
Abstract
Abstract
Background:
To provide an optimal operative view for upper abdominal laparoscopic surgery, we developed a liver retraction method using a double-sling suture (DSS). The current report describes this method and compares the clinical results with the liver puncture (LP) retraction method.
Materials and Methods:
The data and video recordings of patients who underwent laparoscopic gastrectomy for gastric adenocarcinoma by a single surgeon from May 2009 to October 2013 were retrospectively analyzed.
Results:
Of the 189 patients included, 73 underwent surgery with the DSS method, and 116 underwent surgery with the LP method. Both groups exhibited no complications directly related to liver retraction. Compared with the LP group, the DSS group had a higher American Society of Anesthesiologists' physical status score, shorter operation time (153.2±42.1 minutes versus 224.8±83.3 minutes [P<.001]), shorter liver retraction time (200.1±76.8 seconds versus 231.4±97.5 seconds [P=.023]), and less elevation of activities of liver enzymes.
Conclusions:
Our DSS liver retraction method provided rapid and safe liver retraction for laparoscopic gastrectomy compared with the LP method. This method should also be useful for other laparoscopic upper abdominal surgery requiring liver retraction.
Introduction
L
Although various techniques of liver retraction have been introduced for laparoscopic surgery, no standard method has been established for laparoscopic gastrectomy.1–9 Hepatic injury associated with liver retraction varies from elevation of liver enzyme activity due to liver necrosis.3,10–17 The optimal liver retraction maneuver should provide a clear operative view, without damaging the liver parenchyma.
Previously, we used a liver puncture (LP) method to provide adequate exposure of the operative field. 4 However, this involves the risk of hepatic injury and subsequent elevation in activities of liver enzymes. Although critical adverse effects have not been experienced with this method, our novel technique was investigated to reduce the risk of hepatic damage.
In this study, we describe a simple and safe liver retraction procedure using polypropylene suture material, which we have called the double sling-suture (DSS) method. The clinical results of this method are compared with those of the LP method.
Materials and Methods
Patients
We retrospectively reviewed a prospectively maintained patient database and video recordings of patients with gastric cancer. Between May 2009 and Oct 2013, in total, 363 laparoscopic gastrectomies were performed by a single surgeon. Of these, 174 patients were excluded from the analysis for the following reasons: application of other liver retraction methods (n=97); medical comorbidity associated with liver disease or abnormal preoperative liver function tests (n=27); unavailable video recording of the liver retraction procedure (n=48); and ligation of the replacing left hepatic artery (n=2). In total, 189 patients were evaluated to compare the two liver retraction methods: DSS method (n=73) and LP method (n=116).
This study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System (protocol number 4-2013-0710).
Port placement
After induction of general anesthesia, a supra- or infraumbilical incision was made, and a 12-mm camera port was introduced into the peritoneal cavity using an open technique (Fig. 1A). The port placements and operative procedures were performed as previously described.18,19 Pneumoperitoneum was established, and the patient was positioned in the 15° reverse Trendelenburg position for the remainder of the operation. Four additional working ports were placed: two 12-mm trocars in the right and left lower quadrant and two 5-mm trocars in the right and left upper quadrant, medial to each side of the 12-mm trocars. The liver was then retracted using the DSS method (Fig. 1B) or LP method (Fig. 1C).
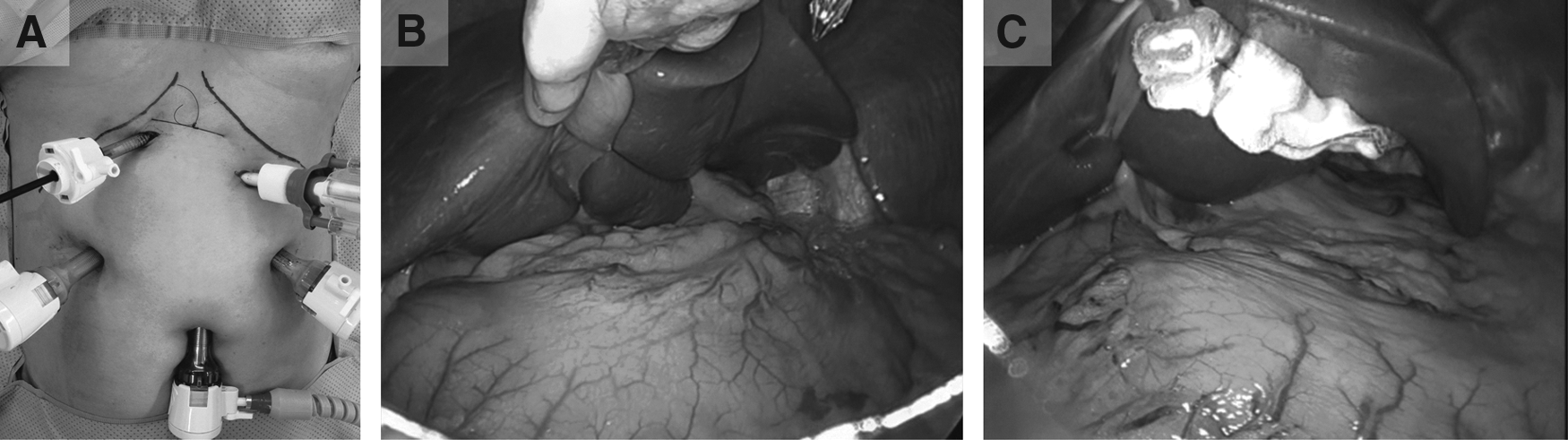
External and internal operative views after each liver retraction method.
