
Abstract
Abstract
Background:
Appendicular stump closure is a crucial step during laparoscopic appendectomy. Recently, endoclips (ECs) have been described for ligation of the appendicular stump. The objective of this review was to compare outcomes with EC versus endoligature (EL) for appendiceal stump closure during laparoscopic appendectomy.
Materials and Methods:
A literature search of Medline, Embase, Cochrane Database, and Google Scholar was performed to identify studies comparing use of EL versus EC in laparoscopic appendectomy between January 1992 and September 2013. Reviews of each study were conducted, and data were extracted. The random-effects model was used to combine data, and between-study heterogeneity was assessed.
Results:
Seven of the 101 identified studies met the inclusion criteria: four randomized controlled trials and three case controlled series. For the primary outcome of perioperative and postoperative complications, there was no significant difference between the EC versus EL groups. No differences were noted in length of hospital stay. However, a significant reduction in operative time was observed with EC as opposed to EL (standardized mean difference=–0.90, 95% confidence interval=−1.26 to −0.54, P=.001). Moreover, EC procedures were less expensive than EL procedures.
Conclusions:
EC application in the management of appendiceal stump during laparoscopic appendectomy appears to be simple, efficacious, safe, and a cost-effective alternative.
Introduction
A
Laparoscopic technique has been shown to markedly reduce postoperative pain and incidence of wound infection, shorten the hospital stay, and facilitate faster postoperative recovery. 4 However, a significant downside of laparoscopic appendectomy, besides a longer procedure time and higher operative cost, is a marginally higher intraabdominal abscess rate. 1 All these factors have been implicated as being influenced by the technique of stump closure. Moreover, although laparoscopic appendectomy is becoming the treatment of choice, provided expertise is available, much ambiguity still persists regarding appendiceal stump closure and the optimum closure device. This is further illustrated by the range of techniques and closure devices currently available for this purpose, such as endoligatures (ELs) (including preformed suture loops [endo-loops] and intracorporeal knot-tying sutures), bipolar coagulation, endoscopic linear cutting staplers (Endo GIA™; Covidien, Mansfield, MA), the LigaSure™ system (Covidien), and the Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH). Although literature suggests that the stapling is the safest closure method of the appendicular stump, it is also the most expensive.
Recently, endoclips (ECs), both metal and polymer, have been described for ligation of the appendicular stump. Several studies have now compared the outcomes of ECs with those of ELs for appendicular stump closure in laparoscopic appendectomy. We performed a systematic review of all studies comparing ECs with ELs in the laparoscopic management of acute appendicitis. Our primary aim was to assess the difference in perioperative and postoperative outcomes of laparoscopic appendectomy between the two appendicular stump closure techniques.
Materials and Methods
Identification of studies
The electronic bibliographic databases Medline, Embase, Cochrane Database, and Google Scholar were searched from January 1992 to September 2013 for all studies, comparing use of EL versus EC in laparoscopic appendectomy. The following terms were used in the search algorithm: laparoscopic appendectomy OR appendicular stump closure AND endo-clips OR endo-loops OR knot tying sutures. Identification of studies and subsequent data extraction were performed independently by two researchers (R.B. and F.M.S.), and conflicts were solved by consensus.
Eligibility criteria
Only studies in English literature that compared EL and EC for laparoscopic appendectomy in all patients regardless of age and country were eligible for inclusion. The primary end points of this meta-analysis were the rate of perioperative and postoperative complications following the use of EL and EC. The secondary end points examined were total operative time, length of postoperative hospital stay, and cost.
Data extraction and outcomes
The following information regarding each eligible study was recorded: authors' names, journal, publication year, and study design. The following data were recorded for both arms of each eligible study: the number of patients assigned to each appendix stump closure technique, number analyzed per arm, mean age, perioperative complications, conversion rate, total operative time, postoperative complications, total hospital stay, and cost.
