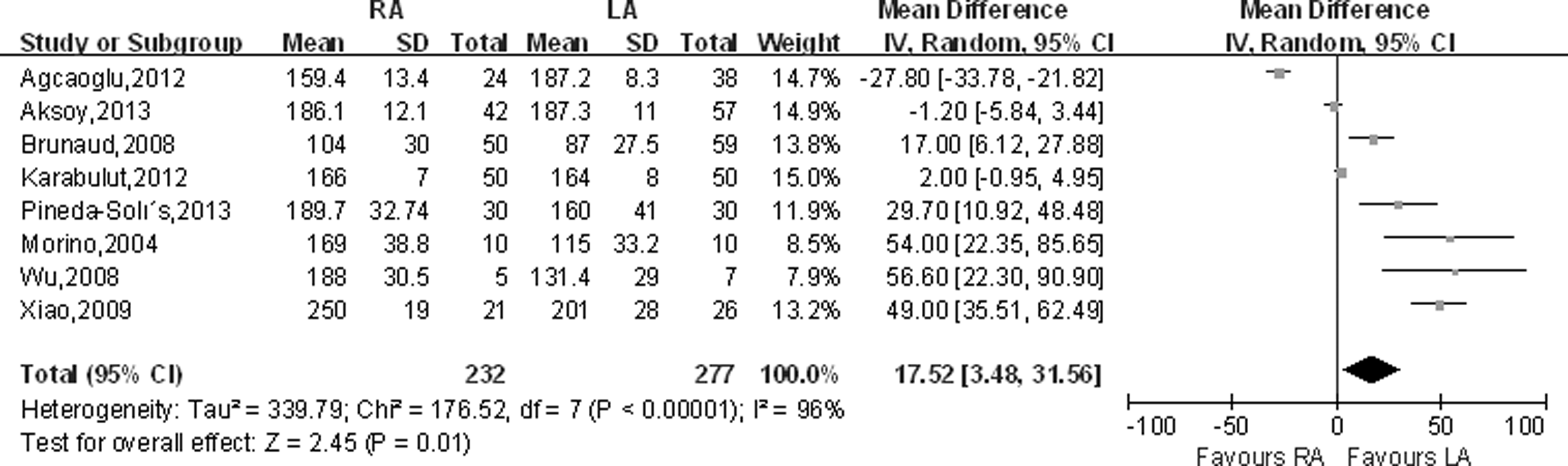
Forest plot and meta-analysis of operative time. CI, confidence interval; IV, inverse variance; LA, laparoscopic adrenalectomy; RA, robot-assisted adrenalectomy; SD, standard deviation.
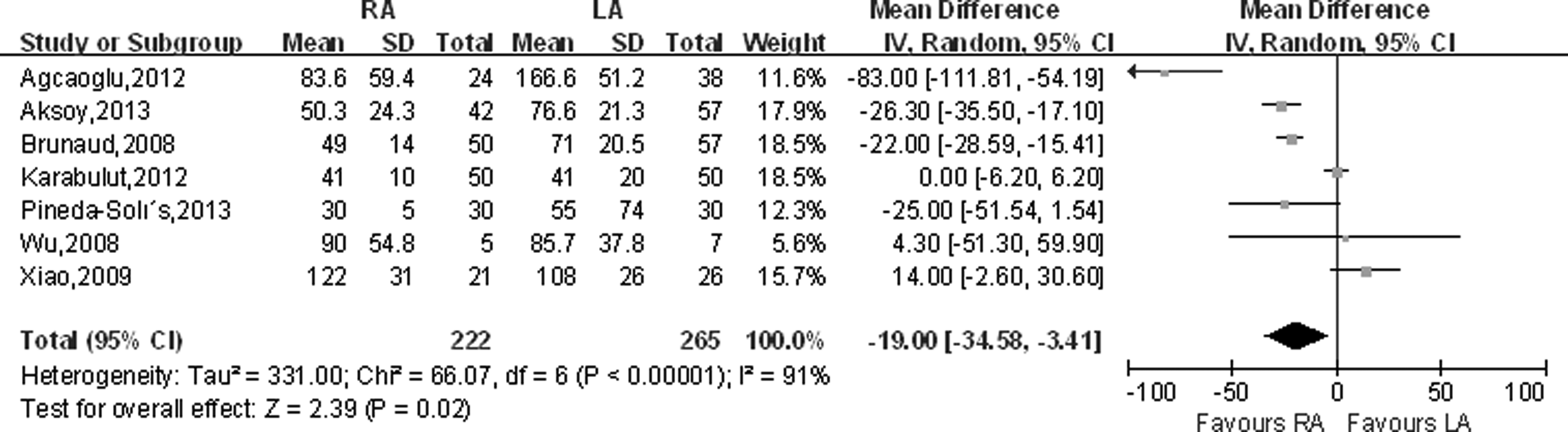
Forest plot and meta-analysis of estimated blood loss. CI, confidence interval; IV, inverse variance; LA, laparoscopic adrenalectomy; RA, robot-assisted adrenalectomy; SD, standard deviation.
