
Abstract
Abstract
Background:
When a tumor is located in segment 4 (S4), it is preferable to perform only limited resection of S4, even in laparoscopic surgery. Here we describe anatomical laparoscopic S4, subdivision of S4 (S4a and S4b), and extended S4 segmentectomy for hepatocellular carcinoma (HCC), using the Glissonian pedicle transection method for each, and evaluate the feasibility of laparoscopic liver resection (LLR) for tumors located in S4.
Patients and Methods:
Among 417 patients who underwent LLR for malignant tumors between March 2003 and February 2014, we performed retrospective analysis of the clinical and perioperative outcomes of 10 patients who underwent anatomical liver resection for tumors located in the S4 area of the liver.
Results:
Total laparoscopic anatomic liver resection (S4, extended S4, and S4a and S4b segmentectomies) were performed in 10 patients. There was no open conversion or postoperative mortality. The mean operation time was 316.5 minutes (range, 175–460 minutes), and mean estimated blood loss was 592 mL (range, 100–1600 mL). An intraoperative transfusion was necessary in 2 (20%) of the 10 patients. All patients had negative resection margins. Three patients (30%) had postoperative complications (intraabdominal fluid collection). The mean postoperative hospital stay was 7.7 days (range, 3–13 days). The median follow-up period was 18 months. Intrahepatic recurrence occurred in 2 (20%) of the 10 patients, which was managed by radiofrequency ablation with transarterial chemoembolization in 1 patient and by transarterial chemoembolization alone in the other patient.
Conclusions:
Total laparoscopic anatomical S4, extended S4, or S4a or S4b segmentectomy is a feasible procedure for HCC. The Glissonian pedicle transection method is an effective technique for rapid and safe control and subdivision of the S4 pedicle that facilitates anatomical laparoscopic S4, extended S4, and S4a and S4b segmentectomy.
Introduction
N
Left hemihepatectomy is generally performed for tumors located in segment 4 (S4). However, because left hemihepatectomy entails removal of a large volume of liver tissue, limited resection may be an alternative option. Patients with hepatocellular carcinoma (HCC) commonly have concomitant chronic liver disease or liver cirrhosis that predisposes them to postoperative liver failure after liver resection. In contrast, limited resection surgery, which removes only the diseased area, may reduce postoperative liver failure in these patients.
Although still controversial, anatomical resection for HCC has been reported to have better survival outcomes compared with nonanatomical resection.8–10 A typical anatomical and limited liver resection, which resects only the area of tumor involvement, can be a bisectionectomy, bisegmentectomy, or monosegmentectomy. Our group has previously reported LLR by central bisectionectomy, right posterior sectionectomy, right anterior sectionectomy, and S4 and S5 monosegmentectomy.11–15 When the tumor is confined to S4, resection of the S4 segment alone is advantageous in terms of preserving liver volume. S4 can be subdivided into the superior S4a and inferior S4b regions. Anatomic S4a or S4b resection may also be advantageous for a tumor that is confined to S4a or S4b.
In this study, we describe the technical aspects and feasibility of anatomical S4, S4a, S4b, and extended S4 segmentectomy using laparoscopy.
Patients and Methods
Anatomical LLR for an S4 lesion was performed on 10 of 417 patients who underwent LLR for a malignant tumor at the Department of Surgery at Seoul National University Bundang Hospital, Seoul, Korea, between March 2003 and February 2014. All patients were assessed preoperatively with contrast-enhanced abdominal and pelvic computed tomography and liver magnetic resonance imaging to determine tumor location. The patients' clinical data were retrieved by reviewing their medical records, radiological images, and pathological reports; the data were analyzed retrospectively.
The retrospective analysis of the prospectively collected data was approved by the Bundang Hospital Ethics Committee. All patients provided written informed consent. The nomenclature from the Brisbane 2000 Guidelines for Liver Anatomy and Resection was used to describe the extent of the liver resections.