Statistical analysis
Data from eligible studies were entered into a computerized spreadsheet for analysis. Statistical analysis was done using the Comprehensive Meta-Analysis software (version 2.2.034; Biostat, Englewood, NJ). All pooled outcome measures were determined using a random-effects model as described by DerSimonian and Laird. 5 The odds ratio (OR) was estimated with its variance and 95% confidence interval (CI). The random-effects analysis weighted the natural logarithm of each study's OR by the inverse of its variance plus an estimate of the between-study variance in the presence of between-study heterogeneity.
For continuous data (e.g., total operative time, total hospital stay), we used the Hedges g statistic to calculate standardized mean differences (SMDs). We summarized binary data (e.g., complications, recurrence) as risk ratios. When standard deviations (SDs) were not reported in the studies, we estimated SDs from either means or P values. 6 Heterogeneity between different studies was assessed by use of the I2 inconsistency test and chi-squared-based Cochran's Q statistic 7 test in which P<.05 is taken to indicate the presence of significant heterogeneity. Subgroup and sensitivity analyses were not feasible owing to the limited number of studies included in our review. Publication bias was also difficult to assess for the same reason.
Quality assessment
The quality of the included studies for randomized clinical trials was assessed by using the scoring system of Jadad et al. 8 and for nonrandomized studies by the Newcastle–Ottawa scale. 9
Results
Description of eligible studies
The literature search revealed seven published articles that directly compared EL and EC appendiceal stump closure techniques.10–16 No reference was identified through scanning the reference lists of the identified studies. Table 1 shows the patients' demographics and the characteristics of the included studies. All studies were restricted to emergency laparoscopic appendectomy for acute appendicitis. Most of the characteristics were not significantly different between treatment groups. All except one study were performed on an adult patient population. Figure 1 depicts a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram, detailing the literature search. 17 Of note is that four studies were randomized. Only two studies specified their randomization method; Colak et al. 12 used a computer-generated randomization schedule, whereas Gonenc et al. 15 used a lottery method. Ates et al. 11 assigned an uninvolved officer for consecutively randomizing patients; however, they did not explain the randomization method. Patient groups were clearly described in all studies, and all were accounted for results.

PRISMA flow diagram.
EC, endoclip; EL, endoligature; NA, not applicabl; NI, not indicated; NOS, Newcastle–Ottawa scale.
The total number of patients assigned to treatment in the seven studies was 517. After excluding the dropouts, the total number examined was 487 patients. Of these, 245 (50.3%) underwent EL and 242 (49.7%) underwent EC stump closure. All patients were enrolled between 2006 and 2011. For stump closure in the EC group, five studies used polymer clips, and the remaining two used titanium clips. In the EL group, five used endo-loops, and two studies used intracorporeal knot-tying sutures.
Primary outcomes
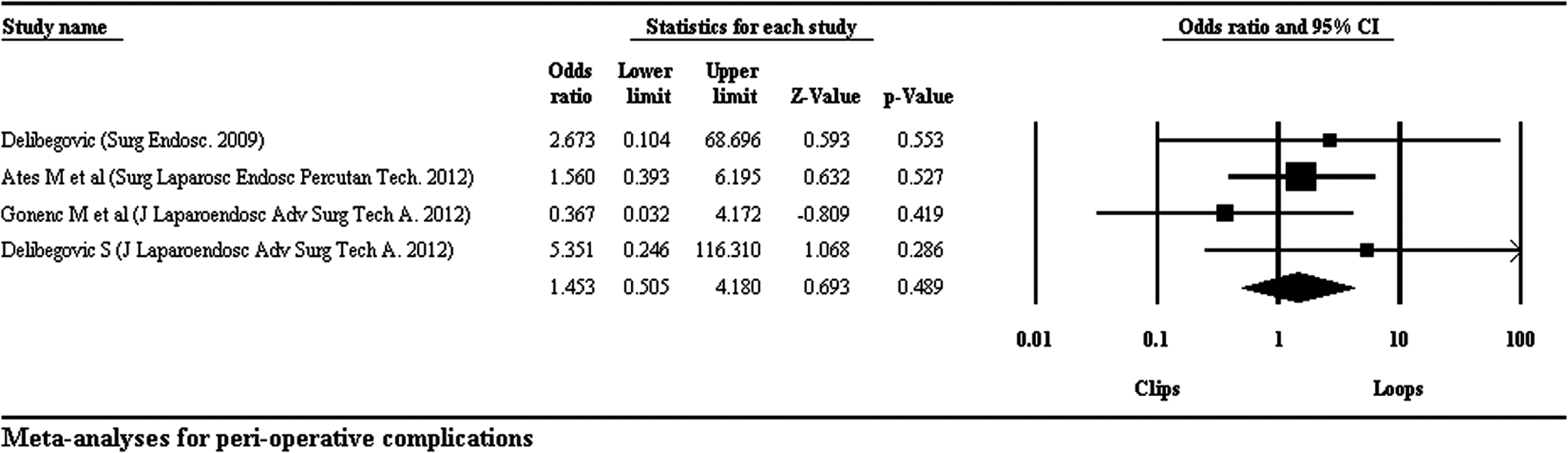
Perioperative complications
Four studies recorded perioperative complications. Results of meta-analysis demonstrated a nonsignificant difference between perioperative complication rates (OR=1.45, 95% CI=0.51–4.18, P=.49) (Fig. 2). There was no evidence of statistical heterogeneity (Q=2.06; P=.55, I2=0%).
