
Abstract
Abstract
Background:
Detailed preoperative delineation of biliary tract anatomy plays a pivotal role in guiding surgeons completing laparoscopic cholecystectomy (LC) smoothly. Hereby, we retrospectively investigated the potential impact of preoperative magnetic resonance cholangiopancreatography (MRCP) on LC.
Patients and Methods:
In this study, clinical data of LC patients who received conventional preoperative examinations from January 2008 to December 2010 (Ctrl group, n=300) versus conventional examinations plus extra preoperative MRCP assessment between January 2011 and December 2013 (MRCP group, n=300) were randomly retrieved. The ratios of conversion to open cholecystectomy and various postoperative morbidities were respectively analyzed.
Results:
In total, the incidences of operation conversion, postoperative remnant cystic duct stone, and choledocholithiasis in the MRCP group were 12 (4.0%), 1 (0.3%), and 2 (0.7%), respectively, all evidently lower than those in the Ctrl group: 41 (13.7%), 7 (2.3%), and 9 (3.0%). In addition, the MRCP group also presented with fewer cases of bile duct injury and incidental gallbladder carcinoma compared with the Ctrl group (1 versus 5 and 1 versus 2, respectively), although none of the variances was statistically significant.
Conclusions:
Our results demonstrated that preoperative MRCP had a robust safeguarding effect on LC and deserves further promotion.
Introduction
S
Magnetic resonance cholangiopancreatography (MRCP) is a noninvasive diagnostic technique. Because MRCP provides high-quality cross-sectional and projection images of the biliary tree, the technique harbors considerable sensitivity and specificity in detecting the bile tract lesions and anomalies.3,4 Because of the activities of accurately depicting biliary anatomy without need of contrast agent or intubation, MRCP has frequently been deployed as an alternative to percutaneous transhepatic cholangiography and endoscopic retrograde cholangiopancreatography (ERCP) in diagnosing hepatobiliary pancreatic ailments.3,5 Since January 2011, we have routinely used MRCP as a preoperative examination before LC. Herein, we retrospectively explored the potential effects of MRCP on LC.
Patients and Methods
Patients
All cases recruited to this study were approved by the Institutional Ethical Board of Taizhou People's Hospital, Taizhou, China, and conformed closely to the Declaration of Helsinki. 6 In brief, cases of 600 patients were randomly retrieved from 4503 candidates scheduled for LC from January 2008 to November 2013 according to the resident record keeping unit in our hospital. Of all participants, half (300 of 2157) underwent conventional preoperative examination mainly including abdominal type-B ultrasonography and blood biochemical test between January 2008 and November 2010 (Ctrl group), whereas another half (300 of 2346) received an extra MRCP assessment on the basis of previous examinations from January 2011 to November 2013 (MRCP group).
In the two different periods noted, all participants received standard three- or four-port LC performed by the same two experienced surgeons specializing in laparoscopic surgery for at least 8 years. No significant variances existed between the two groups in the age distribution, sex composition, constituent pathogenic factors (such as gallbladder stone, cholecystic polyps, and acute gallbladder torsion), or operation timing (including elective operation, emergency LC after an acute episode) (Table 1). Patients having a history of abdominal operation, preoperatively diagnosed with concurrent choledocholithiasis and Mirizzi's syndrome, suspected of having gallbladder carcinoma and gallbladder–intestinal fistula, or diagnosed with coexisting choledocholithiasis by intraoperative cholangiography (IOC) would receive some other operation and thus be excluded from this study.
Emergency operation after an acute episode.
Ctrl, control; MRCP, magnetic resonance cholangiopancreatography.
Evaluation indexes
The incidences of operation conversion, bile duct injury, incidental gallbladder carcinoma, remnant choledocholithiasis, and cystic duct stone were analyzed. The latter four complications were validated by postoperative MRCP, ERCP, relaparotomy, or pathological examination, respectively. The bile duct injury here was defined as the existence of bile leakage or abnormal bile duct ligation according to the aforementioned cholangiography and postoperative clinical presentations including fever, jaundice, right upper quadrant pain, etc.
Statistical analysis
Data for all parameters were expressed as mean±standard error of the mean and analyzed by Student's t test, while analysis of frequency data was performed with Pearson's chi-squared, continuity correction, or Fisher's exact test. For all tests, analyses were done using SPSS version 19.0 statistical software (SPSS, Inc., Chicago, IL), and a two-sided P<0.05 was defined as statistically significant.
Results
The morbidities of operation conversion, postoperative remnant cystic duct stone, and CBD calculus in the MRCP group were 12 (4.0%), 1 (0.3%), and 2 (0.7%), respectively, all remarkably lower than the respective values in the Ctrl group: 41 (13.7%), 7 (2.3%), and 9 (3.0%) (Table 2). Meanwhile, the MRCP group also presented with fewer cases of bile duct injury and incidental gallbladder cancer compared with the Ctrl group (1 versus 5 and 1 versus 2, respectively), although the variances were not statistically significant. In addition, a separate investigation demonstrated that the incidence of incidental gallbladder cancer in the total candidate population was 38/4503 (0.8%).