Surgical technique
Under general anesthesia, the patient was placed in the lithotomy position, with the surgeon standing between the patient's legs. After insertion of a 12-mm umbilical port, a pneumoperitoneum was established by the insufflation of CO2, and the intraabdominal pressure was maintained at a level below 12 mm Hg. A flexible laparoscope (Olympus, Tokyo, Japan) was introduced, and four trocars (one 12 mm, two 10 mm, and one 5 mm) were placed (Fig. 1). The falciform and coronary ligaments were dissected in the cephalic direction using a Harmonic® scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH) until the middle and left hepatic veins were visualized. Intraoperative ultrasonography (IOUS) was performed to confirm the location of the tumor and to ensure an adequate resection margin. The medial resection margin was marked along the right side of the falciform ligament with electrocautery, after which transection of the liver on the medial side was begun. The superficial hepatic parenchyma was transected using a Harmonic scalpel, and the deeper portion of the parenchyma was dissected using a laparoscopic cavitron ultrasonic surgical aspirator (ValleyLab, Boulder, CO). Control of the small veins or biliary branches was achieved with the bipolar sealing system (LigaSure™ sealing device; ValleyLab). During transection of the liver parenchyma, laparoscopic IOUS was repeatedly performed to ensure an adequate resection margin.
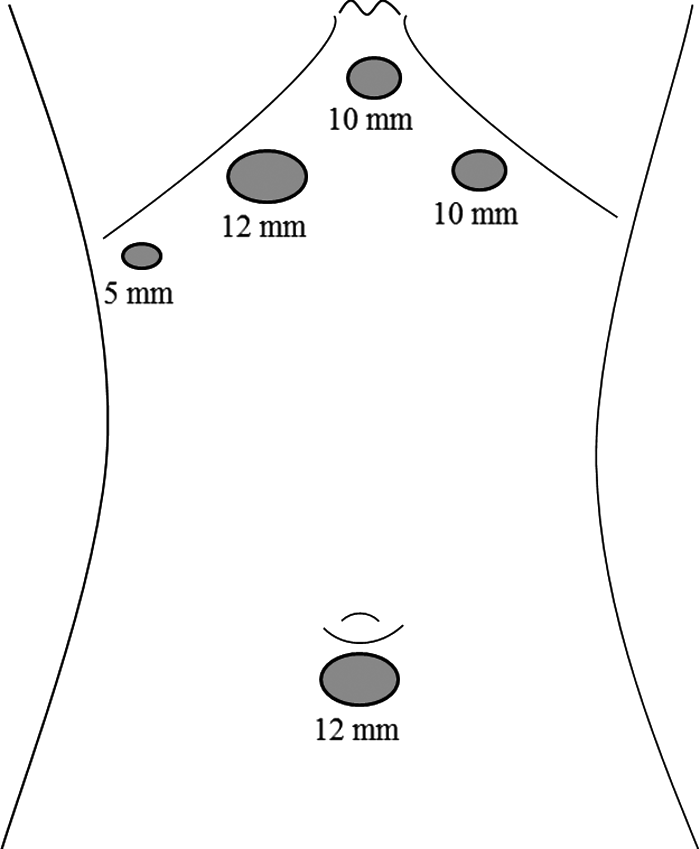
The location of the trocars.
The intrahepatic approach was used to control the S4 Glissonian pedicles. First, parenchymal transection was started along the right side of the falciform ligament, followed by meticulous dissection of the parenchyma to reveal the S4 Glissonian pedicle. The Glissonian pedicles to S4 were then isolated (Fig. 2). If we needed to dissect the subdivisional Glissonian pedicle to S4a or S4b, we performed dissection of the S4 Glissonian pedicle more peripherally to enable identification and isolation of each S4a and S4b pedicle (Fig. 3). To confirm the correct identification, we checked for an ischemic color change in the corresponding area after temporarily clamping the S4a or S4b pedicle. The isolated S4a or S4b pedicle was then ligated and divided with Hem-o-lok® clips (Weck® Teleflex Medical, Research Triangle Park, NC). For example, during S4a segmentectomy, the S4a Glissonian pedicle was isolated and cut while preserving the S4b Glissonian pedicle. The resulting discolored area of S4a (the ischemic line) was then used to mark the transection line on the liver surface, and a parenchymal transection was performed using the marked resection line as a guide. For S4b segmentectomy, the S4b Glissonian pedicle was isolated and cut while preserving the S4a Glissonian pedicle. The Pringle maneuver was used on only 1 patient during the parenchymal transection. Extended S4 segmentectomy was performed if there was invasion of the middle hepatic vein by the tumor in the S4 segment, in which case the S4 segment including the middle hepatic vein was resected.
