
Abstract
Abstract
Purpose:
To report a laparoscopic approach for pediatric inguinal hernia repair using a hybrid single-incision laparoscopic (H-SIL) technique and its clinical outcomes.
Materials and Methods:
A retrospective study was carried out in inguinal hernia cases treated with the new H-SIL approach using intracorporeal jumping purse-string sutures. The operative time, length of postoperative hospital stay, efficiency of the operation, and complications were analyzed.
Results:
In total, 157 inguinal high ligations were performed in 106 children (89 boys, 17 girls). The median age was 1.5 years (range, 25 days–11.6 years). The mean operative time was 15.8±3.4 minutes for the single-side procedure and 20.3±2.5 minutes for bilateral procedures. The mean postoperative hospital stay was 0.99±0.52 (range, 0.25–3 days). No postoperative bleeding, abdominal wall emphysema, abdominal viscera injury, or scrotal edema was found, and there were no known cases of postoperative testicular atrophy or hypotrophy. Ninety-three percent of the patients became fully mobile on the first postsurgical day. The median follow-up period was 17 months (range, 9–21 months), with no recurrence, no visible scars on the abdominal wall, and no foreign body felt in the inguinal region.
Conclusions:
This H-SIL approach is a safe and efficient method for pediatric inguinal hernia repair. The maneuverability is the same as that in the triport laparoscopic technique, and the cosmetic results are similar to those of single-port laparoscopic surgery.
Introduction
C
To preserve the advantages and overcome the limitations, we have recently developed a hybrid single-incision laparoscopic (H-SIL) high ligation approach using intracorporeal jumping purse-string sutures and knotting by a trocarless technique to treat pediatric inguinal hernias. We herein evaluate the technical feasibility, safety, and preliminary results of this approach.
Materials and Methods
This study was approved by the Ethics Committee of the Union Hospital of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Between June 2012 and June 2013, in total, 106 consecutive children (89 boys, 17 girls) with inguinal hernias (17 left-sided, 38 right-sided, 51 bilateral) repaired by this new approach were included in this study. The median age was 1.5 years (range, 25 days–11.6 years). Informed consent for the surgical procedure was obtained from all patients' parents or guardians before surgery. The patients' general clinical data, operative data, complications, and recurrences were noted. All of the patients had 100% follow-up, with 17 months (range, 9–21 months) as the median follow-up period.
Surgical procedures
Under general anesthesia, the patient was placed in the supine position, and a monitor was placed at the patient's feet. Pneumoperitoneum was established using a 5-mm trocar with an open technique through a vertical 5-mm incision at the umbilicus. The insufflation pressure was maintained between 6 and 12 mm Hg, based on the patient's age.
A 5-mm 30° laparoscope was introduced, and the whole abdominal cavity was inspected. A 3-mm grasping forceps was inserted at the horizontal ends of the umbilical incision laterally to the left of the laparoscope. Then, a needle holder was inserted through one 3-mm stab incision at the lateral side of the right rectus muscle at the level of the umbilicus without a trocar under laparoscopic vision (Fig. 1A). A 2-0 nonabsorbable suture was introduced into the peritoneal cavity through the anterior abdominal wall near the internal inguinal ring, with the suturing tail kept outside the peritoneal cavity (Fig. 1B). The 3-mm mini-forceps was used to grab and smooth the peritoneal fold between the vas deferens, vessels, and adjacent structures. The orifice of the hernia sac was closed intraperitoneally with a jumping purse-string suture around the internal inguinal ring (more specifically, a purse-string suture was made all around the orifice of the hernia sac, with a jump in the peritoneal fold, leaving a peritoneal gap over the cord structures to spare/prevent injuries to the vas deferens, spermatic cord, and testicular/or gonadal vessels) (Fig. 1C and D), and intraperitoneal knot-tying was performed with the grasping forceps holding the suture inside the abdominal cavity while an assistant pulled the end of the suture outside the abdominal cavity with minimum tension (Fig. 1E and F). The gas inside the hernia sac was expelled back into the abdominal cavity before knotting. Finally, the needle was removed transparietally from the abdominal cavity through the anterior abdominal wall (Fig. 1G), and the threads were cut adjacent to the skin, leaving the suture thread tied up intracorporeally.
