
Abstract
Abstract
We present our technique for a totally robot-assisted laparoscopic Roux-en-Y gastric bypass. Moreover, data are presented in relation to a single-surgeon experience with use of the robotic platform in bariatric surgery. We reviewed a single surgeon's console and room time from 2009 to 2013 for all robot-assisted Roux-en-Y gastric bypasses (RARYGBs). Revision operations were excluded. There were in total 168 robotic bariatric operations in this time frame. The number of cases performed each year and the cumulative number of each operation were considered as well. The change in console time as related to the number of cases and the change in room time as related to the console time and number of cases were investigated. Complications during this time and their frequency were noted and described. The console time for RARYGB ranged from 131±46 minutes in 2010 to 94±29 minutes in 2013 (P<.05). There were in total 22 complications, for an overall complication rate of 13.1%: four anastomotic strictures (2.4%), seven marginal ulcerations (4.2%), two gastrointestinal bleeds (1.2%), five internal hernias (3.0%), two abdominal pains requiring diagnostic laparoscopy (1.2%), and two gastrointestinal leaks (1.2%). There were no deaths. In this series, the console surgeon performed 168 RARYGBs and had a leak rate of 1.2% and a mortality of 0% within the first 66 cases and a 0% leak rate over the next 102 cases. Thus, we believe that the robot has a decreased caseload requirement to reach proficiency with comparable outcomes versus both the hybrid and purely laparoscopic approaches.
Introduction
T
Currently, over 250,000 gastric bypass cases are performed annually across the United States. 2 Our institution, a designated Bariatric Center of Excellence, began performing robotic bariatric procedures in 2005, with nearly 1000 cases performed to date. The learning curve has proven to be shorter than that for standard LRYGBs. 3 In addition, the morbidity and mortality associated with the robotic platform have been proven to be equal to or superior to those of laparoscopic approaches. 4 Over the past several years, our group has developed a standard approach to a totally RARYGB operations. We have found this approach to be safe with complication rates below the national average. 5
We believe that it is important to standardize techniques among surgeons to facilitate fruitful discussion and promote the advancement of technology, especially as more general and bariatric surgeons are beginning to use robotics in their everyday practice. Therefore, in this article, we describe our current technique as it has been modified since the first descriptions published in 2005–2010.2–4 This technique has never been explained by us or any other surgeons in the amount of detail described below with corresponding high-definition photographs.
In addition, we give data for the RARYGB learning curve for the first 5 years of a fellowship-trained robotic surgeon coming into practice as it is related to the time spent on the robotic console and the total time in the operating room, and how these times have changed over this same period, in particular, as it relates to the change from the hybrid to the totally robotic technique described below.
Finally, we report the complication rates for our primary RARYGB during this learning curve. Major complications and their frequency are reported for both the hybrid and totally RARYGBs that were performed over the first 5 years of the surgeon's career.
Technique
Preparation and port placement
To perform a single-quadrant, totally RARYGB, the patient is positioned supine with the left arm tucked. Morbidly obese patients require special attention to appropriate padding of pressure points and support of the lower extremities with foot rests. The bed is placed in its lowest position, to allow adequate room for docking the patient cart. The patient is positioned in approximately 15° of reverse Trendelenburg position, and a 34–36 French bougie is placed orally into the esophagus and proximal stomach. The patient is prepped in a standard fashion, and the abdomen is draped in a pentagon configuration (Fig. 1) to allow access to the entire upper abdomen.

The patient is draped in a pentagon fashion.
Ports are placed in a relatively straight line across the abdomen 1–2 cm above the umbilicus, depending on the patient's body habitus. The first 5-mm port is placed in the left upper quadrant approximately 8 cm below the costal margin in the midclavicular line. This surgeon prefers a direct entry technique under direct visualization. After insufflation of the abdomen, a 12-mm camera port is generally placed 1–2 cm above the umbilicus and slightly to the left of midline to avoid interference with the falciform ligament. Once access to the abdomen is gained, the remaining ports are placed based on internal landmarks.
The Nathanson® retractor (Cook Medical®, Bloomington, IN) is placed just below and to the left of the xiphoid process. Once the retractor is inserted, the left lobe of the liver is retracted upward, exposing the esophageal hiatus, and secured using a flexible arm device (Bookler®; Mediflex® Surgical, Islandia, NY) mounted to a laparoscopic Bookwalter® (Antioch, TN) post placed to the right side of the bed, above the patient's right shoulder. The flexible arm device is placed as low as possible and up against the patient so as to keep a minimal profile and not interfere with the docking of the robot or the #2 arm once docked. Once the Nathanson retractor is in place, the right lateral (5-mm) and assistant (12-mm) ports are placed, followed by the lateral left upper abdominal (5-mm) port. If a direct entry technique is used, the left subcostal port should be exchanged for an 8-mm robot port to accommodate the fenestrated grasper and shears. Once all of the ports are in place (Fig. 2), the robot is docked.
