
Abstract
Abstract
Introduction:
One of the latest methods for management of pancreaticogastrostomy (PG) leakage after pancreaticoduodenectomy (PD) is endoscopic vacuum therapy.
Subjects and Methods:
PD was performed on a 72-year-old man suffering from a nonfunctioning pancreatic neuroendocrine tumor of the head of the pancreas. On postoperative Day 6 after the primary surgery, postoperative pancreatic fistula (POPF) of the PG was revealed. Based on the International Study Group of Pancreatic Fistula recommendations, total parenteral nutrition, a regimen of somatostatin analogs, and intravenous antibiotics were implemented. The patient was qualified for a re-exploration because of the doubtful safety of percutaneous drainage of fluid collection detected in the ultrasonography scan. However, this management was not efficient. Endoscopic vacuum treatment (E-VAC) was initiated. The E-VAC was placed directly into the POPF site using a modified “percutaneous endoscopic gastrostomy (PEG)-like” technique.
Results:
Over the next few days, the E-VAC was started. The volume of fluid collection from percutaneous drainage rapidly decreased, whereas the volume of E-VAC the following day after vacuum therapy was approximately 1000 mL. There were no signs of leakage of PG confirmed with endoscopy, and there was no fluid collection from peripancreatic drainage. The E-VAC therapy was stopped after 6 days. The patient's general condition improved significantly. There were no abnormalities observable in both clinical and imaging examinations.
Conclusions:
In selected patients, the “PEG-like” modification can be used successfully in the management of POPF. This technique allows the E-VAC to be placed directly in the POPF site under the endoscopic camera, which is what makes this method safe and efficient.
Introduction
D
From all anastomoses performed during PD procedures, the pancreatic fistula concerning the pancreaticojejunostomy or pancreaticogastrostomy (PG) is the most common and reaches up to 20%. 2
Based on the International Study Group of Pancreatic Fistula classification for Grade C fistulas, total parenteral or enteral nutrition, a regimen of somatostatin analogs, and intravenous antibiotics are recommended. 1 Indications for re-exploration in patients with postoperative pancreatic fistula (POPF) are strictly defined. However, for patients characterized with multiple organ dysfunctions and, generally, a severely unstable condition, there is a need to search for other promising interventions.
Recently some minimally invasive procedures have been proposed for the purpose of enhancing the standard management of gastrointestinal fistulas. Fibrin glue for endoscopic treatment of upper gastrointestinal tract fistulas or coagulation factor XIII for pancreatic and duodenal fistulas was used.3,4 Although the preliminary reports are promising, these techniques seem to be suitable for a selected group of patients. Therefore it is highly desirable to discover new methods to improve treatment of gastrointestinal anastomotic leakages. The optimal method should be characterized by simplicity, high success rate, safety, and cost-efficiency. We present the case of a patient with POPF successfully treated with the use of endoscopic vacuum treatment (E-VAC) applied in a “percutaneous endoscopic gastrostomy (PEG)-like” manner after PD.
Based on the International Study Group of Pancreatic Fistula recommendations for POPF, Grade C was implemented. Because of the ineffective drainage of POPF contents and unsafe possibility for percutaneous drainage, re-exploration was performed. Subsequently, deterioration of the patient's general condition was observed with evidence of multiorgan dysfunctions. Because there was no improvement, the patient was qualified for E-VAC therapy.
Materials and Methods
A 72-year-old man was qualified for surgery because of a nonfunctioning pancreatic neuroendocrine tumor at the head of the pancreas at approximately 11.5 cm based on the ultrasonography scan. According to the abdominal computed tomography scan, a large pancreatic tumor measuring 14×11×10 cm was revealed. The enhancement due to the computed tomography scan was weak and nonequally distributed, with features of central necrosis and calcifications. There was no evidence of infiltration of adjacent organs. Both bile ducts as well as the pancreatic duct were not dilated. The patient did not present any signs of jaundice.