Liver retraction
DSS
A 2-0 polypropylene (Prolene®; monofilament polypropylene suture W8400; Ethicon, JJ Medical GmbH, Norderstedt, Germany) suture with two straight needles, one at each at end, was used for the DSS method. Figure 2 depicts the procedure. One of the needles was brought into the abdominal cavity via the 12-mm left lower quadrant trocar. As an assistant raised the left lobe of the liver, the needle was brought forward to the liver hilum—more specifically, the right crus muscle (Fig. 2A). The needle was passed through the right crus muscle (first sling; Fig. 2B) and then pierced the anterior abdominal wall at the subcostal area in the left midclavicular line to become exteriorized (Fig. 2C). This needle was pulled until the other needle was brought into the abdominal cavity (Fig. 2D). The other needle was driven through the avascular portion of the middle of the falciform ligament, in the direction from right to left (second sling; Fig. 2E and F). This needle was brought again to the right side of the falciform ligament (Fig. 2G) and exteriorized on the immediate right side of the falciform ligament (Fig. 2H). Both threads were tied externally, so that the thread lifted up the left lobe of the liver and falciform ligament.

Procedure for the double-sling suture method.
LP
LP was slightly modified from the original report.4,20 The same type of 2-0 polypropylene suture as was used for the DSS method was threaded with a 4-×4-inch X-ray-detectable gauze. The surgeon grasped one needle with the grasper and brought it to the middle of the left lobe of the liver. After the liver was lifted slightly, the needle punctured the liver in the direction from dorsal to ventral. After the needle passed completely through the liver, the other needle was exteriorized just to the right side of the falciform ligament. The two suture ends were tied.
Gastrectomy procedure
Guidelines of the Japanese Gastric Cancer Association were used to determine the extent of lymph node dissection.21,22 Laparoscopic gastrectomy, using an ultrasonic device, was performed as previously described.18,19
Measurements
Patient clinical characteristics and perioperative parameters, including operative time and liver retraction time, were recorded. Liver retraction time was measured reviewing operative video recordings. Laboratory values, including aspartate aminotransferase (AST) activity, alanine aminotransferase (ALT) activity, and total bilirubin level, were determined and compared preoperatively, immediately postoperatively (postoperative day [POD] 0), POD 1, POD 3, and POD 5. AST and ALT activities were measured with the International Federation of Clinical Chemistry and Laboratory Medicine assay without pyridoxal phosphate activation, on a Hitachi-7600 apparatus (Hitachi Ltd., Tokyo, Japan). 20
Statistical analysis
Data were analyzed by SPSS statistical software version 20.0 (IBM SPSS Statistics, version 20.0; IBM Corp., Armonk, NY). For continuous variables, the independent t test was used for comparing mean values. Pearson's chi-squared test was used for analyzing categorical variables. The results were considered statistically significant if the P value was <.05.
Results
Patients
The clinical characteristics of both groups are shown in Table 1. No significant differences were observed between the groups in terms of age, sex, body mass index, history of a previous intraabdominal operation, or pathologic staging. DSS group patients had more medical comorbidities (American Society of Anesthesiologists' physical status score of 1: 17.8% in the DSS group versus 76.7% in the LP group [P<.001]).
Data are mean±standard deviation or number (percentage) as indicated.
P value<.05, considered to indicate a significant difference.
According to the American Joint Committee on Cancer 7th edition.
DSS, double-sling suture; LP, liver puncture.
Surgical outcome
Both methods provided appropriate operative views of the lesser curvature of the stomach and the esophagogastric junction without the need for additional liver retraction techniques, even in the presence of a hypertrophic fatty liver. Only temporary elevation of the left lobe by the grasper was necessary for dissection of lymph node station 1 and dissection around the cardia. No specific intraoperative or postoperative complications associated with liver retraction were identified in either group.
As shown in Table 2, we compared perioperative parameters between the two groups. The DSS group had a significantly shorter operation time (153.2 minutes versus 224.8 minutes [P<.001]), shorter liver retraction time (200.1 seconds versus 231.4 seconds [P=.023]), and less blood loss (45.8 mL versus 90.6 mL [P<.001]). The extent of gastrectomy and lymph node dissection did not differ between groups. Major postoperative complications requiring interventions were similar in both groups (1.7% versus 2.7% [P=.637]). No in-hospital mortality was observed in either group. The mean postoperative hospital stay was 7.0 and 9.4 days in the DSS and LP groups, respectively (P=.025).
Data are mean±standard deviation or number (percentage) as indicated.
P<.01, bP<.05, considered to indicate a significant difference.
DSS, double-sling suture; LP, liver puncture.