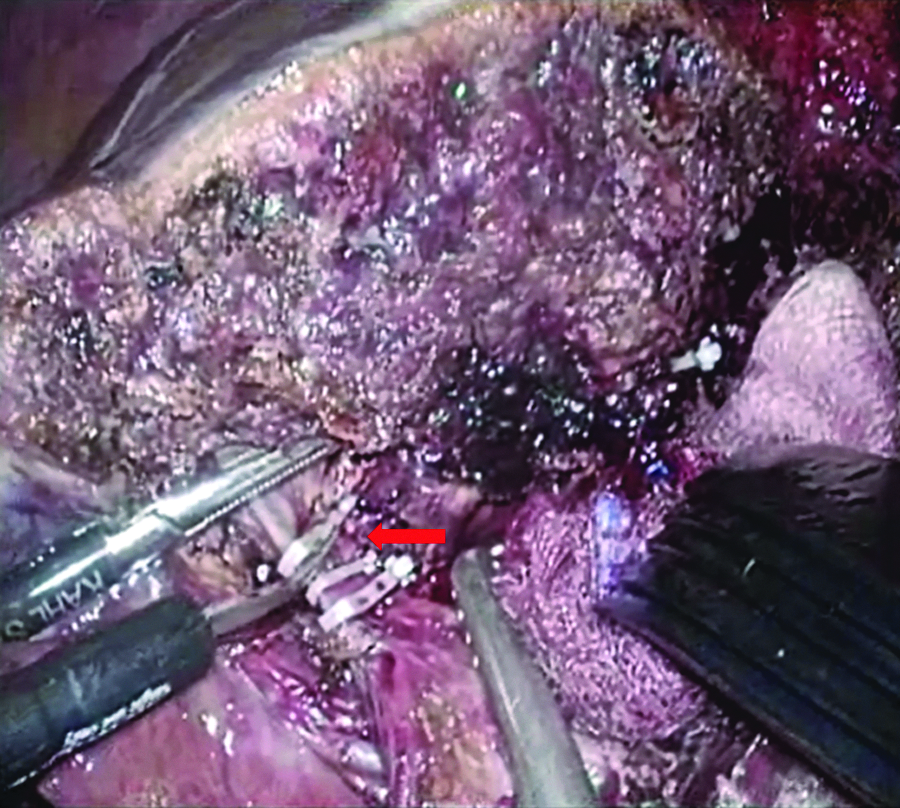
Laparoscopic view of the S4 Glissonian pedicle (arrow).
