
Abstract
Abstract
The “ALPPS” (associating liver partition with portal vein ligation for staged hepatectomy) procedure enables the rapid growth of the future liver remnant and extended surgical indication to patients with an “insufficient” future liver remnant. In May 2014, a 64-year-old male patient was admitted. The computed tomography (CT) scan showed multiple right liver lesions, which were diagnosed to be hepatocellular carcinoma by liver biopsy. The future liver remnant volume after right hemihepatectomy was calculated to be 35.6% based on the CT reconstruction. Completely laparoscopic ALPPS using round-the-liver ligation, which replaced liver splitting, was performed on him. The two-stage operation was performed successfully. The future liver remnant volume increased 37.9% according to the CT scan on Day 10 after the first-stage operation. The second-stage operation was performed on Day 14 after the first-stage operation. The patient recovered uneventfully. No bile leakage occurred. Thus the round-the-liver ligation can be safely executed in laparoscopy. Completely laparoscopic ALPPS using round-the-liver ligation is feasible and could result in a rapid hypertrophy of the liver remnant in patients with liver cancer complicated with cirrhosis.
Introduction
R
Subject and Methods
Patient
In May 2014, a 64-year-old male patient with multiple liver cancers was admitted to Sir Run Run Shaw Hospital (Hangzhou, China). He was found to have multiple right liver tumors 2 years previously, which were diagnosed to be hepatocellular carcinoma by liver biopsy. He had had radiofrequency ablation done 2 years previously and had had transcatheter arterial chemoembolization 2 months previously. He had had chronic hepatitis B infection for 16 years. The recent computed tomography (CT) scan showed multiple right liver lesions (Fig. 1), liver cirrhosis, and cholelithiasis. The FLR volume after right hemihepatectomy was calculated to be 35.6% based on the result of reconstruction of CT images (using Volume Viewer version 9.6.25b software and GE Advantage Workstation hardware [GE Healthcare, Little Chalfont, United Kingdom]). His liver function was evaluated to be Child A classification. Because of the high possibility of postoperative liver failure, the procedure of completely laparoscopic ALPPS was decided on for him.

The preoperative computed tomography scan showed multiple right liver lesions with iodine deposition (arrows).
Procedure
The first-stage operation, completely laparoscopic ALPPS, was performed with the patient under general anesthesia and in the supine position. A pneumoperitoneum was established with CO2 gas pressure at 14 mm Hg. Four entries were made as previously described, 1 including an observation port (10 mm), a main manipulation port (10 mm), and two assistant ports (5 mm).
The liver was mobilized to well expose the hepatic hilum by the traction of the ligamentum teres. The right hepatic artery and its branches were dissected by meticulous blunt dissection (Fig. 2A). Then the right branch of the portal vein, which was below the artery, was visualized and was further dissected using the same manner. After careful dissection, the right branch of the portal vein was freed and ligated near the bifurcation (Fig. 2B).