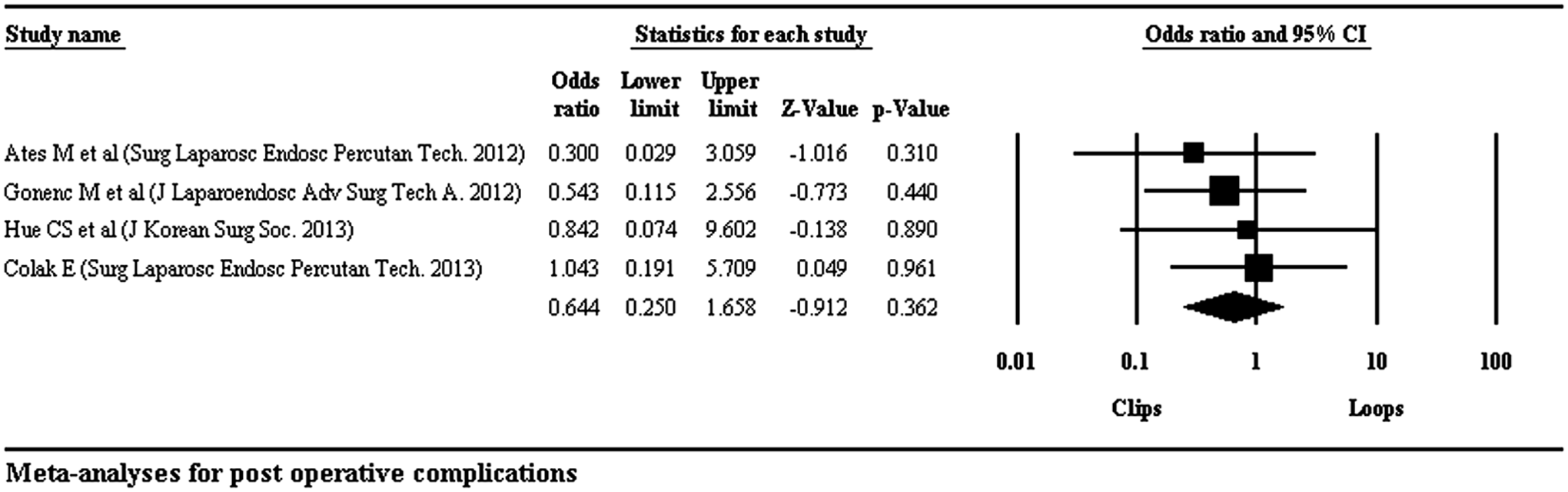
Postoperative complications
Postoperative complications were described in four studies. Subsequent meta-analysis calculated a nonsignificant difference between postoperative complication rates (OR=0.64, 95% CI=0.25–1.66, P=.36) (Fig. 3). There was no evidence of statistical heterogeneity (Q=0.82; P=0.85, I2=0%).
