
Abstract
Abstract
Objectives:
In this study, we report a simple closure technique of the renal parenchyma using a knotless running suture with Hem-o-lok® (Teleflex® Medical, Research Triangle Park, NC) clips (running-clip renorrhaphy) to minimize warm ischemic time (WIT) and reduce intraoperative blood loss (IBL).
Materials and Methods:
From 2008 to 2010, laparoscopic partial nephrectomy (LPN) was performed by traditional interrupted knot-tying suture renorrhaphy (Group I; n=28). Since then, from 2011 to 2013, LPN was performed by running-clip technique renorrhaphy (Group II; n=51). A comparative analysis of WIT and IBL between Groups I and II patients was investigated.
Results:
All the LPNs were performed successfully without open conversion. No significant differences were observed for patients of different ages, body mass indexes, and preoperative estimated glomerular filtration rates. In Group I, the operative time, WIT, and IBL were 170.0±27.0 minutes, 32.3±6.5 minutes, and 369±201 mL, respectively. In Group II, the operative time, WIT, and IBL were 148.7±31.9 minutes, 21.5±5.8 minutes, and 254±162 mL, respectively. There was significant difference in operative time, WIT, and IBL between Groups I and II (P=.004, .001, and .008, respectively).
Conclusions:
The running-clip renorrhaphy reduced operative time, WIT, and IBL during the LPN. Therefore, running-clip renorrhaphy is a safe, efficient, and operative technique for performing the LPN.
Introduction
W
Intracorporeal suturing and knot tying are the most important factors that determine the warm ischemia time (WIT) and intraoperative blood loss (IBL). The sliding-clip renorrhaphy allows a significant reduction in WIT and reduces IBL during LPN compared with the interrupted suture, and the use of surgical clips as the suture anchors has made LPN technically simpler by removing the need for intracorporeal knot tying.4,5
In this study, we demonstrated a simple renorrhaphy closure technique of the renal parenchyma using a knotless running suture with Hem-o-lok® clip (Teleflex® Medical, Research Triangle Park, NC). This technique, termed running-clip renorrhaphy, minimized operative time and WIT and reduced IBL.
Materials and Methods
In total, 79 patients with a small renal mass underwent transperitoneal or retroperitoneal LPN in our institution from January 2008 to May 2013. The data for all the patients were reviewed with the approval of the institutional review board (approval number KC13RISI0679).
All the procedures were conducted by an experienced laparoscopic urologist (S.-H.H.) in our institution. Between 2008 and 2010, the suture technique of the LPN was performed by interrupted sutures with knot tying (Group I). Since then, the LPN technique with running-clip renorrhaphy was used from 2011 to 2013 (Group II). For Group I, the interrupted suture was performed with 3-0 polyglactin 910 (Vicryl®; Ethicon, Somerville, NJ) prior to proceeding with the outer layer of the renal parenchymal suture in the case of an opened pelvocalyceal system or renal defect site bleeding, and a Surgicel® (Ethicon EndoSurgery, Somerville, NJ) bolster was placed on the renal defect site, depending on the size of the renal defect. After that, fibrin sealant (Tisseel™; Baxter Healthcare Corp., Westlake Village, CA) was applied to the approximated edges of the renal parenchyma. The outer layer of the renal parenchymal suture was performed using 2-0 Vicryl by the interrupted suture closure with knot tying. After the suture closure of the renal parenchyma was completed, the vessel clamp, such as a bulldog or Satinsky clamp, was removed. To make sure of bleeding control, the suture site was observed under low-pressure pneumoperitoneum.