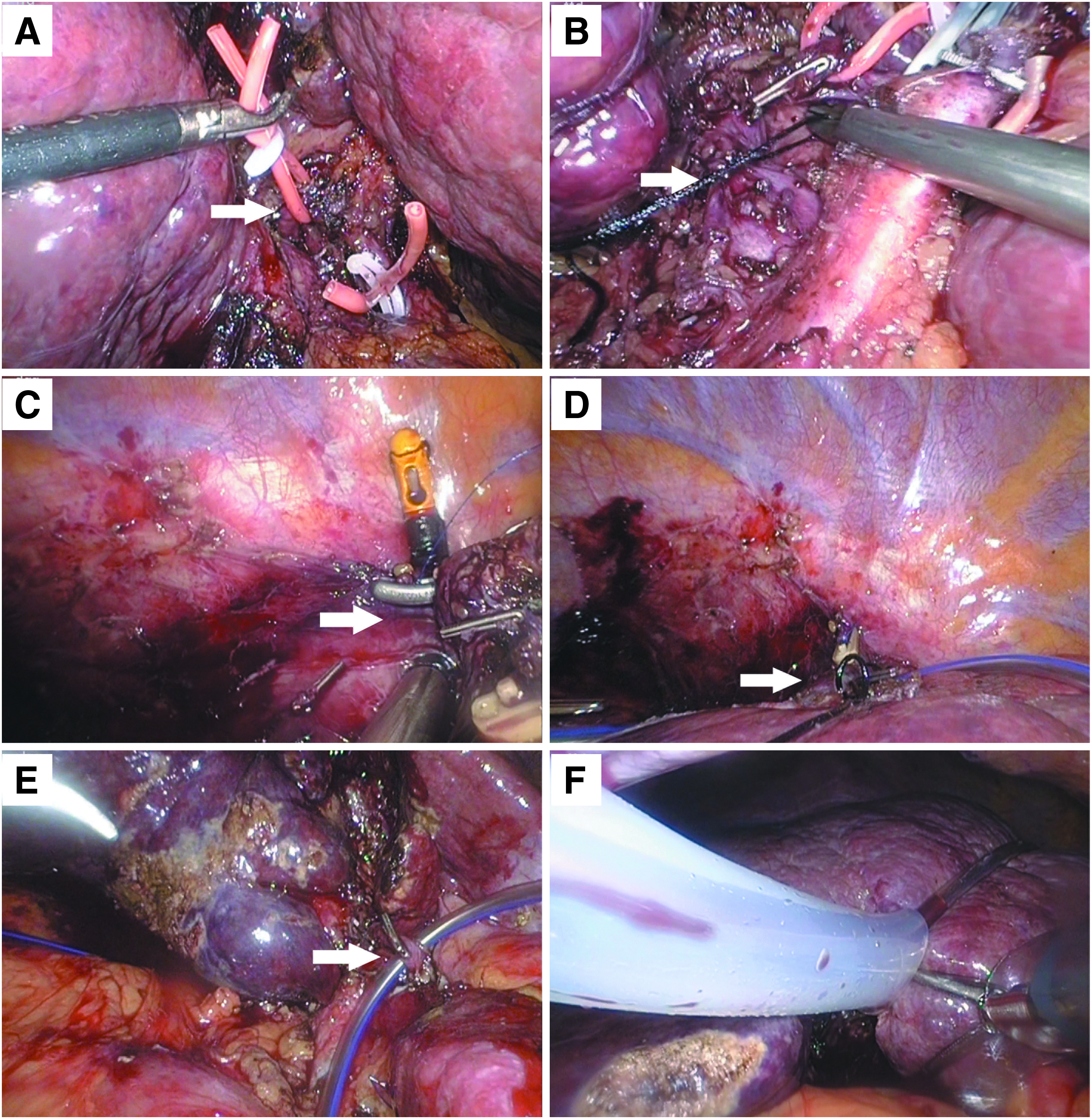
Surgical procedure.
The falciform ligament was divided. Then the patient was tilted 70° to the left. The right coronary ligament and the right triangular ligament were divided. A space under the right lobe was created, and a small hole between the right hepatic vein and the liver surface was created by meticulous dissection (Fig. 2C). Liver lesions were located with laparoscopic ultrasonography, and the future resection line was marked on the liver's surface by electric coagulation. A Flocare® nasogastric tube (Nutricia Flocare, Schiphol Airport, The Netherlands) with a guide wire inside was used as the ligature. It was passed between the right hepatic vein and the liver surface (Fig. 2D) and was further passed between the right hepatic artery and the liver surface (Fig. 2E). The ligature was wrapped around the liver along the future resection line and was closed by the manner that is used in Pringle's maneuver: both ends of the nasogastric tube were passed around a thorax tube, and the ligature was closed by manipulating the thorax tube (Fig. 2F). The thorax tube was passed through the abdominal wall via a small incision, and the ligature was locked with a forceps outside the abdominal cavity.