Ctrl, control; MRCP, magnetic resonance cholangiopancreatography.
Discussion
Traditionally, the definitive diagnose of gallbladder ailments is fundamentally based on type-B ultrasonography. 5 However, hepatobiliary ultrasonography inherently possesses some disadvantages: relative lower accuracy in diagnosing CBD ailments due to the existence of intestinal gas and imaging viabilities secondary to mutable probe direction and intuitive readability.5,7 In contrast, recently developed MRCP not only can depict the global coronal anatomy of biliary tract tree by using a hydrographic T2-weighted turbo spin-echo sequence with fat suppression, but also can facilitate detecting fine lesions through tracking different transverse sections.3,8 In the present study, MRCP prior to LC evidently reduced the incidences of conversion to open cholecystectomy, postoperative remnant cystic duct stone, and choledocholithiasis. The variations of the morbidities of bile duct injury and unsuspected gallbladder cancer in the two groups were not statistically significant, but we speculate these might be partly due to innately low incidences and not large enough sample scales. In any case, these two complications were also greatly decreased since the introduction of preoperative MRCP. To our experience, preoperative MRCP might safeguard LC through multiple aspects.
A clinically “silent” CBD stone usually coexists with gallstones without any prototypic clinical presentations of fever, jaundice, or right upper quadrant pain (Fig. 1a).3,8 Unfortunately, these patients are liable to be misdiagnosed by conventional ultrasonography due to the distortion effect of intestinal gas and thereby inappropriately receive mere LC, leaving a problem of residual choledocholithiasis. Theoretically, this dilemma may be prevented by IOC or made up by postoperative endoscopic sphincterotomy. In fact, we had indeed diagnosed considerable amounts of choledocholithiasis and avoided this awkwardness via IOC in the early stage when we had not used preoperative MRCP. However, the incidence of remnant choledocholithiasis was still frustrating.
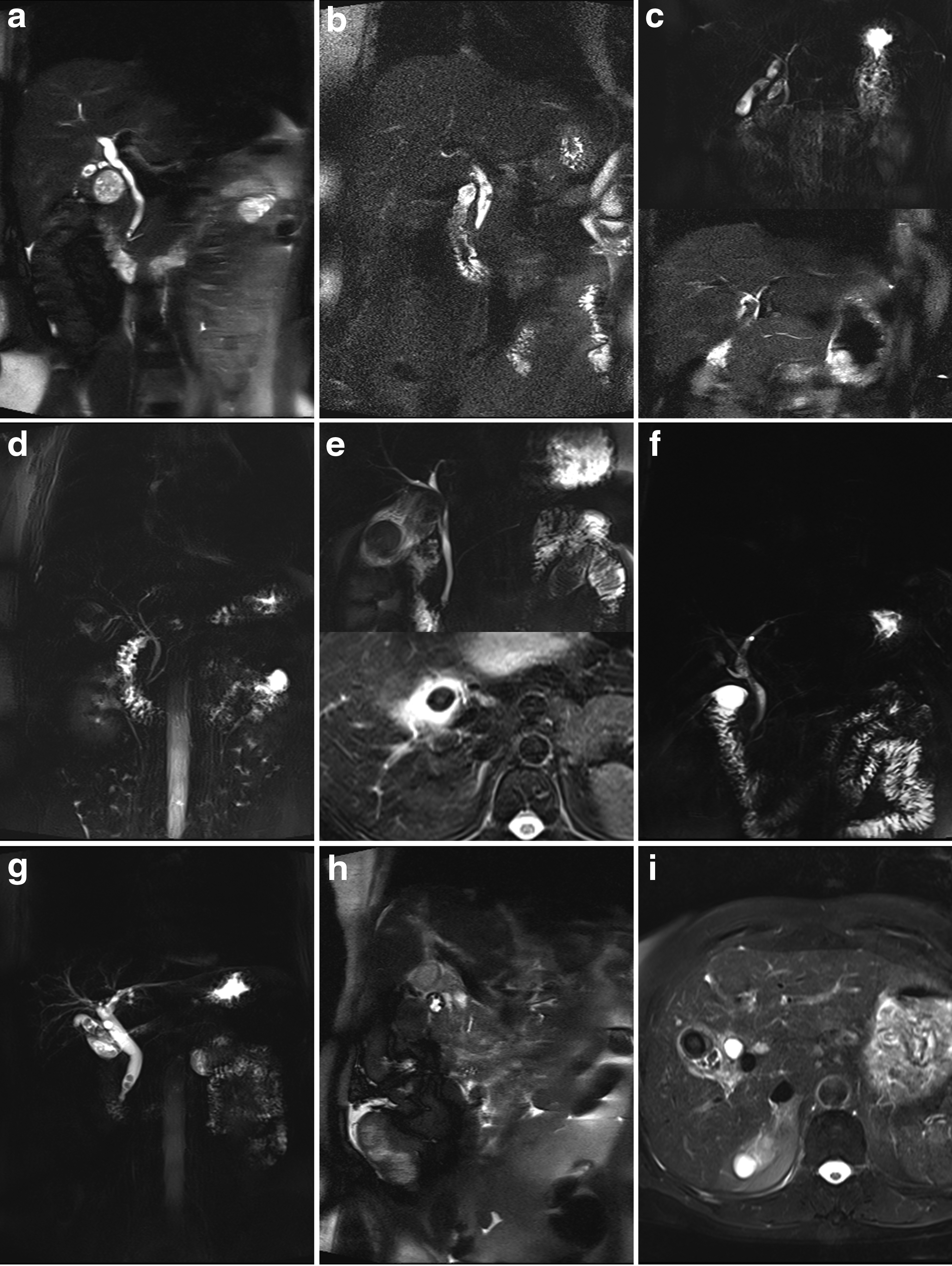
Prototypic magnetic resonance cholangiopancreatography images:
In our experience, there are two explanations: we might miss IOC because some choledocholithiasis patients possessed an undilated CBD, or a blocked cystic duct hindered the IOC application. For the endoscopic sphincterotomy precedure, we also observed failed cases sometimes because of the presence of a huge CBD stone or duodenal diverticulum, besides an increased hospital stay and cost as well as potential endoscopic sphincterotomy–related morbidity and mortality. 8
In this sense, preoperative MRCP could instruct the surgeon to convert LC to other appropriate approaches such as laparoscopic choledocholithotomy or ERCP plus LC. On the other hand, negative ERCP, transcystic cholaniography, and laparoscopic choledocholithotomy always happen in patients with a dilated bile duct diameter of >8 mm. 8 For these patients, MRCP can also minimize these unnecessary procedures through portraying the bile duct structure in detail. In addition, remnant CBD lithiasis is occasionally found in gallstone patients who undergo LC despite a negative preoperative MRCP or ERCP.
One of the most important causes for this dilemma is that part of the cystic duct stone has slipped into the CBD during the dissection course (Fig. 1b).3,8,9 In this context, the preoperative perception of cystic duct lithiasis by MRCP could alert the surgeon to mobilize the cystic duct more gently and squeeze the stone toward the gallbladder before eventual ligation.