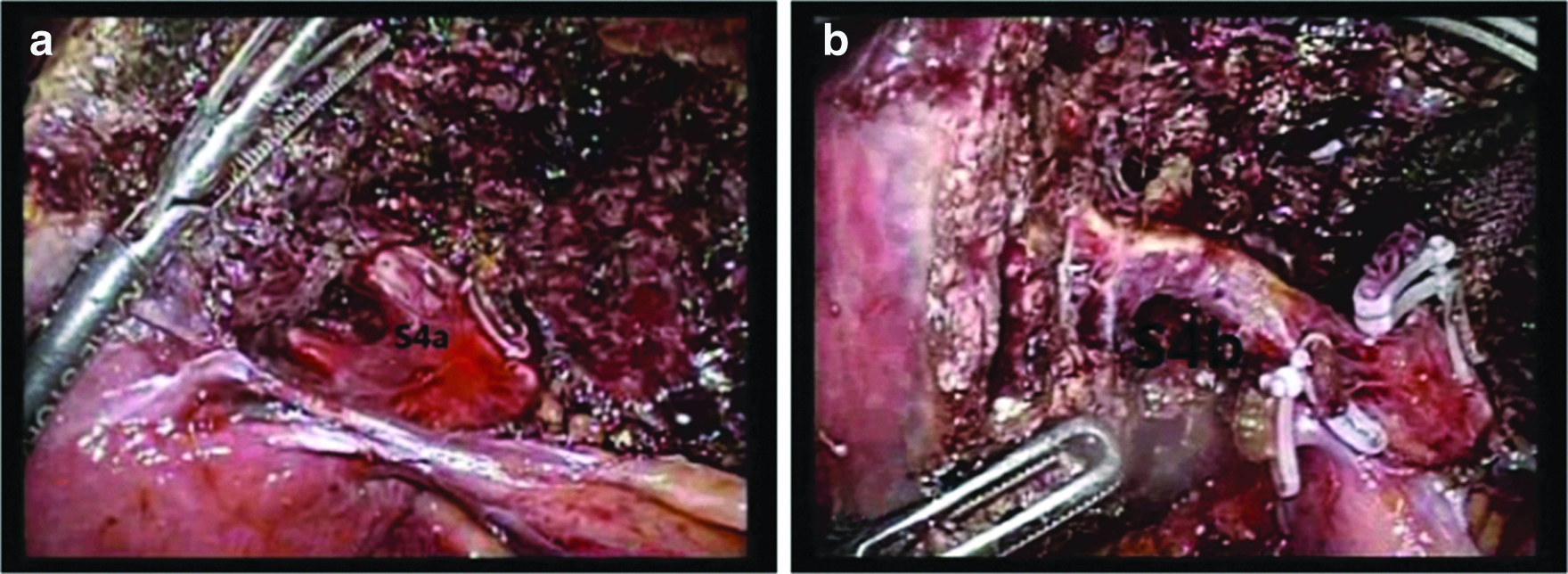
Laparoscopic view of the
In extended S4 segmentectomy, the resection line of the lateral site of S4 was marked 1 cm away from the ischemic line, to include the middle hepatic vein. Transection of the lateral side was continued until the inferior vena cava was reached. Thereafter, the middle hepatic vein was isolated and transected using an endoscopic linear stapler (Ethicon Endo-Surgery, Inc.). Following complete division, the resected specimen was inserted into a vinyl bag and extracted through an extended incision at the subumbilical port. After careful hemostasis, a fibrin glue sealant (Greenplast®; Green Cross Corp., Seoul) was applied to the raw surface. The surgical field was irrigated, a Silastic® (Dow Corning, Midland, MI) drain was inserted, and the wound was then closed in layers.
Results
Patients' characteristics
Of the 10 patients, there were seven men and three women, with a mean age of 65.6 years (range, 53–78 years). The patients' characteristics are shown in Table 1. Comorbidities included 4 cases of underlying chronic liver disease associated with hepatitis B virus infection (n=1) or alcohol abuse (n=3) and an additional 5 cases of liver cirrhosis associated with hepatitis B infection (n=3), hepatitis C infection (n=1), or alcohol abuse (n=1). Only 1 patient had normal liver status. Liver function was classified as Child–Pugh class A in all patients.
HBV, hepatitis B virus; HCV, hepatitis C virus.
Intraoperative and postoperative clinical outcomes
Anatomic liver resection was performed wholly laparoscopically in 10 patients (S4 [n=3], extended S4 [n=2], and S4a [n=1] and S4b [n=4] segmentectomies). Tumor locations and operation performed are shown in Table 2. There were no conversions to open surgery. Perioperative outcomes are shown in Table 3. The mean operation time was 316.5 minutes (range, 175–460 minutes). Intraoperative transfusions were necessary in 2 (20%) of the 10 patients. The mean tumor size was 25.5 mm (range, 17–48 mm), and the mean resection margin was 7.3 mm (range, 1–19 mm). All patients had negative margins without tumor involvement at the resection site. There was no postoperative mortality. Three patients (30%) experienced postoperative morbidity (intraabdominal fluid collection), which was managed conservatively in 2 patients and by percutaneous drainage in 1 patient. The mean postoperative hospital stay was 7.7 days (range, 3–13 days). Tumor recurrence was detected in 2 (20%) of the 10 patients during a median follow-up period of 18 months (range, 1–57 months). These tumors were intrahepatic and distant to the original resection margin. One patient was treated by radiofrequency ablation with transarterial chemoembolization, whereas another patient was treated by transarterial chemoembolization alone. All patients are currently alive.