Intraoperatively, the tumor at the head of the pancreas was found. It was a fully encapsulated, movable tumor with a rich pathological vasculature within the capsule, without any evidence of invasion into adjacent organs. No lymphadenopathy was found. Intraoperatively, the specimen of the tumor was taken for histopathologicical examination, which confirmed the neuroendocrine nature of the tumor. The final histopathological examination revealed a neuroendocrine carcinoma, NEC grade G3 (with a mitotic count of >20 per 10 high-power fields and >20% Ki67 index). Immunostaining with chromogranin A and synaptophysin confirmed the neuroendocrine carcinoma.
PG following PD was performed (Fig. 1). The duodenum was mobilized (the Kocher maneuver). Following the dissection of the superior mesenteric vessels as well as the portal vein, the pancreas was cut using cautery. The proximal pancreatic remnant was mobilized. The entire duodenum and pancreas were dissected and resected en bloc. The gallbladder was resected as well. Because of our institute's surgeon preferences as well as the anatomy aspects in this particular case, the PG anastomosis following PD was performed. End-to-side hepaticojejunostomy and end-to-end gastrojejunostomy were performed on the same jejunal limb. Gastrojejunostomy was performed with a running PDS (polydioxanone) suture, whereas for the hepaticojejunostomy an interrupted monofilament suture was used. For a pancreatic remnant reconstruction, the PG was performed with single-layer 3-0 silk sutures. The first layer was placed from the posterosuperior wall of the stomach to the posterior wall of the pancreas. Then the gastrostomy (4 cm) was performed, and the layer of the anterior wall of the pancreas was placed to complete the PG.
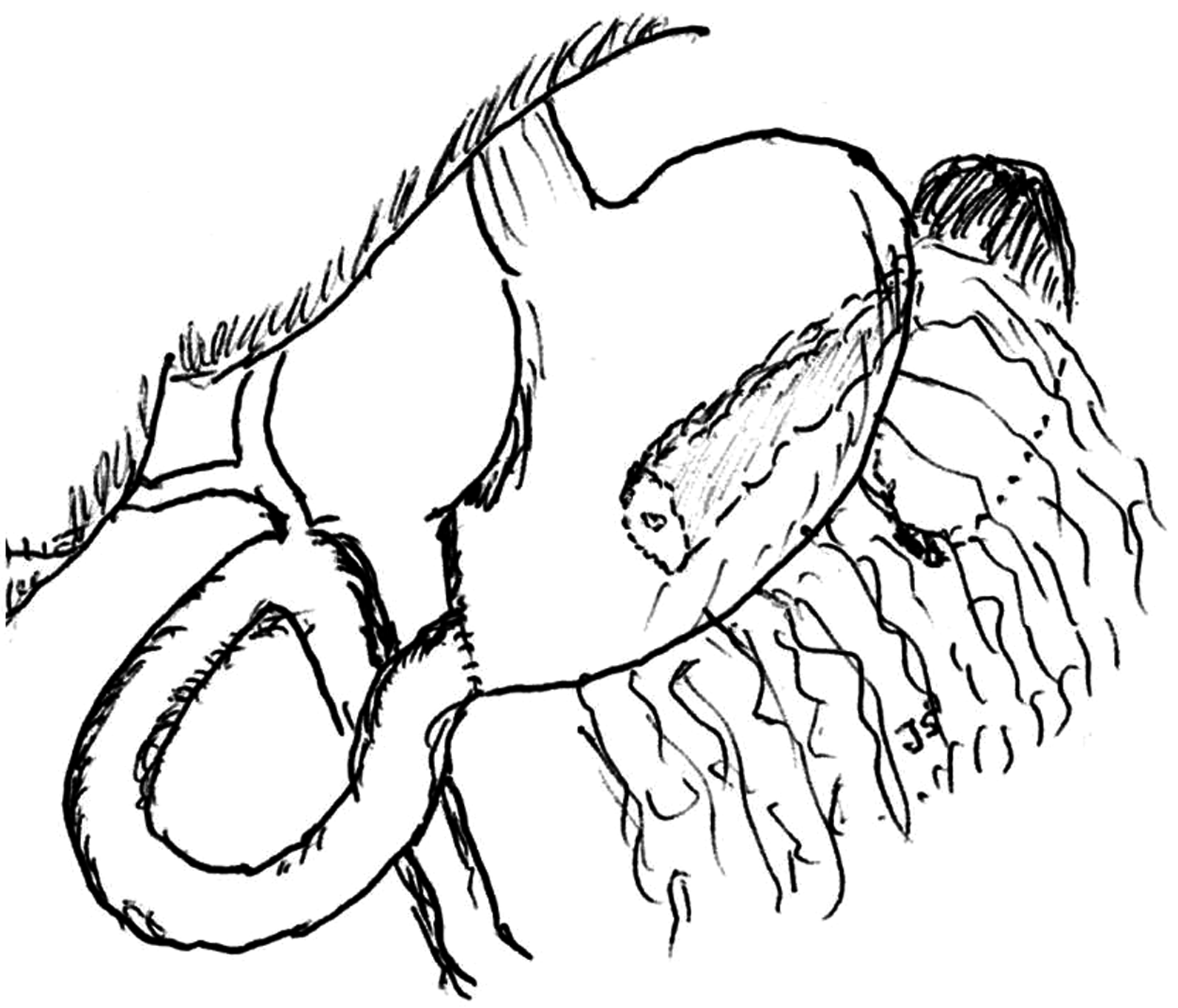
Schematic diagram of the pancreaticoduodenectomy.