It is well known that the biliary tract usually harbors congenital malformations such as a double gallbladder, the presence of an accessory right hepatic duct, abnormal bile duct bifurcation, and cystic duct insertion (Fig. 1c and d).3,10,11 Besides, Mirizzi's syndrome represents another important risk factor in which the swollen gallbladder neck compresses the CBD and results in CBD stricture (Fig. 1e).10,12 Failure to recognize these variants may lead to disastrous bile duct ligation or resection (Fig. 1f). In such cases, accurate preoperative MRCP could help the surgeon away from these “traps” through choosing an optimal operation schedule other than LC and paying greater attention in dissecting Calot's triangle.
Postcholecystectomy syndrome refers to the persistence of antecedent symptoms and emerges in approximately 10%–40% of patients following LC. 13 Actually, a few of these patients may harbor a residual gallbladder or a long cystic duct stump, although the etiology of postcholecystectomy syndrome is mainly nonbiliary (Fig. 1b and g).3,13,14 Thus, MRCP could foretell surgeons of the presence of a long parallel cystic duct with the CBD and remind them of ample cystic duct resection.
Gallbladder–intestinal fistula can be occasionally encountered in cholecystectomy (Fig. 1h). Failure to identify this rare entity may give rise to intraoperative contamination and iatrogenic injury. 15 Through prototypic MRCP signs of continuity interruption in the gallbladder wall as well as air–fluid level within that gallbladder, a hepatobiliary doctor might foresee this ailment and judiciously adopt bowel preparation and other favorable operation schedules.
Gallbladder carcinoma represents a sort of notorious neoplasm and ranks first among the primary biliary tract malignant tumors. 16 As gallbladder carcinoma frequently coexists with gallstone or gallbladder polyps, early patients may only presents with clinical symptoms of acute cholecystitis and thereby incorrectly receive mere LC (Fig. 1i). Due to the potential intraoperative dissemination, these patients may still face a gloomy distal outcome despite the relaparotomy following pathological assessment. 17 To avoid this embarrassing situation, elaborate precautions consisting of contrast magnetic resonance scanning, tumor biomarker assessment, and necessary intraoperative instance pathological examination in the suspected cases preliminarily assessed by preoperative MRCP remain significant. In the current study, the morbidities of unexpected gallbladder carcinoma between the MRCP group (0.3%) and the Ctrl group (0.7%) presented with no statistical difference. However, the incidence of incidental gallbladder carcinoma in the total 4503 candidate cases is 0.8%. This relatively lower morbidity according to previous literature (0.19%–3.3%) may due to our adoption of the preoperation MRCP, more or less. 18
In conclusion, our study clearly revealed the instructive impact of MRCP on LC in terms of the significantly decreased ratio of operative conversion and various morbidities, including residual cystic duct stone, choledocholithiasis, etc. Inevitably, the introduction of MRCP will increase hospital expense (about 5% in our hospital). But, the potential benefits may be quite satisfactory. We considered that preoperative MRCP played a pivotal safeguarding role in LC practice and is worth further clinical popularizing.
Footnotes
Disclosure Statement
No competing financial interests exist.