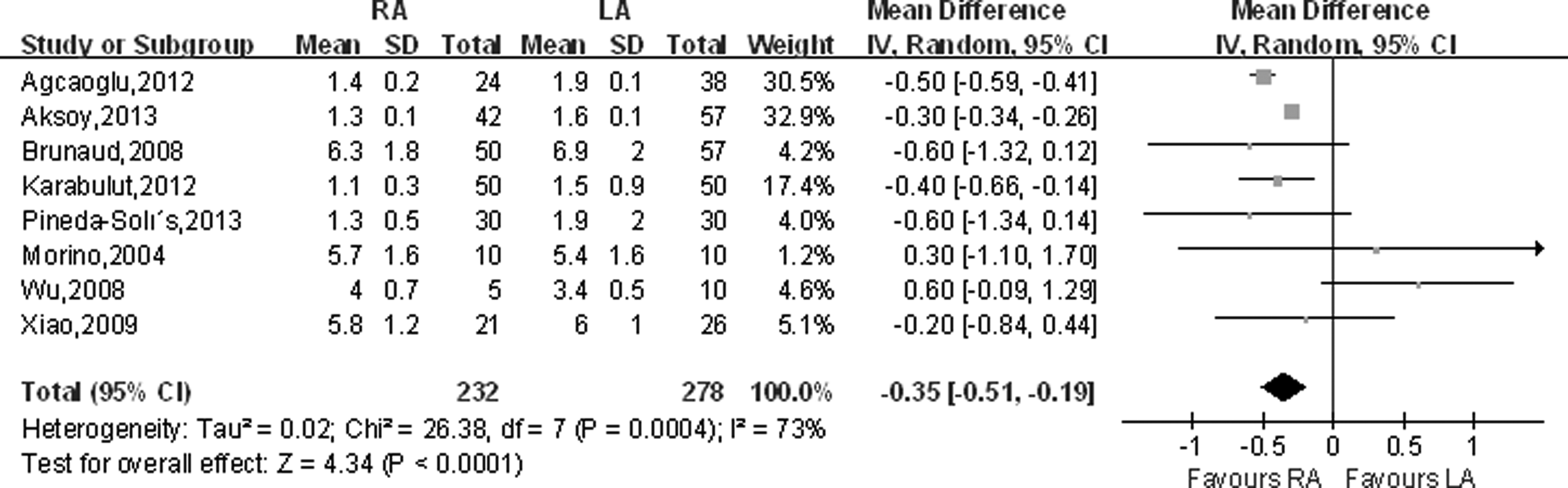
Forest plot and meta-analysis of length of hospital stay. CI, confidence interval; IV, inverse variance; LA, laparoscopic adrenalectomy; RA, robot-assisted adrenalectomy; SD, standard deviation.