On postoperative Day 6, POPF was confirmed by the elevated level of amylase in the fluid collected from peripancreatic drainage (108,000 U/L). The patient was re-operated on twice, on postoperative Days 7 and 12. Because of the first re-surgery, the leakage of the posterior wall of the PG was revealed. POPF of the PG was assessed approximately in one-third of the posterior wall of the anastomosis. The PG was revised, and two drains were placed in the peripancreatic region. Total parenteral nutrition and somatostatin management were implemented. According to the second re-operation, the appropriate PG dehiscence was impossible to evaluate owing to massive intraabdominal adhesions. In endoscopy, before the negative pressure wound therapy implementation, the dehiscence of PG was approximately of 50% of the posterior wall of PG.
The patient's condition deteriorated, with signs of multiorgan dysfunctions. Additionally, an increased fluid collection from peripancreatic drainage was observed. On postoperative Day 20, the patient was qualified for E-VAC.
Gastroscopy was performed with the patient under sedation using propofol and midazolam. The POPF of PG anastomosis was easily identified. At the bottom of the POPF, one of the abdominal drains was visualized as being deeply embedded in the POPF site. A monofilament suture (3-0) was attached to the outer end of drain number 1 (located outside the abdominal cavity). Using the endoscopic grasper, the drain with the attached monofilament suture was passed from the outside of the abdomen and pulled out through the mouth together with the endoscope (Fig. 2). The monofilament suture was thus localized, outside the abdominal wall from one side, while the other end was pulled out through the oral cavity. Then the polyurethane sponge (the so-called “black sponge”) was cut to the appropriate size to fill the POPF and attached to the end of the monofilament suture passing through the mouth (Fig. 3). The E-VAC was pulled down into the stomach through the mouth and esophagus and placed in the POPF. The final position of the E-VAC was established using both endoscopic grasper manipulation and the outer end of the monofilament suture pulled outside the abdominal cavity (Fig. 4). The sponge completely filled the POPF and the PG anastomosis (Fig. 5).