The second-stage operation, the completely laparoscopic right hemihepatectomy, was performed using the technique of laparoscopic hepatectomy by curettage and aspiration, which was previously described. 2 In brief, the right hepatic pedicle was dissected and divided, the liver parenchyma was transected using the laparoscopic multifunctional operative dissector, and the right hepatic vein was clamped and divided at last. The liver specimen was placed in a specimen retrieval bag and was extracted through a small incision.
Results
The two-stage operation was performed successfully. The operating time of the first-stage operation was 315 minutes, and intraoperative blood loss was 100 mL. The ligation was tightened by manipulating the thorax tube on Day 5 after the first-stage operation. The FLR volume increased 37.9% according to the CT scan performed on Day 10 after the first-stage operation (Fig. 3). The second-stage operation, the laparoscopic right hemihepatectomy, was carried out on Day 14. The operating time was 215 minutes, and blood loss was 300 mL. Atrophy was observed in the liver parenchyma under the ligation in the second-stage operation (Fig. 4), and multiple liver cancers were detected in the specimen (Fig. 5).
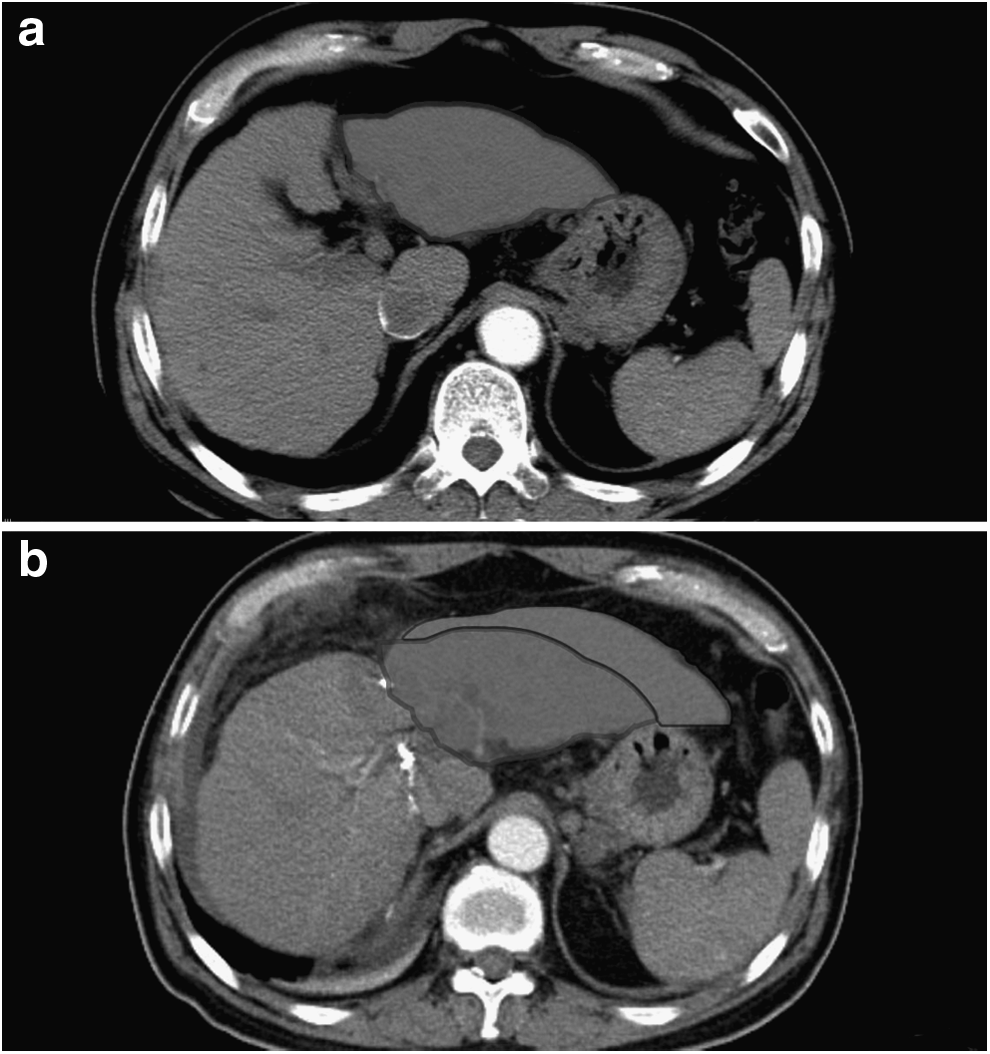
Comparison of computed tomography images
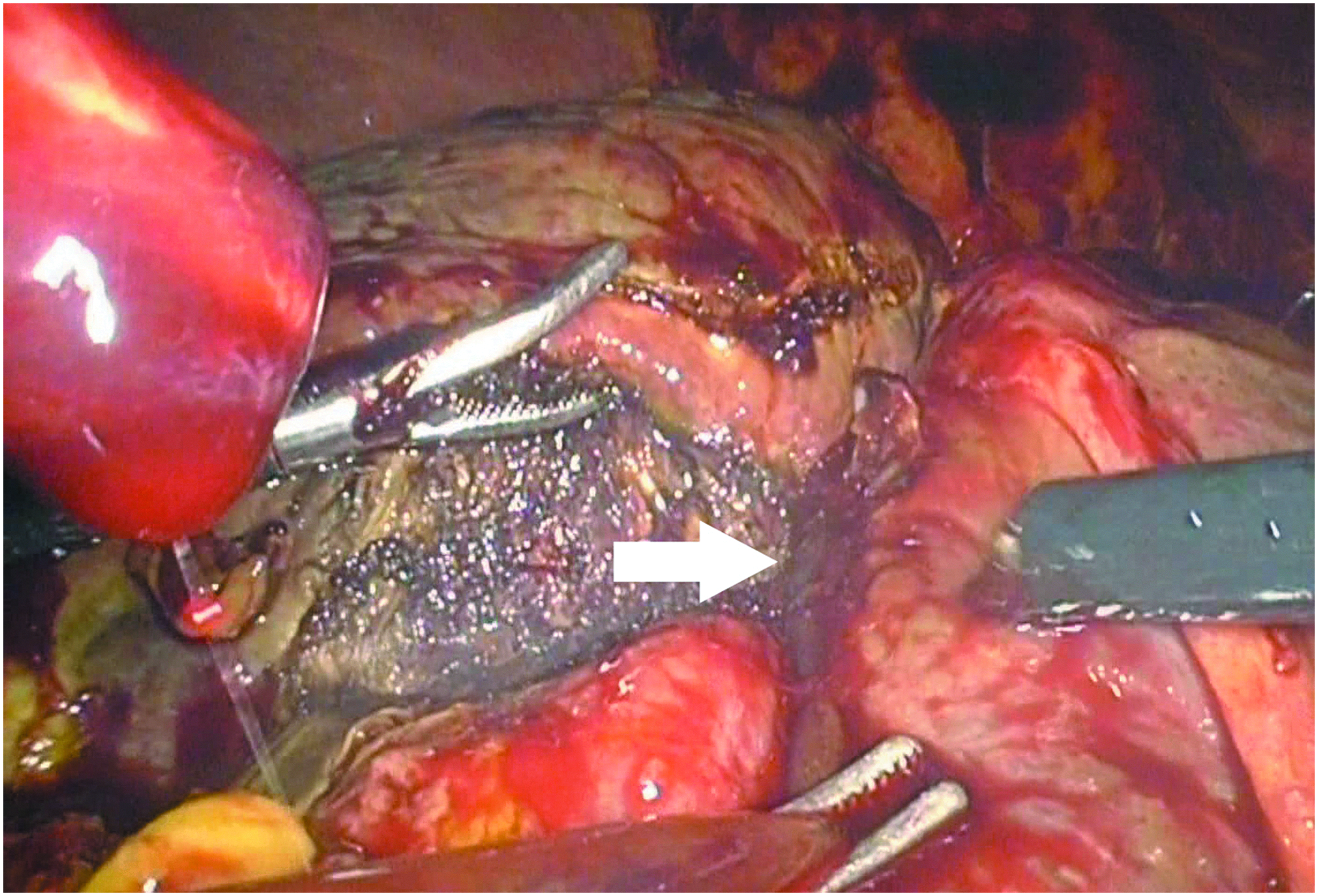
Atrophy was observed in the liver parenchyma under the ligation (arrow) in the second-stage operation.