Laboratory values
AST activity (Fig. 3A) was significantly lower in the DSS group than in the LP group on POD 0, 1, and 5 (45.2±26.4 IU/L versus 60.4±45.4 IU/L [P=.003], 34.4±23.3 IU/L versus 54.9±54.1 IU/L [P<.001], and 21.6±11.6 IU/L versus 29.45±31.0 IU/L [P=.019], respectively). ALT activity (Fig. 3B) was significantly lower in the DSS group on POD 0, 1, 3, and 5 (38.1±26.7 IU/L versus 57.2±41.8 IU/L [P<.001], 32.7±26.2 IU/L versus 54.6±46.4 IU/L [P<.001], 22.57±21.1 IU/L versus 32.7±36.0 IU/L [P=.013], and 21.0±14.1 IU/L versus 32.6±29.0 IU/L [P<.001], respectively). The total bilirubin level (Fig. 3C) was significantly lower in the DSS group on POD 0 and 1 (0.69±0.29 mg/dL versus 0.84±0.40 mg/dL [P=.002] and 0.87±0.35 mg/dL versus 1.02±0.49 mg/dL [P=.013], respectively).

Liver function tests.
Discussion
In this study, we described our DSS liver retraction technique. Compared with our previously described LP method, the DSS method required no additional preparation on the suture material, provided a better operative view because of removal of gauze, and required less time to perform. Furthermore, liver damage, as monitored by AST, ALT, and total bilirubin, was less after the DSS method than after the LP method.
Liver retraction is one of the most important procedures in laparoscopic gastric surgery because it determines the degree of exposure of the operative field to allow appropriate lymph node dissection around the hepatoduodenal ligament, the celiac artery, and the esophagogastric junction. In addition to the operative view, hepatic damage during liver retraction is also a consideration when choosing the liver retraction method. Mechanical retractors, such as the Nathanson retractor, have been conventionally used, but they require placement of an additional port and the dedicated use of an assistant's hand. Moreover, they can cause iatrogenic liver injury.3,13,23 The LP method, which was adapted from our previous laparoscopic gastrectomy report, is an acceptable alternative. 4 It reduces the number of ports and provides a good operative view. However, it is invasive because liver parenchyma is directly punctured. Although the resulting hepatic dysfunction is transient and may have no long-term oncological effects, injury to healthy organs is not justified if alternatives exist.
Our DSS liver retraction method has several advantages. First, it is quite simple. This method requires basic laparoscopic tools and only one polypropylene suture, without the need for any special preparation or specific instrument(s). Compared with previously reported techniques, which require special equipment, this method involves a use of only one suture material and two intracorporeal sutures.5,6,8 Thus, the time required for the entire procedure is approximately 3 minutes, which is shorter than the time for the LP technique or other methods reported in the literature.2,7,20,23
Second, it is less likely to damage the liver because it does not hamper the hepatic blood supply by mechanical compression. In contrast to previous techniques, 15 no repositioning of the retraction is needed, and the surgeon can focus on the operation without being concerned with the possibility of hepatic necrosis. Postoperative liver dysfunction with the DSS method is comparable to or less than that of the LP technique or other previously reported methods.3,6,20,23
Third, the surgeon can obtain an optimal operative view because there is no bulky protective material, such as gauze, in the area. Because the sling suture runs parallel to the liver surface, no acute angle is encountered between the contact point on the liver surface and the suture material. We identified no liver laceration caused by suture material in our entire DSS cohort, although no protective material was used to cover the suture. Elevated activities of liver enzymes in the DSS group were similar to those for the gauze suture method reported by our institute. 20 This indicates that a protector over the thread is not always necessary to prevent the harmful effects of retraction thread on liver parenchyma, if the whole procedure is ideally performed. In the cases with higher risk of liver damage because of liver cirrhosis, fatty liver disease, or hemangioma on the liver surface, liver laceration was preventable by putting gauze pads between thread and the liver (data not shown and excluded from the analysis).
Despite these advantages, several limitations still exist. First, this method would not be optimal for surgery of cardia cancer invading distal esophagus. In that case, additional LP retraction or an additional trocar for liver retraction would be required. Second, although the DSS group showed a better surgical outcome, cautious interpretation of the data is required. Compared with our recent DSS method, the LP method was adopted for an initial series. Patients in the LP method group underwent operation with ineffective manipulation of the operative field. The data show longer operation time, increased blood loss, increased liver enzyme activities, and longer hospital stays in the LP group. Differences of liver retraction time and liver enzyme activities between the two groups might have been affected not only by the liver retraction method, but also by the learning effect. Although this study has limitations as described, we believe that simplicity and utility of our technique are still effective despite the imbalanced comparison of the two groups.
In conclusion, our DSS liver retraction method provided rapid and safe liver retraction for laparoscopic gastrectomy compared with the LP method. This method should also be useful for other laparoscopic upper abdominal surgery requiring liver retraction.
Footnotes
Acknowledgments
This study was supported by a new faculty research seed money grant (8-2013-0029) of Yonsei University College of Medicine for 2013.
Disclosure Statement
No competing financial interests exist.