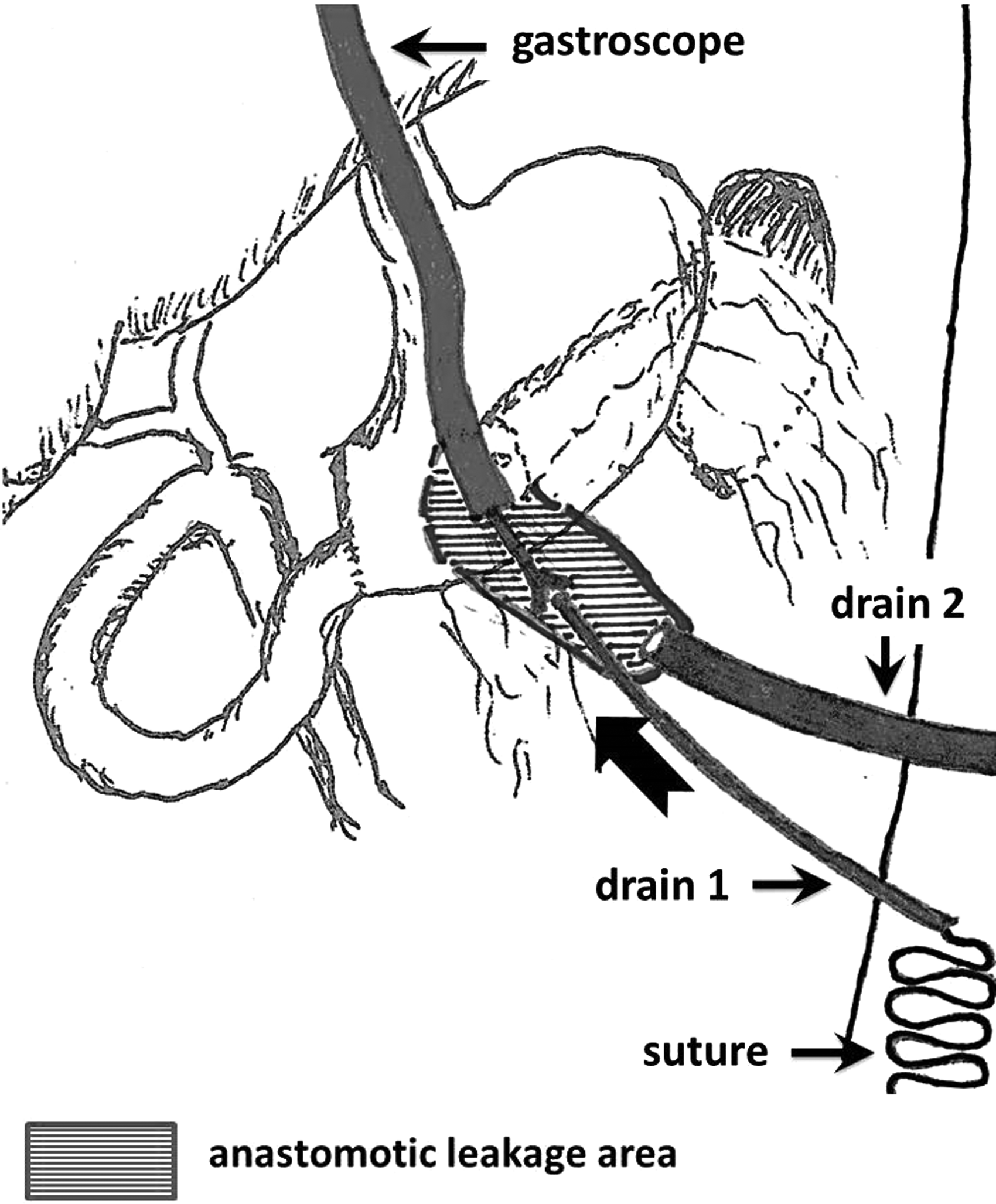
The postoperative pancreatic fistula (marked with hatched lines) drained with drains number 1 and number 2. The endoscope was introduced into the stomach, and using an endoscopic grasper, the drain with the attached monofilament suture (drain number 1) was passed from the outside of the abdomen and pulled out through the mouth.