In Group II, compared with Group I, 2-0 polydioxanone (PDS; Ethicon) was prepared on the back table by applying a Hem-o-lok clip to the suture's terminal end by cutting to a length of 30 cm. In the presence of an opened pelvocalyceal system and transected blood vessel, the running suture was performed by 15 cm-long 3-0 PDS for closing the collecting system and secure sealing of the vasculature. After the initial suture, the renal parenchyma was initiated outside of the kidney and came out on the inside of the renal parenchyma using prepared 2-0 PDS; the sutures were performed sequentially four or five times in a running manner, and sequential tightening and locking were performed with Hem-o-lok clips. The tightening tension was applied perpendicular to the capsule to reduce the risk of tearing the renal parenchyma. Because the running-clip renorrhaphy was complete, the clamps were removed, and the suture site was inspected to ensure the hemostasis. If significant bleeding occurred, additional sutures or hemostatic agents may be applied to the bleeding site.
We compared patients' demographic characteristics, including patient age, sex, body mass index, and preoperative estimated glomerular filtration rate, which was measured by the Modification of Diet in Renal Disease formula, between the two groups. Intraoperative and postoperative data, including WIT, IBL, operative time measured from the first incision to skin closure, hemoglobin reduction, postoperative eGFR change, complication, and hospital stay were also evaluated and compared between the two groups. Pathological data included tumor type, size, location, and surgical margin.
All the variables are presented as mean±standard deviation values. The perioperative and postoperative variables were evaluated for statistically significant differences between the two groups. Student's t test was used to compare continuous variables, and the chi-squared test was used to compare categorical variables. The reported P values are two-sided, and a P value of <.05 was considered as statistically significant. All the statistical analysis was performed by SPSS® software (SPSS Inc., Chicago, IL).
Results
The demographic characteristics of the patients are listed in Table 1. LPN was performed for 28 patients in Group I and 51 patients in Group II. All the LPNs were performed successfully without open conversion. There was no significant difference between the two groups in the patients' sex, age, body mass index, and preoperative estimated glomerular filtration rate.
BMI, body mass index; eGFR, estimated glomerular filtration rate.
Intraoperative and postoperative outcomes are listed in Table 2. No significant differences in hemoglobin reduction, postoperative creatinine level, and estimated glomerular filtration rate between Group I and II patients were observed. Hospital stay, complications, and preoperative transfusion were similar for the two groups. However, operative time, WIT, and IBL were significantly higher in Group I compared with Group II (170.0±27.0 versus 148.7±31.9 minutes, 32.3±6.5 versus 21.5±5.8 minutes, and 369±201 versus 254±162 mL; P=.004, .001, and .008, respectively).
eGFR, estimated glomerular filtration rate; IBL, intraoperative blood loss; WIT, warm ischemic time.
WIT of each case is shown in Figure 1.
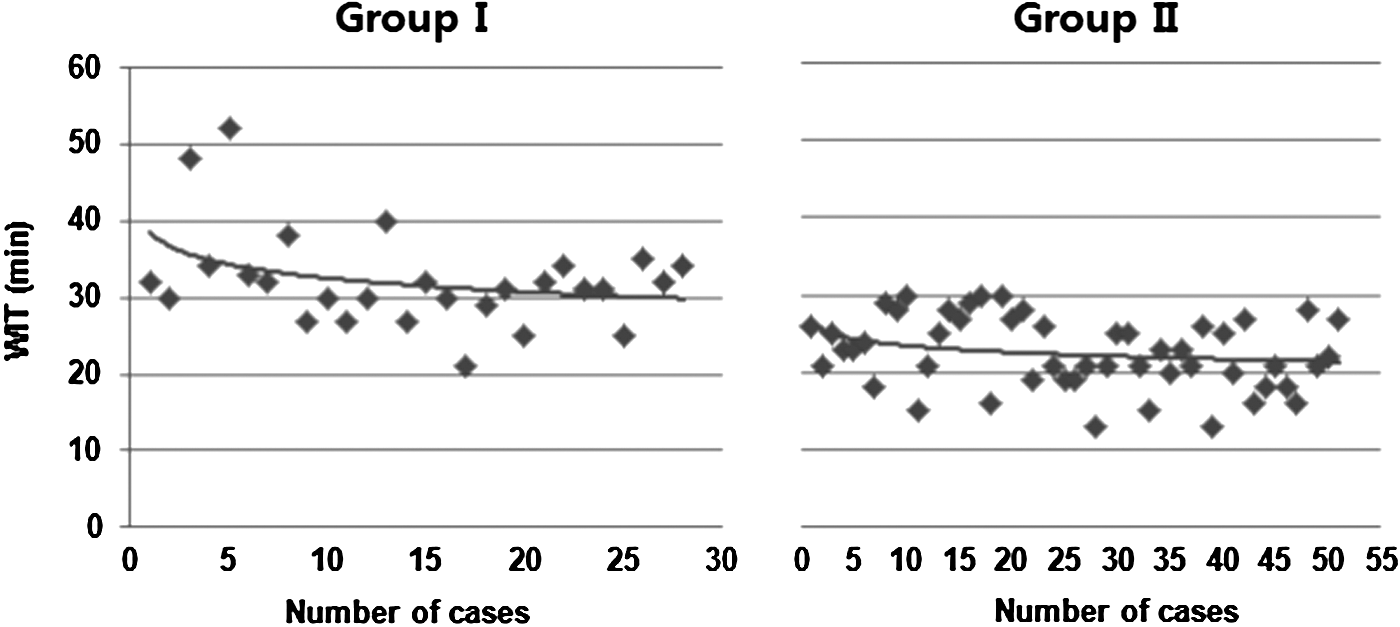
Graph of warm ischemia time (WIT) versus number of cases. The WIT of the initial 28 cases (Group I)