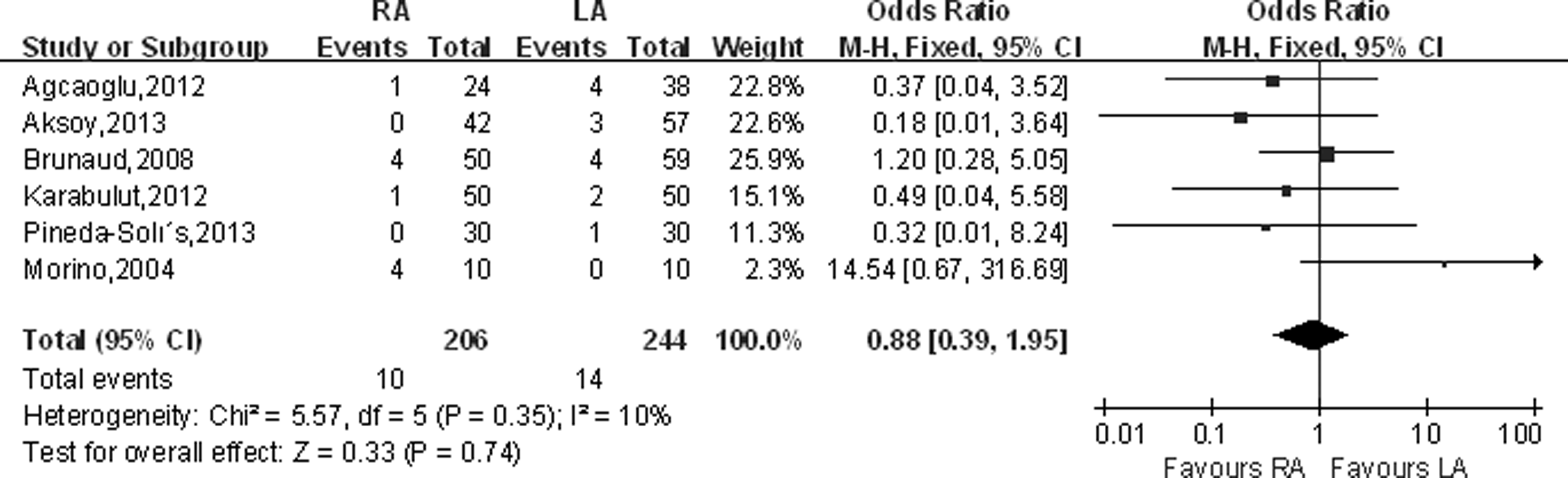
Forest plot and meta-analysis of conversion rate. CI, confidence interval; LA, laparoscopic adrenalectomy; M-H, Mantel–Haenszel; RA, robot-assisted adrenalectomy.

Forest plot and meta-analysis of overall complications. CI, confidence interval; LA, laparoscopic adrenalectomy; M-H, Mantel–Haenszel; RA, robot-assisted adrenalectomy.
Statistically significant result.
Values of odds ratio (OR).
CI, confidence interval; EBL, estimated blood loss; LA, laparoscopic adrenalectomy; LOS, length of hospital stay; RA, robot-assisted adrenalectomy; WMD, weighted mean difference.
Sensitivity analysis and publication bias
Sensitivity analysis (Table 4) was carried out for studies matched for general variables by two methods of higher-quality studies and studies published in 2012/2013. When studies with higher quality and published in the year 2012 were analyzed separately, there was no significant difference in operating time (WMD=11.45 minutes; 95% CI, −1.81 to 24.71; P=.09 versus WMD=−1.44 minutes; 95% CI, −16.30 to 13.43; P=.85, respectively). There was no change in the significance of any other outcomes in sensitivity analysis performed by high-quality studies, as well as another sensitivity analysis performed by four studies published in 2012/2013. The funnel plots and Egger's tests (Tables 2 and 3) revealed that no significant publication bias existed in the 20 comparisons performed in the present analysis.