F, female; M, male; MHV, middle hepatic vein; S4, segment 4.
Discussion
Most patients with HCC have an underlying chronic liver disease or cirrhosis that predisposes them to postoperative liver failure following a major liver resection. Therefore, preserving as much liver tissue as possible during laparoscopic surgery is beneficial to patients. In terms of performing a liver resection, an anatomical versus nonanatomical resection is an important consideration. Because HCC commonly spreads to the portal pedicles in the corresponding regions of the liver, an anatomical resection has a theoretical advantage in terms of oncologic clearance, when compared with a nonanatomical resection. 16 The study of Makuuchi et al. 17 introduced complete or partial anatomical resection of the segment bearing the tumor, based on portal anatomy, using IOUS. Subsequent studies have also demonstrated superior disease-free or overall survival when performing an anatomical resection compared with a nonanatomical resection.8–10
Although LLR is gaining popularity as a surgical strategy, anatomic LLR remains challenging, with the exception of left lateral segmentectomy. A left hemihepatectomy is usually performed when the tumor is located in S4. In left hemihepatectomy, however, the uninvolved left lateral segment is resected as well as S4. Therefore, limited resection of S4 with preservation of the left lateral segment is ideal because this technique preserves as much volume as possible. In addition, a more limited anatomic resection for a tumor confined to the superior or inferior portion of S4, such as S4a or S4b subsegmentectomy, is even more beneficial to the patient as only the involved segment is resected. Further studies on performing laparoscopic anatomical S4, S4a, S4b, and extended S4 segmentectomies are needed to determine whether these procedures are indeed beneficial to HCC patients.
The major concerns associated with laparoscopic S4a or S4b subdivision segmentectomies include maintaining a proper transection line to ensure a safe resection margin and preservation of the vascular structures that supply the remnant liver. Injury to these structures can lead to ischemia or congestion of the remnant liver. The Glissonian pedicle transection technique has been successfully used in our institutions as a method of anatomical liver resection. 11 The laparoscopic Glissonian pedicle transection technique is becoming more popular because it enables anatomy-based resection and can reduce operative bleeding,10,11,18–20 as well as being feasible in cirrhotic patients.10,21 This technique enables complete ischemic demarcation of the liver segments, which facilitates anatomical segmentectomies by guiding the resection plane.
With regard to S4 or subdivision of S4 segmentectomies, the Glissonian pedicles to S4, S4a, or S4b can be isolated during transection between the S4 segment and the left lateral section. After isolation and ligation of the Glissonian pedicle to S4a or S4b, the transection plane between the S4a and S4b segments is determined by the ischemic demarcation line. When the tumor is confined to the S4 subdivision, S4a and S4b resection is preferred. In the case of tumor invasion to the middle hepatic vein, extended S4 resection is preferred.
Laparoscopic IOUS is effective in confirming the spatial relationship of the vascular structures in the deep liver parenchyma. In addition, laparoscopic IOUS helps detect satellite nodules and to confirm the location of HCC-bearing segments.22–25 In our patients, laparoscopic IOUS was useful for performing isolated S4a and S4b segmentectomies, and it was repeatedly used to guide the resection line to ensure that adequate margins were obtained.
A limitation of our study is that we only assessed tumors confined to S4. However, the major advantage of the procedure is that only the liver segment or subsegment involved is resected. Future evaluation of the isolated laparoscopic anatomical resection technique will progress the standard of laparoscopic liver resections performed.
In conclusion, our findings demonstrate that laparoscopic S4, extended S4, S4a, or S4b anatomical segmentectomy is a feasible operative procedure in selected patients, particularly for those with limited liver function. With careful dissection and control of the Glissonian pedicle, the procedure of laparoscopic isolated anatomical liver resection is as feasible as open liver resection.
Footnotes
Disclosure Statement
No competing financial interests exist.