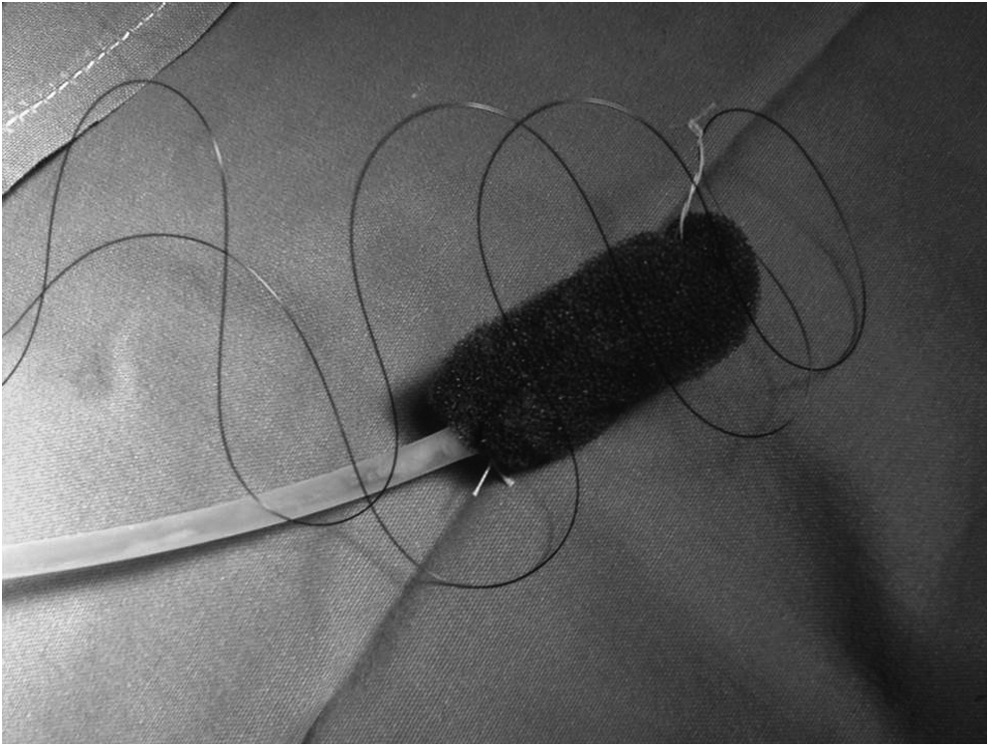
The polyurethane sponge attached to the nasogastric tube (the endoscopic vacuum treatment device).
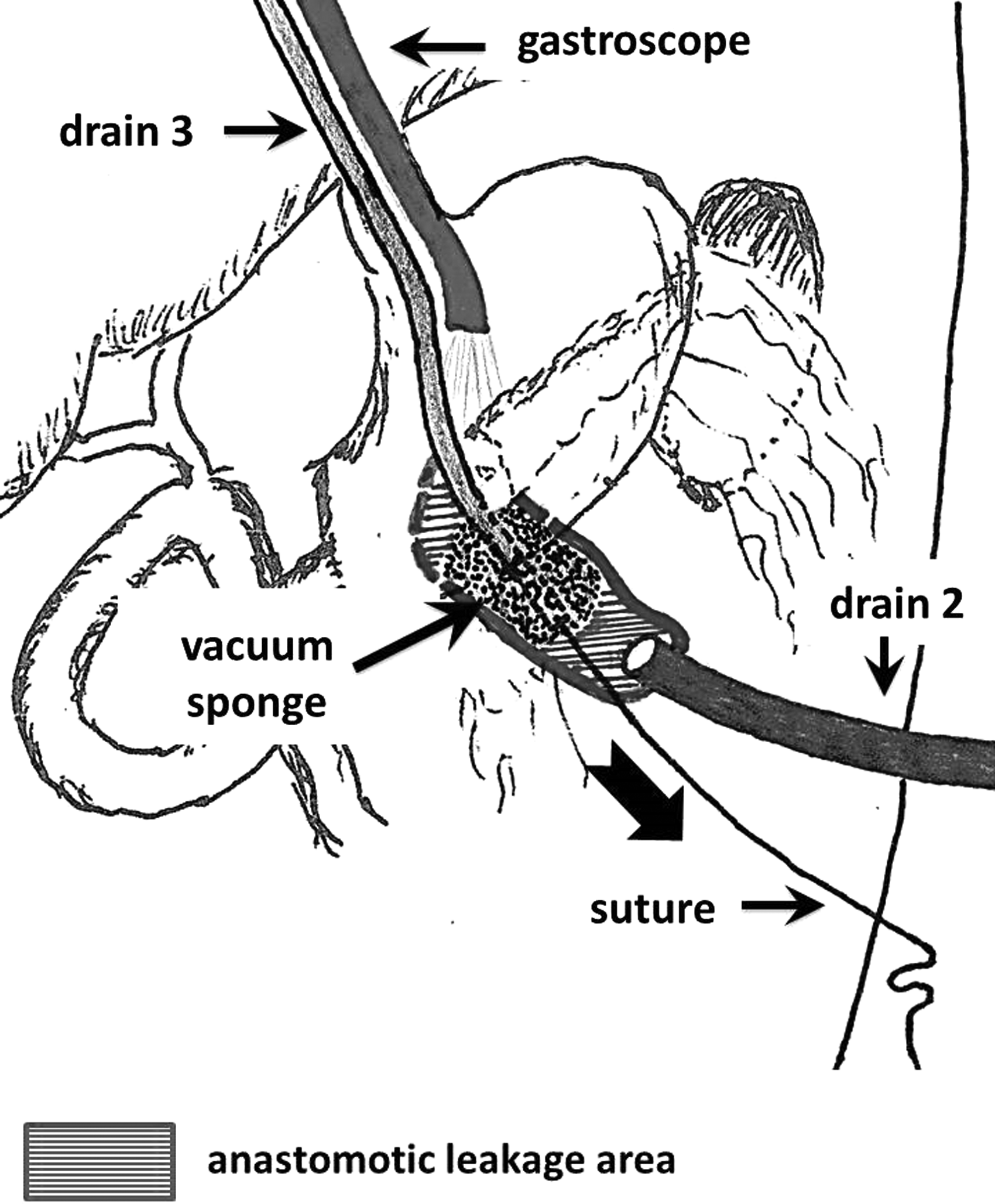
The endoscopic vacuum treatment device placement into the postoperative pancreatic fistula site was