Both Group I and Group II had three complications (Table 2). Two cases of delayed bleeding in Group I and two pseudoaneurysms in Group II were resolved by angioembolization without additional complications.
The pathological data are shown in Table 3. The tumor sizes were 2.35±0.91 and 2.19±0.94 cm in Groups I and II, respectively (P=.509). Malignancy was revealed in 87% of the excised tumors. The most common pathological type of renal cell carcinoma was clear cell type (60/68, 88%). Other benign tumor types were angiomyolipoma, oncocyoma, leiomyoma, and complex renal cyst. Surgical margin was positive in 1 patient of Group I and 2 patients of Group II. However, all 3 patients did not show any recurrence evidence in the follow-up period.
AML, acute myleogenous leukemia; RCC, renal cell carcinoma.
Discussion
Laparoscopic radical nephrectomy has been a standard treatment method for the patient with localized renal cell carcinoma since reported in 1991 by Clayman et al. 6 Initial transperitoneal LPN was reported by Winfield et al., 7 and since then, the LPN appears as an alternative to laparoscopic radical nephrectomy in tumors smaller than 4 cm, with equivalent long-term oncological results in terms of recurrence and survival.8,9 Because of the success of the laparoscopic techniques, instruments have considerably developed, and more and more patients are operated on using LPN. Gill et al. 10 compared 1800 patients undergoing open partial nephrectomy and LPN by an experienced urologist, indicating that LPN has advantages of less operative time, decreased operative blood loss, and a shorter hospital stay, but disadvantages of longer WIT and more postoperative complications. For this reason, even for an experienced laparoscopic urologist, LPN is a difficult surgical technique because of the high level of difficulty related to intracorporeal suturing and knot-tying procedures. 11
Many types of innovative instruments have been designed to overcome the surgical difficulty of intracorporeal suturing and knot tying. Robot-assisted LPN appears to be a minimally invasive option that may offer shorter WIT and learning curve, showing favorable results for many perioperative parameters compared with LPN. 12 However, the robot-assisted LPN is limited because of a loss in tactile feedback resulting in tissue trauma or suture breakage, higher cost, and reliance upon the assistant to perform some of the more critical aspects of the case.13,14
A recent study reported that comparing running polyglactin suture and barbed suture using V-Loc™ (Covidien, Dublin, Ireland) for renorrhaphy during LPN reduced WIT to 7.4 minutes in the barbed suture group. 15 Erdem et al. 16 also reported that inner layer renorrhaphy time of 155 seconds and WIT time of 9 minutes were significantly reduced in the group treated by V-Loc in matched-pair analysis. The main drawback of the barbed suture is its expensiveness compared with the conventional polyglactin suture; if the wrong suture is performed, retrieval of the needle and the thread is difficult. Moreover, the time-consuming procedure of redoing the suture augments the operative time and WIT. We developed a running-clip renorrhaphy that is believed to be expeditious and simplified, as well as a reproducible technique for executing LPN to overcome the limitation of the robot-assisted LPN and barbed suture.