Multiple liver cancers (arrows) were visualized in the specimen.
The patient recovered uneventfully. No bile leakage occurred. He could have bedside activity on Day 1 after both the first-stage operation and the second-stage operation.
Discussion
The safety of liver resection mainly depends on the function of the FLR. Inadequate FLR volume is associated with a significant increase in postoperative liver failure, especially in patients with liver cirrhosis. Surgical indications for patients with small FLR volumes are always difficult to perceive because of the confliction between safety and oncological radicality. Two effective methods for increasing FLR volume have been adopted: one was portal vein ligation or percutaneous portal vein embolization, and the other was two-stage surgery. However, these methods require several weeks for liver regeneration before resection of the liver malignancy. The risk of tumor progression during the waiting time was a concern for surgeons.3,4 Recently, a new “two-stage” operation, termed ALPPS by de Santibañes and Clavien, 5 is drawing the attention of surgeons. This method enables the rapid growth of the FLR. However, the complication of bile leakage is increased. In the report of Schnitzbauer et al., 6 bile leakage was observed in 24% of the patients, and the mortality was 12%. The safety of ALPPS has been questioned by some surgeons. 7 The procedure of the in situ splitting of the liver was supposed to be the major cause of the high occurrence rate of biliary leakage. This procedure was modified by Robles Campos et al. 8 A round-the-liver ligation was executed to replace liver splitting to avoid the complication of biliary leakage and to simplify the procedure as well.
Totally laparoscopic ALPPS was described by Machado et al. 9 in a letter to the editor in 2012. Unlike in their cases, we adopted the execution of the round-the-liver ligation to replace the in situ splitting of the liver, which could avoid postoperative bile leakage and might simplify the operation. Meticulous laparoscopic dissection was the point of the first-stage operation. The aspiration tube and 90°-angle forceps were good instruments for blunt dissection, which could safely free the branches of the portal vein and hepatic veins. Because of the short interval between the first-stage operation and the second-stage operation, adhesion did not bring much difficulty to the second-stage operation. Only minor adhesion was observed, and it was easy to detach. In addition, the ligation would become loose after the first-stage operation for the gradual atrophy of the liver parenchyma under the ligature, so it is necessary to tighten the ligation a few days after the first-stage operation.
In this case, completely laparoscopic ALPPS using round-the-liver ligation was successfully performed on the patient, whose estimated FLR volume was lower than 40%, to achieve a radical resection of multiple liver malignancies, and a rapid increase of FLR volume was observed. Theoretically, the advantage of minimally invasive laparoscopic surgery would decrease surgical trauma and lead to a lower occurrence rate of postoperative liver failure. The adoption of round-the-liver, which replaced liver splitting, could avoid biliary leakage and simplify the first-stage operation and finally led to a decrease in perioperative morbidity and mortality.
The round-the-liver ligation can be safely executed in laparoscopy. Completely laparoscopic ALPPS using round-the-liver ligation is feasible and could result in a rapid hypertrophy of the liver remnant in patients with liver cancer complicated with cirrhosis. However, this is an initial case. The value of this procedure should be further evaluated.
Footnotes
Acknowledgments
This study was supported by the Fund of Key Lab of Surgery of Zhejiang Province (grant 2010E10002).
Disclosure Statement
No competing financial interests exist.