established using both endoscopic grasper manipulation and the outer end of the monofilament suture (outside the abdominal cavity).
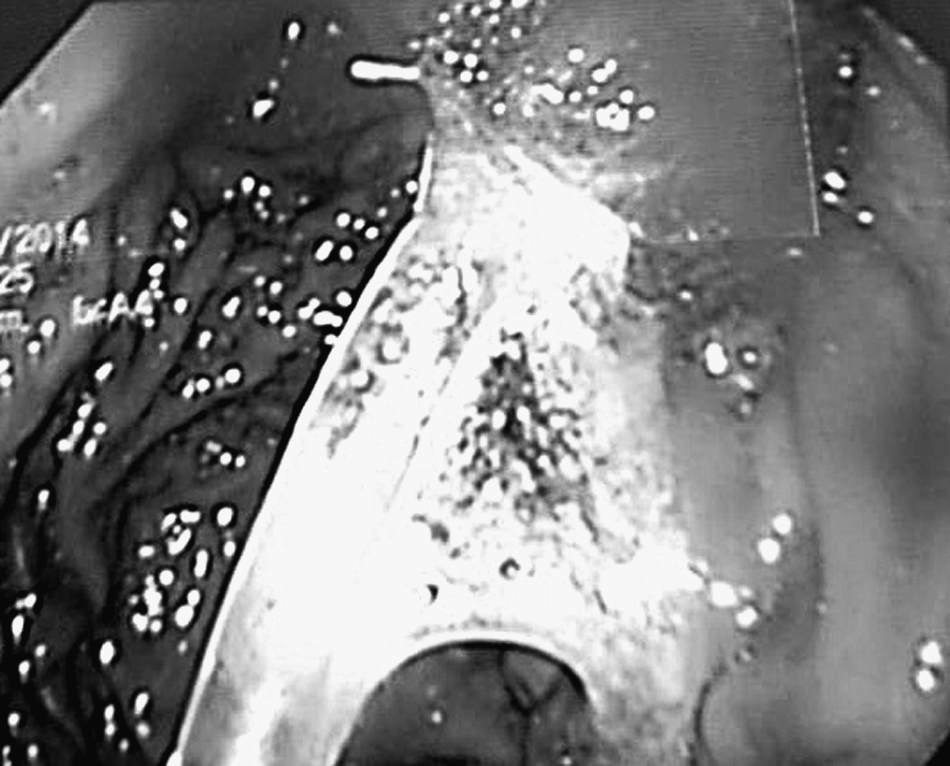
Endoscopic view of the endoscopic vacuum treatment device placement in the postoperative pancreatic fistula site.