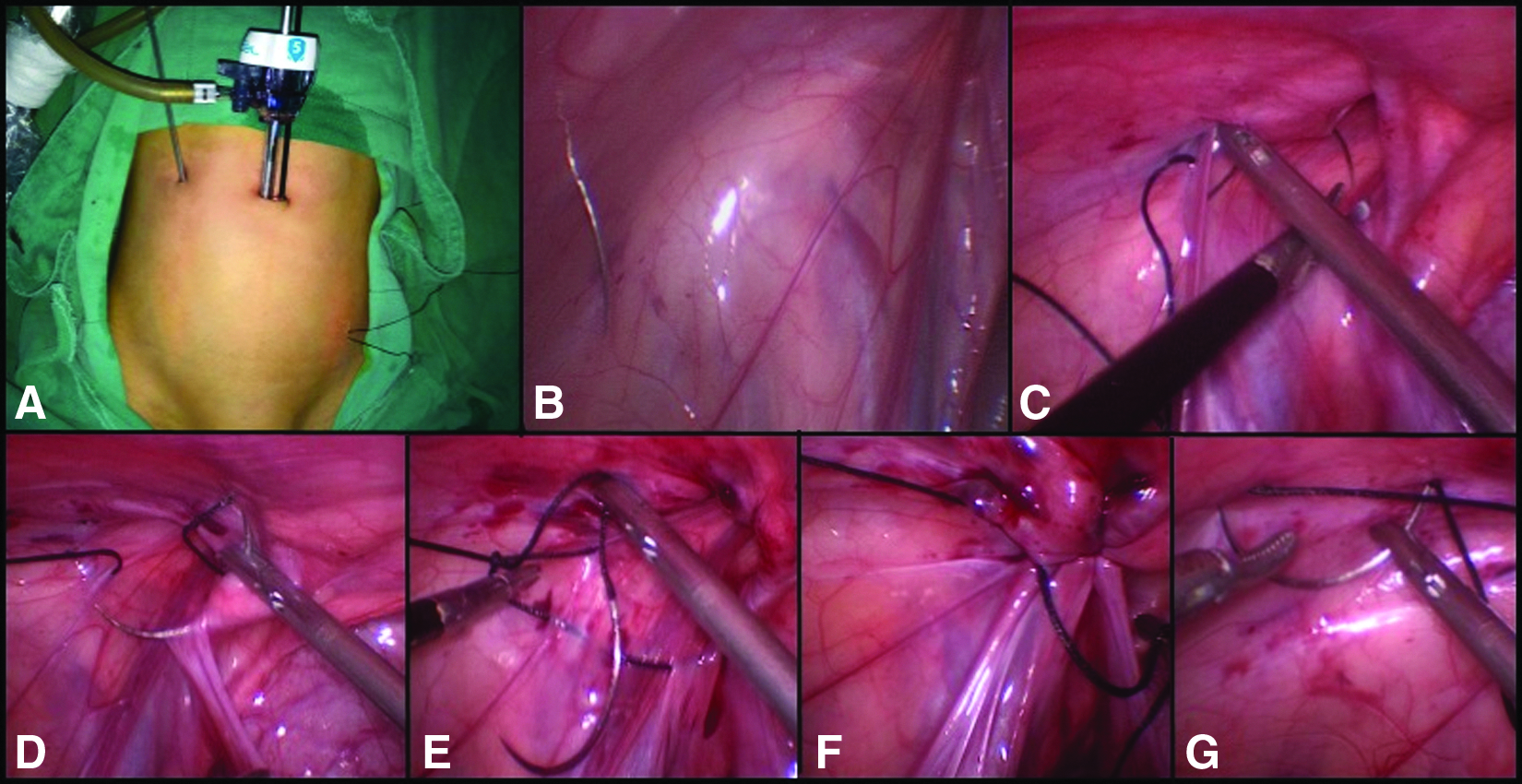
Surgical procedure of hybrid single-incision laparoscopic intraperitoneal ligation.
The peritoneum at the umbilicus was closed using 2-0 polyglactin 910 (Vicryl™; Ethicon, Somerville, NJ). The skin of the umbilicus and the 3-mm stab incisions were closed by skin glue without stitches.
Statistical analysis
The operative time, length of postoperative hospital stay, efficiency of the operation, and complications were analyzed. The results were expressed as medians with ranges or as means with standard deviations. Student's t test was used to compare the operative time between patients younger than 6 months and those older than 6 months. The odds ratio and chi-squared test were used to identify the significance of the identification of bilateral hernias. Univariate and multivariate linear regression analyses were used to identify the factors influencing the operating time. Potential influencing factors, such as the patient's age, gender, body weight, incarceration of the hernia, and the repaired side(s), were analyzed in multivariable analyses. A value of P<.05 denoted statistical significance. SPSS version 18.0 software (SPSS Inc., Chicago, IL) was used for all statistical analyses.