Our study demonstrated that the running-clip renorrhaphy could reduce the WIT in performing LPN. Although the exact limit of WIT beyond which irreversible renal injury occurs is controversial, the safe limit of WIT, the most critical portion of the LPN, is accepted to be within 30 minutes. Tumor excision and reconstruction of the remaining kidney must be completed within 30 minutes to preserve the function of the remaining kidney.17,18 In this study, WIT for all the cases using the running-clip renorrhaphy did not exceed 30 minutes.
The most remarkable change in the technique with running-clip renorrhaphy includes placing a continuous suture for the renal reconstruction and applying a Hem-o-lok clip to the threads sequentially for preserving the tension of the renal reconstruction. The running-clip renorrhaphy has some advantages compared with the conventional renorrhaphy. First, because running suture can be completed by inserting needle and thread at one time and a Hem-o-lok clip clip was applied sequentially after finishing the running suture, therefore, the WIT was minimized by obviating the extra steps for inserting and extracting the needle and thread and the laparoscopic instruments. Less WIT time allows more time to focus on delicate tumor resection and precise renal reconstruction. The mean WIT of sliding-clip renorrhaphy in the published series is in the range of 23.8–31 minutes for performing LPN.4,5 The mean WIT of our study was 21.5 minutes, and that is superior to the sliding-clip technique in LPN. Second, if the thread may be cut off for some reason, the tension pressure to maintain hemostasis decreases in performing a running suture. Hence, sequential locking Hem-o-lok clips prevent bleeding from loosening the thread tension. Third, laparoscopic tying is very difficult for a beginner laparoscopic urologist, and the no-tying suture technique is easy to follow and is replicable. Finally, the running-clip renorrhaphy can be easily performed at the institution not equipped with the robot-assisted system to reduce WIT, or it can be also applied in the setting of the robot-assisted LPN.
This study has several limitations. First, because of the retrospective nonrandomized study, a comparative analysis between a control group and randomization was impossible. However, for minimizing the effect of the learning curve by a surgeon, early series of the LPN were not included, and hundreds of cases of LPN, laparoscopic radical nephrectomy, laparoscopic radical prostatectomy, and laparoscopic pyeloplasty before initiating this study were performed by our surgeon (S.-H.H.). Second, because the Hem-o-lok clip is nonabsorbable, the long-term fate of the Hem-o-lok clip is unknown. One animal model study showed that Lapra-Ty has no evidence of migration, erosion, and similar inflammatory reaction compared with suture material. 19 We considered that the Hem-o-lok clip is also safe in the aspect of not increasing the complication of delayed bleeding, infection, and stone formation in Group II; however, long-term follow-up will be necessary to evaluate the effect and any complication by the Hem-o-lok clip in performing the running-clip renorrhaphy.
Conclusions
The use of the running-clip renorrhaphy for performing LPN is a safe and an efficient technique, offering significant reduction in operative time, WIT, and IBL compared with the interrupted knot-tying suture renorrhaphy. Moreover, the running-clip renorrhaphy may be easily adapted by a beginner laparoscopic urologist and is an easily reproducible operative technique.
Footnotes
Disclosure Statement
No competing financial interests exist.