Results
The entire time of the procedure was 17 minutes. It was well accepted by the patient, and no complications occurred either peri- or postoperatively. Immediately after the E-VAC was placed, negative pressure therapy was initialized with a Renasys™ device (Smith & Nephew, Hull, United Kingdom). Continuous negative pressure was set up with a pressure of −100 mm Hg.
On the second day of the E-VAC therapy, a decreased volume of peripancreatic fluid collection from percutaneous drainage was observed. The volume of exudate of the E-VAC was approximately 1000 mL, since the first day of the vacuum therapy. The volume of the drainage contents is summarized in Table 1.
Before vacuum drain introduction.
The general condition of the patient improved, which was confirmed by the patient's biochemical parameters (Fig. 6). According to the ultrasonography scan, there were no abscesses or fluid collection in the abdominal cavity. The patient began rehabilitation, and very quickly he was able to be mobilized with the mobile vacuum device. To avoid ingrowing of the polyurethane sponge with granulated tissue at the site of the POPF, the position of the E-VAC was slightly moved every 2 days. On Day 6 after the introduction of the E-VAC therapy, a check-up endoscopy was performed. The POPF was found to be significantly decreased in size with no further indication for the E-VAC therapy.
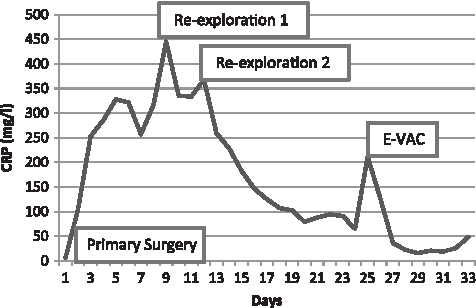
C-reactive protein (CRP) level.
After the E-VAC therapy was stopped, slightly increased fluid collections from percutaneous drainage (drain 2) were observed within the next 4 days (ranging from 50 to 70 mL/day). In the next few days, the fluid contents were normalized to approximately 10–20 mL/day. At 21 days after the beginning of negative pressure therapy, only a marginal volume was observed at the place where the drain was removed (secured with an ostomy bag). The patient was discharged from the hospital in good general condition.
Discussion
Endoscopic management for the gastrointestinal tract is still under development. Negative pressure wound therapy is considered to be a reasonably successful method for the management of surgical complications, including anastomotic leakage. Negative pressure wound therapy is a well-known method for the treatment of complicated wounds. The necessity for application of negative pressure wound therapy has become more prevalent in recent years for fistulas and anastomotic leakages. 5 In the case of lower gastrointestinal tract fistulas following anastomosis insufficiency, mostly after anterior resection of the rectum, endoscopic vacuum therapy is used with high effectiveness and a low rate of complications.6,7 Endoluminal vacuum therapy based on the B. Braun (Melsungen, Germany) Endo-Sponge® system seems to be an effective and helpful method for the treatment of anastomotic leakage in this group of patients. 8 According to the latest studies, data concerning endoscopic vacuum therapy for esophageal fistulas are promising. 9 Endoscopic vacuum-assisted therapy is well tolerated by patients and is an effective therapeutic option for the treatment of esophageal leakage after surgery. Brangewitz et al. 10 found the E-VAC as a more effective method than a stent placement. The E-VAC method still requires some improvements. Currently, the management is based on the existing standard wound dressing sets in a combination with a polyurethane sponge and a nasogastric tube. However, some new devices, designed more specifically for endoscopic negative pressure wound therapy, such as an endoscopic sponge application tool, have already been described by Senderak and Banasiewicz. 11
Data concerning endoscopic vacuum therapy for upper gastrointestinal tract fistulas are limited.9,10 So far, only one case report has been described regarding PG leakage successfully treated with endoscopic vacuum therapy. 12
In the results presented here, endoscopic vacuum therapy for POPF management was impressive. The fluid collection of POPF decreased rapidly following the implantation of the E-VAC. The general condition of the patient improved significantly. High tolerance for the E-VAC therapy by the patient was reported, and there were no side effects or complications.