Results
There were 106 patients enrolled in this study (89 males and 17 females), with a median age of 1.5 years (range, 25 days–11.6 years). The mean operative time was 15.8±3.4 minutes (range, 10–30 minutes) in 55 cases of unilateral repair and 20.3±2.5 minutes (range, 15–35 minutes) in 51 cases of bilateral repair (Table 1). In 19 patients with a preoperative diagnosis of unilateral inguinal hernia, a contralateral hernia was identified during the laparoscopic surgery, and subsequent repair was performed. No conversion to open surgery was needed. No patient experienced inadvertent puncture of the intraabdominal viscus during the operation. The mean postoperative hospital stay was 0.99±0.52 days (range, 0.25–3 days). The postoperative pain was minimal, and 99 patients (93%) were out of bed, fully mobile, and discharged within the first 24 hours after surgery. Of the remaining 7 patients (7%), 5 complained about postoperative pain, and 2 had a longer recovery phase after general anesthesia.
Bilateral hernias were expressed as the total number of hernias, where the number in parentheses is the number of cases in which a contralateral hernia was discovered during the operation and was simultaneously repaired.
Seventeen (16%) of the patients were younger than 6 months old. For these patients, more bilateral repairs were performed (odds ratio=3.08, P=.043), and the present method was more time-consuming in these patients than in those older than 6 months (operative time, 21.1±5.3 minutes versus 17.4±4.2 minutes, P=.002). The main factor influencing the length of the operation was bilateral repair, according to the regression analysis (Table 2).
The median follow-up period was 17 months (range, 9–21 months), with no recurrence, granuloma, hydrocele, testicular atrophy, or foreign body felt in the inguinal region. According to the parents, the cosmetic result was excellent, with almost invisible scars on the right side of the umbilicus.
Discussion
In 1997, the initial application of laparoscopic ligation of an inguinal hernia in a human was reported by El-Gohary. 2 Since then, numerous laparoscopic techniques for the repair of pediatric inguinal hernias have been described. Among these techniques, laparoscopic percutaneous extraperitoneal closure of the hernia is a recently developed technique. The cosmetic outcomes of laparoscopic percutaneous extraperitoneal closure were outstanding.4–6 In addition, the introduction of preperitoneal hydrodissection, which can avoid trauma to the cord structures and help to enclose the hernia defect without peritoneal gaps, extended its scope of application. 7 However, increasing numbers of reports have described complications related to percutaneous extraperitoneal knotting, such as a stitching abscess, mild pain, granuloma, and discomfort due to the nonabsorbable knots, which can be felt as a foreign body in the inguinal region.1,5,6,8 Transumbilical endoscopic surgery with an intraperitoneal tie may be an alternative solution, but a one-hand suture and tie technique is needed in the procedure, which is a more challenging technique for surgeons. Furthermore, for cases with huge open internal rings of folded peritoneum (where the diameter of the hernia ring defect is larger than 2.5 cm), complete sealing of the internal rings using only one instrument is difficult. 9
The new technique that we have described is a hybrid version of the single-incision laparoscopic procedure. The modified steps in this procedure were the introduction of instruments without trocars, except for the laparoscope, and the use of an intracorporeal jumping purse-string suture on the internal inguinal ring. The stab incision made for the trocarless insertion of the 3-mm laparoscopic needle holder was closed using skin glue, and an almost invisible scar was present 2 months after the operation. The trocarless 3-mm grasping forceps, inserted through the umbilicus incision to the left of the laparoscope, was of great help to complete the jumping purse-string suture by making it possible to simultaneously grab and smooth the peritoneal fold, as well as facilitating the intraperitoneal knotting, regardless the size of the internal ring.
As with any innovative technique, there was a learning curve during our study; the suturing skills were acquired by training on a simulator for at least 50 successful attempts, and then the new skills were successfully applied in clinical practice. 10 At the beginning, we routinely made the stab incision 3 cm laterally to the right of the umbilicus, but at this position, the insertion of the needle holder was difficult, and the procedure was time consuming for proper suturing. We subsequently modified the introduction technique (changed the location of the mini-incision to the lateral border of the right rectus muscle at the level of the umbilicus), which made the procedure more fluent and practical. We felt comfortable with the operation after the first 10 cases.
Although using a purse-string suture without any peritoneum gap is preferred by many surgeons, jumping-suturing of the internal ring has been demonstrated as an effective technique, with no additional risk of recurrence.11–13 Moreover, an animal experiment demonstrated that the addition of minor peritoneal trauma caused by jumping-suturing induced sufficient scarring to provide a more durable repair. 14 So far, there have been no conclusive data indicating that childhood inguinal hernia repair can increase the risk of infertility, but Zendejas et al. 15 reported a diagnosis of infertility in 5% of the adults who had undergone primary inguinal hernia repair in childhood. For the sake of safety, it is necessary to minimize the potential risk of damage to the structures of the cord. In this study, the jumping purse-string suturing of the internal ring was adopted as a precaution to prevent potential damage to the spermatic cord, vas deferens, and gonadal vessels, rather than enclosing the hernia defect completely without peritoneal gaps. Based on our practice, grabbing and smoothing the peritoneal fold using the grasping forceps are the key to proper suturing, and thus to reducing the risk of recurrence, as well as to avoiding injury to the cord structures. In cases with a huge opening in the internal ring, which was previously reported to have a higher risk of recurrence, 16 two lap sutures or repair with the medial umbilical ligament can be added.