Secondary outcomes
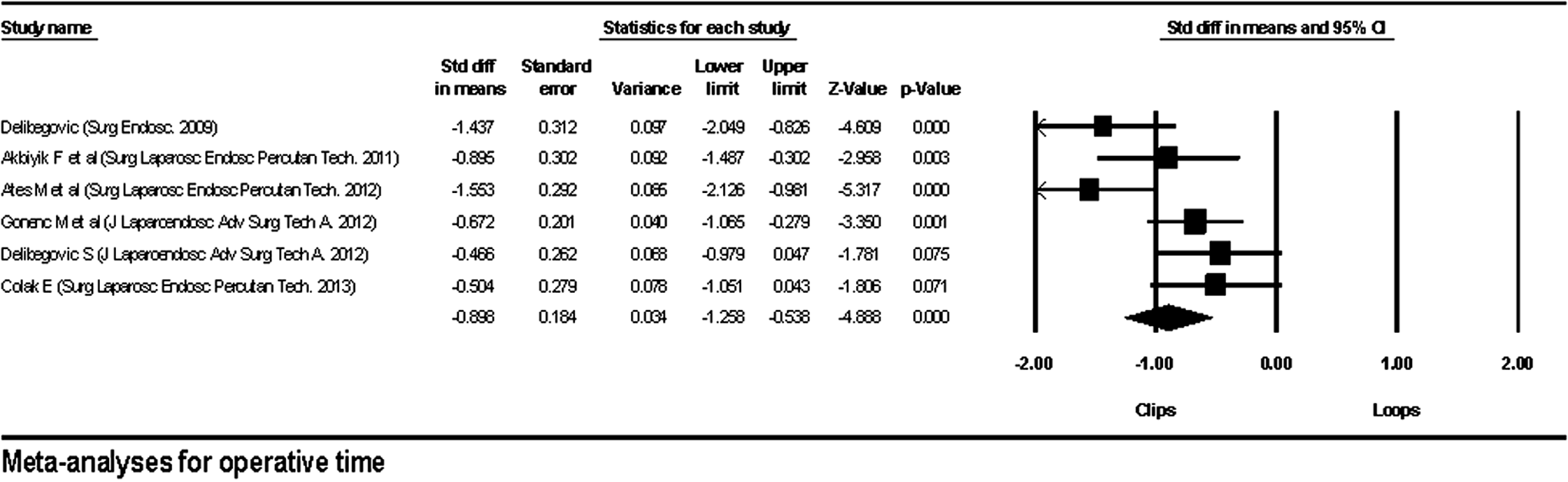
Operative time
Operative times were compared in six studies. There was a significant reduction in operative time when ECs were used as opposed to ELs (SMD=−0.90, 95% CI=−1.26 to −0.54, P=.001) (Fig. 4). There was evidence of statistical heterogeneity (Q=13.84; P=.02, I2=63.87%).
Length of stay
All seven studies examined length of stay and did not identify a significant difference between the two appendicular stump closure techniques (SMD=−0.040, 95% CI=−0.22 to 0.14, P=.660) (Fig. 5). There was no evidence of statistical heterogeneity (Q=0.806; P=.99, I2=0%).

Cost-effectiveness
Six studies compared the cost of ECs versus EL. However, it was not possible to perform cost analyses because of lack of data, specifically mean and SD among studies. Table 2 describes the individual cost of each procedure detailed in each study. For comparative convenience we converted all currencies to Euros. EC usage was comparatively lower priced than EL usage.
Original currencies were converted to Euros using the Google Currency Converter. 18 Using a a two-sample t test, P=.007 between EL and EC costs.
EC, endoclip; EL, endoligature; NI, not indicated.