We used negative pressure therapy for POPF of PG anastomosis insufficiency in a modified manner.
Because all the steps of placing the E-VAC in the POPF are very similar to the PEG procedure, we adopted the name for the purpose of describing the procedure in a more understandable manner. In our opinion that kind of procedure is exactly the same as for PEG. Both introduction of the E-VAC through the mouth and esophagus (similar to the PEG procedure) and support with the guidance of the monofilament suture from outside through the stomach (comparable to the wire in the PEG procedure) under the endoscopic camera are almost the same as in the PEG procedure. The main benefit of this modification is the safety of the E-VAC application as well as the reassurance that the E-VAC was located in the POPF site using both endoscopic camera guidance and the monofilament suture from outside the abdominal cavity. Changes of the E-VAC position (a delicate movement), made every 2–3 days, protect the polyurethane sponge of the E-VAC from overgrowing with granulated tissue. That prevented potential bleeding while the E-VAC is changed. The guidance of the monofilament suture allows the E-VAC to be changed in a simple and safe way.
The question whether the E-VAC itself affects the healing process at the POPF site is still unresolved. From the practical point of view it is important to adjust the appropriate size of the polyurethane sponge to the size of the POPF. In our opinion, proper adjustment of the E-VAC size to the POPF should not have an influence on increasing PG dehiscence. Moreover, every change of the E-VAC should be adapted to the current size of the POPF, which usually means using a polyurethane sponge smaller and smaller in size.
There are some limitations of this therapy. First, the chance of visualization of the abdominal drain at the POPF site during endoscopy is limited by the small number of cases. Second, although the outside part of the abdominal drain and the monofilament suture were disinfected prior to their passage inside, there is a potential possibility of bacterial transmission into the peritoneal cavity. One of the potential problems of using vacuum-assisted therapy for fistula management is the increased volume of the output. This problem is particularly important in a case of using vacuum-assisted therapy for open abdomen management complicated with enterocutaneous fistulas. 13 It is important to note that when using the E-VAC, the fluid collection of the POPF is sucked directly toward the gastrointestinal lumen and then outside via the nasogastric tube. There are no data based on clinical studies regarding this problem. However, it does not seem that E-VAC therapy increases either pancreatic or gastric secretion. It is also important to use the appropriate negative pressure. There are no precise literature data regarding this issue because of the small number of patients who have been treated with the E-VAC therapy. Based on our experience, pressure ranging between −80 to −120 mm Hg is sufficient for the purpose of effective treatment without any side effects of the therapy. In our opinion the appropriate settings of negative pressure should be adjusted to the POPF size and the density of secretions, as well as the daily volume of the E-VAC fluid collection.
In our opinion E-VAC therapy for upper gastrointestinal tract anastomotic leakage is a safe and simple method, fully accepted by the patient. One of its limitations is the lack of a specially designed device for the purpose of that particular management. In selected patients the “PEG-like” modification can be used. That technique allows the E-VAC to be introduced directly at the POPF site in a safe and efficient manner.
Footnotes
Acknowledgments
The authors thank Stanisław Malinger, MD, PhD, and Józef Świrkowicz MD, PhD, for their assistance in the preparation of the manuscript.
Disclosure Statement
No competing financial interests exist.