Evaluating the asymptomatic contralateral side is one of the advantages of the laparoscopic approach. However, there was still an approximately 0.9%–2.5% incidence of metachronous contralateral inguinal hernia (MCIH) after a negative laparoscopic exploration.17–19 According to our experience, children older than 6 months are more likely to have a small opening of the contralateral internal ring (Fig. 2A), but the difference between age groups was not statistically significant (odds ratio=2.087, P=.315). If not evaluated carefully, these patients may have a greater risk of developing an MCIH, contrary to the report of Nataraja and Mahomed. 20 Therefore, we suggest performing a routine contralateral groin exploration by using the grasping forceps under laparoscopic vision to prevent any risk of missing MCIH. In this study, a contralateral hernia was discovered during the laparoscopic surgery in 25.7% (19/74) of patients with a preoperative diagnosis of unilateral inguinal hernia, and subsequent repair was performed. In 3 of these cases, the contralateral hernias were not detected by simple exploration but were confirmed after pulling the fold of peritoneum covering the opening of the internal ring with the assistance of forceps (Fig. 2B). No MCIH has been found so far in this limited follow-up.
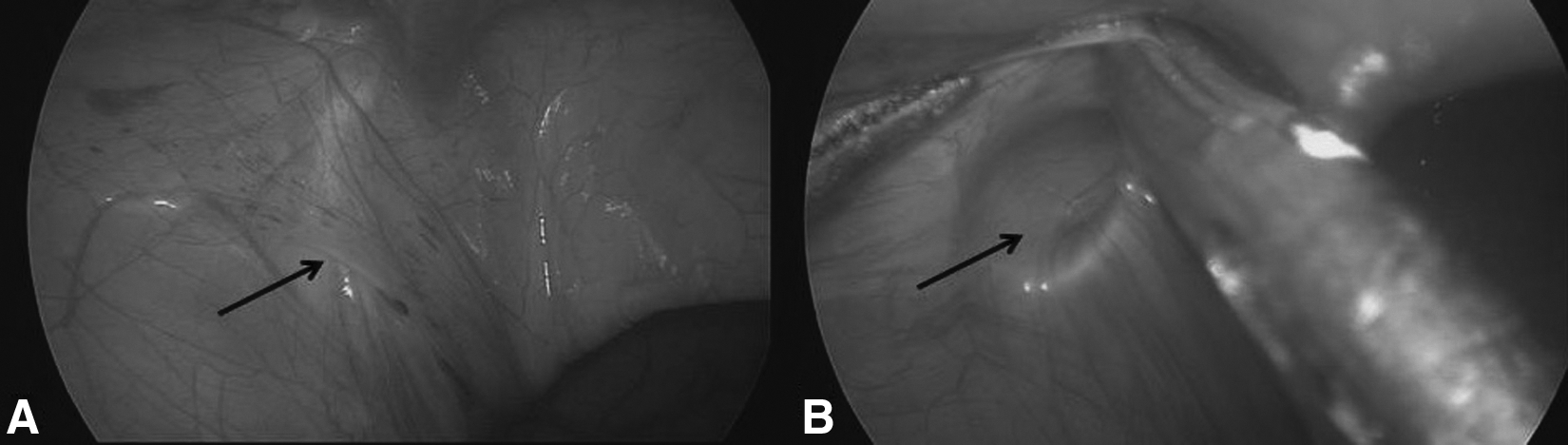
Contralateral groin exploration by a forceps and a needle holder.
Two main drawbacks in the present study have been identified. First, the follow-up period was too short to draw conclusions about the complications associated with the technique. A longer-term follow-up of the treatment modality is necessary. Second, it was slightly more difficult to manipulate the instruments without trocars in children with a thicker abdomen.
In conclusion, this H-SIL intraperitoneal ligation produces nearly the same cosmetic excellence as the single-port laparoscopic technique and also minimizes the potential risks of damaging the cord structures, MCIH occurrence, and discomfort related to extracorporeal knotting, and the new procedure only requires the maneuverability of a standard three-port laparoscopic technique. Therefore, it is well suited for the repair of pediatric inguinal hernias.
Footnotes
Disclosure Statement
No competing financial interests exist.