Statistically significant result.
Values of odds ratio (OR).
CI, confidence interval; EBL, estimated blood loss; LA, laparoscopic adrenalectomy; LOS, length of hospital stay; RA, robot-assisted adrenalectomy; RCT, randomized controlled trial; WMD, weighted mean difference.
Discussion
Less than a decade after LA, RA was first reported in 1992 and 1999 using the AESOP and da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA), respectively.1,7 Since then, a few series have been published about da Vinci RA and have demonstrated the feasibility and safety of RA. Here we first conducted a systematic review and meta-analysis of comparative studies of RA versus LA in the early experience. There was a significant trend to choose patients having a lower BMI and a higher incidence of previous surgery in the RA group. Pooled data indicated significantly less blood loss and shorter hospital stay in the RA than the LA group. Conversion rates and overall complications were comparable between the two groups.
Selection bias therefore may exist in patients whose procedure is performed with RA, as the surgeons may choose patients who are generally fitter to ensure robotic technical ease. In this meta-analysis RA seemed to have a lower BMI (WMD=−2.78; P<.001) and a higher incidence of previous surgery (OR=1.59; P=.05), which showed there was potential bias in selection of patients for BMI and previous surgery. Conversely, RA may have a potential advantage on the management of patients who had a higher incidence of previous surgery.
Operating time is a reasonable parameter to evaluate when determining the efficacy of a new surgical technique designed to improve a preexisting operation. 22 Our data showed that there was a significant difference in the operating time in favor of LA (WMD=17.52 minutes; P=.01); however, sensitivity analyses performed by two methods when the study by Xiao et al. 17 and the studies by Brunaud et al., 12 Morino et al., 15 Wu et al., 16 and Xiao et al. 17 were removed both showed a positive reversal in the operating time, with the statistical significance removed compared with the original analysis. Brunaud et al. 12 also reported that the difference in operative time was not significant after the learning curve of 20 cases. We believe this was mainly attributed to the lack of robotic instruments specifically designed for laparoscopic surgery due to the docking of the robot. In robotic surgery, after the ports are placed, the robot tower must then be docked, and instruments must be inserted. Considering robot-assisted as a new procedure for adrenalectomy, perioperative outcomes are clearly tied to a surgeon's experience, and because introducing a new technique requires a learning curve, we acknowledge that it will probably shorten with improved experience, with an increase in the turnover time for back-to-back cases.23–25
It appears that robotic adrenalectomy can offer better control of bleeding, resulting in less estimated blood loss. Although this difference was statistically significant, it is probably not clinically relevant. Decreased estimated blood loss may be explained by a more precise dissection when using the robotic system.26,27 Length of hospital stay is another important factor to take into consideration when comparing RA to LA. In our analysis, we show a relatively short stay with a mean of 0.35 days. It is largely associated with lower estimated blood loss and similar overall complications, so RA immeasurably improved the postoperative recovery in these patients.