Discussion
Appendicular stump closure is a crucial step during laparoscopic appendectomy, and an inappropriate management can lead to catastrophic complications. Different techniques have been described to secure the appendix base, yet the two most frequently used methods are endo-loops and endostapling.19,20
Mechanical staplers have the advantage of easy handling, tight closure, and prevention of protruding mucosa and hence less chance of intraabdominal abscess formation. Conversely, staplers are expensive and have been implicated in causing small bowel obstruction, limiting their routine use. 21 Closure involving endo-loops, although economical, 22 is associated with marginally higher rates of abscess formation, because of insufficient stump closure and exposure of noninvaginating, contaminated mucosa to the abdominal cavity.23,24
EC usage in laparoscopic appendectomy was first described by Christalli et al. 24 in 1991. Advantages of the EC lie in its ease and simplicity of application, shortening of operative time, and negligible cost. Recently, several experiences of EC application for securing the appendiceal stump in laparoscopic appendectomy have been published, leading to the prospective trials analyzed in our review.
Our study, investigating seven trials, represents a summation of the available evidence to date and is the first of its kind. This review has shown that EC usage is effective in appendiceal stump closure and that its safety is similar to that of EL usage, as there was no difference in peri- or postoperative outcome among the two groups. This is also reflected in term of results of meta-analysis of hospital stay, with no difference on the length of hospital stay among the two groups, suggesting EC usage does not prolong hospital stay.
When compared with open appendectomy, the overall operating theater and equipment costs incurred during laparoscopic appendectomy are higher.25,26 This has slowed down the adoption of laparoscopic appendectomy in many hospitals. In this era of cost containment and healthcare crisis, physicians have been posed significant challenges in minimizing procedural and treatment expenditures. Furthermore, in developing countries, with already scarce health budgets, any measure of minimizing cost is worth considering. This is relevant from meta-analysis, as most studies were from developing countries. This analysis shows that the equipment cost in laparoscopic appendectomy can be reduced, if ECs are used routinely for the management of the appendicular stump. ECs are generally used to ligate the mesoappendix, and in most cases only three or four clips are used from the cartridge, mostly containing 8–10. Managing the appendicular stump with ECs instead of ELs saves the additional cost of ELs. Although it was not possible to perform meta-analysis on cost (because of lack of data), however, we compared the cost between the two groups mentioned in different studies. It is clear that the cost is significantly lower in the EC group.
Laparoscopic appendectomy provides a valuable training opportunity to surgical trainees to master their basic laparoscopic skills.27,28 Unfortunately, this is at the expense of further increase in operative time. Likewise, operative time is correlated with the level of resident seniority and function in the surgical team.29,30 Application of ECs in laparoscopic appendectomy can not only save the operating theater time and cost, it can also make the procedure technically less demanding, especially for junior surgical trainees.
Strengths of the relevant studies and subsequent analysis included their prospective nature and being from different countries around the globe. However, in analyzing the present review, the reader is advised to consider several limitations that may influence the results. First, there has been no major multicenter, randomized controlled trial performed on this subject. The included studies are all single centered. Although four studies were randomized, their design was weak, and poor randomization techniques were used. The second major limitation was inconsistency in exclusion criteria and its contribution to individual study and overall channeling bias. Ates et al. 11 excluded patients with appendiceal mass and perforation. Gonenc et al. 15 excluded patients with septic shock, severe systemic disease, or complicated appendicitis. Patients with a large appendicular base were excluded by Hue et al. 16 Intention-to-treat analysis was not completed in any study for patients excluded for any reason. Third, for stump closure in the EC groups, two types of clips were used—polymer and titanium—whereas in the EL group, both endo-loops and intracorporeal knot-tying sutures were applied to close the appendicular stump. We think, because endo-loops and intracorporeal knot-tying sutures are both well-studied and well-established techniques in appendicular stump closure, these can be used as controls. With regard to technical application of clips, most studies applied two extra-large clips (external length of 13 mm) at the base of the appendix in order secure the appendicular stump and one additional clip distally. Only studies using titanium clips used regular-sized clips. All these limitations should be addressed in future studies.
In conclusion, EC application in management of the appendiceal stump during laparoscopic appendectomy appears to be simple, efficacious, safe, and a cost-effective alternative. Nevertheless, further multicenter, prospective studies with appropriate randomization and design with all grades of appendicitis are required before EC application for securing the base of the appendix in laparoscopic appendectomy can confidently be recommended as the standard practice.
Footnotes
Disclosure Statement
No competing financial interests exist.