Results from comparison of perioperative outcomes in terms of conversion rate and overall complications between RA and LA are similar. The conversion rate of the robotic approach is reported to be between 0% and 40% in the literature and 0% to 10.5% for laparoscopic to open. We attributed this problem mostly to the specific pathology, the diameter of the lesions, the interference between the robot arms, and the lack of a bipolar energy source for the hemostasis. As a consequence, in some cases dissection and hemostasis became hazardous or difficult to manage, prompting the surgeon to convert to traditional laparoscopy. As the technology advances and new multi-use instruments are developed, we can expect these difficulties to be ameliorated. Nevertheless, the learning curve also played a major role in determining the conversion rate. Second, when comparing RA with LA, our data show no difference in terms of overall complication. In fact, the overall complication rate for RA has been reported to be 0%–20%, and that for LA as 0%–15.3%. The overall complication rate, however, appears to be related to the pathology (pheochromocytoma and adrenal cortical carcinoma) and medical condition of the patient (severe systemic disease), rather than to the procedure itself, which achieved the same operating time, minimal blood loss, and similar conversion rate. 28
In an attempt to find whether RA was appropriate for removing large adrenal tumors, Agcaoglu et al. 10 showed that it could shorten operating time and decrease the rate of conversion to open for adrenal tumors larger than 5 cm. Although benefits of robotic instruments and a three-dimensional imaging platform are evident for facilitating dissection, Aksoy et al. 11 found that the difficulty in maintaining exposure in obese patients nullifies these benefits, and there was no significant difference in perioperative outcomes between RA and LA in obese patients (BMI>30 kg/m2). Brunaud et al. 12 demonstrated that in patients with a BMI of >30 kg/m2 and large tumors (55 mm), the mean operating time was longer in the LA group but not in the RA group; conversion rate, morbidity, and hospital stay were similar in both groups. Morino et al. 15 and Xiao et al. 17 both indicated that the total cost of RA was significantly higher than that for LA. The increased expense was mainly due to the use of semidisposable robotic instruments and the longer operative time. Although robotic surgery has been reported to be 1.2–3.2 times more costly than laparoscopy, in high-volume centers with multidisciplinary and increased use of the robot, the cost can decrease to a comparable level between the two approaches. 15 However, cost is still a significant concern for patients choosing robotic surgical procedures.
To assess any impact of study quality on the effect estimates, sensitivity analysis was performed for studies matched for general variables by two methods that showed a positive reversal in the operating time with the statistical significance removed. In terms of estimated blood loss, length of hospital stay, conversion rate, and overall complications, there were no significant differences in the two sensitivity analyses compared with the original analysis. The latter three variables showed still stability even when analysis was performed with one study removed. Between-study heterogeneity was not significant for dichotomous outcomes but was significant for the continuous variables (operating time, estimated blood loss, and length of hospital stay). Year of publication, indication, area, study quality, and sample size of the included studies might contribute to between-study heterogeneity. Heterogeneity decreased but was not abolished when using the random-effects model and performed by the two methods of sensitivity analyses.
However, we should admit that certain inherent limitations could exist in the studies included in the present meta-analysis that should be considered when interpreting our data. The major limitation of this study was the limited number of well-designed nonrandomized prospective studies. Indeed, the only randomized controlled trial randomized only 20 patients. The remaining studies included in our analysis were five prospective and two retrospective studies. Second, clinical and pathologic characteristics of patients were assessed with varying protocols and different levels of surgical expertise, which were of great importance to the oncologic outcomes. Third, short follow-up time in some patients, marked heterogeneity for several continuous variables, and potential bias in selection of patients may have an influence on the confidence of the results, to varying extent. In addition, other potential advantages of RA that still need to be evaluated are perioperative hemodynamic modifications in patients with pheochromocytoma, oncological results in malignant adrenal disorders, and economics for the surgeon.
To the best of our knowledge, this is the first meta-analysis comparing RA and LA that was conducted using the early experience. We applied appropriate method to identify studies, strict criteria with two scales to evaluate the quality of the included studies, different variables (demographic characteristics and perioperative outcomes) to make comparison of the two procedures, and two methods of sensitivity analysis to minimize the effects of heterogeneity. Here, we provide the up-to-date information that may worth reference on the role of RA for adrenal tumors compared with traditional LA.
Conclusions
This present meta-analysis of one randomized controlled trial and five prospective and two retrospective studies including 529 patients (232 RAs and 297 LAs) comparing the safety and efficacy of RA and LA showed that RA may be a safe and feasible option associated with less blood loss and shorter hospital stay when performed by experienced surgeons in selected patients compared with LA. Although the operating time was longer in RA, sensitivity analyses performed by two methods both showed a positive reversal with the statistical significance removed compared with the original analysis. The two surgical techniques appear to be equivalent in terms of conversion rates and overall complications.
Footnotes
Disclosure Statement
No competing financial interests exist.