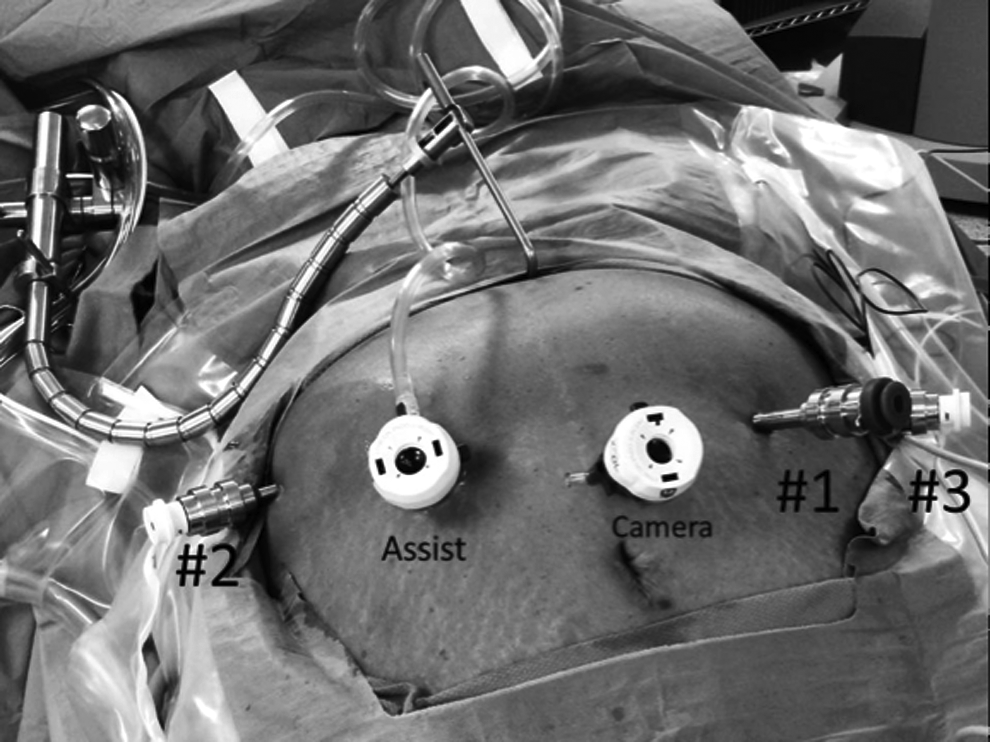
The snake and ports are shown in their ideal configuration.
Docking
Early in our robotic Roux-en-Y gastric bypass experience, we were using the standard da Vinci system. Due to limited range of motion of the arms, this mandated that we dock the robot over the patient's left shoulder. Once the S and Si systems were used, we began to dock the robot parallel to the left side of the bed. This allows for space at the head of the bed for anesthesia and intraoperative endoscopy (Fig. 3). All numbers of the individual robot arms should face out toward the right side of the bed to allow the greatest range of motion and to prevent interference among the arms, the camera port, and the assistant port. The cart is positioned so that the camera is directly over the camera port. The generally accepted “sweet spot” (a designation on the camera arm for greatest range of motion) is unnecessary.

The robot cart is brought in parallel to the left side of the bed just far enough to dock the camera. Note that the numbers on the arms face the right side of the bed.
Creation of the small pouch
The dissection of the angle of His is the first step of the robotic Roux-en-Y gastric bypass. This is done to ensure a clear path when the posterior stomach is dissected through the lesser sac. The fenestrated bipolar grasper (arm #1) and two bowel graspers (arms #2 and #3) are used because they are atraumatic and allow precise dissection with excellent hemostasis. The fundus of the stomach is retracted toward the right foot with the #3 bowel grasper, the angle is retracted inferiorly with the #2 grasper, and the fenestrated bipolar is used to bluntly dissect the epiphrenic fat pad off of the left crus (Fig. 4). This is done until the base of the left crus is well visualized.
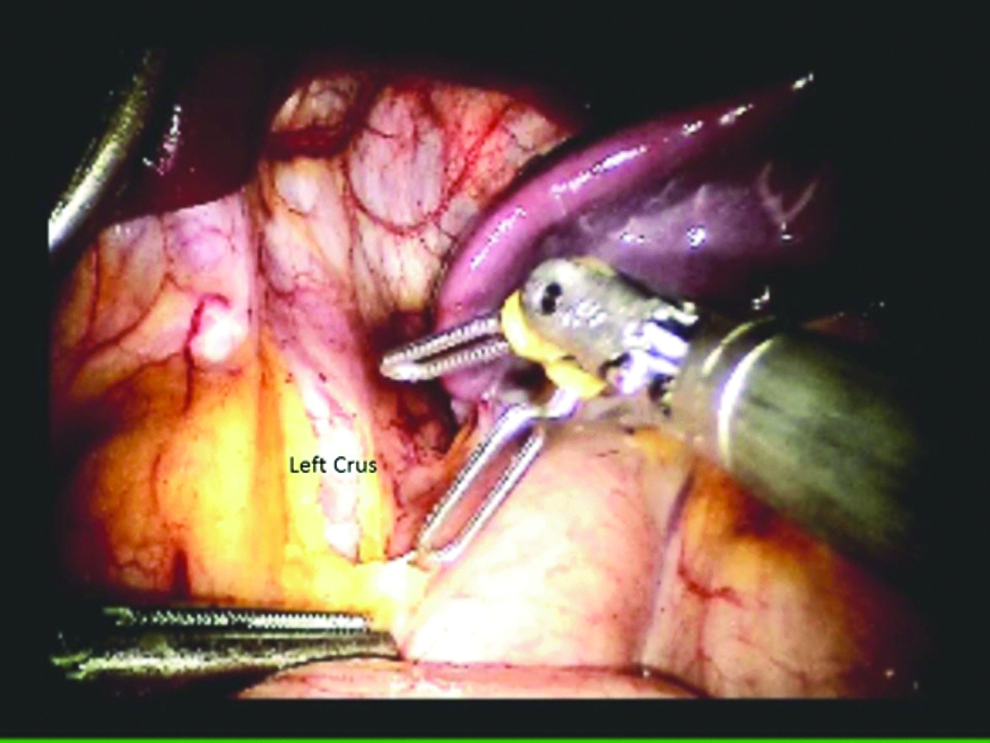
The epiphrenic fat pad is dissected from the left crus at the angle of His.
The pars flacida is then opened inferior to the left gastric vessels (Fig. 5). This space must be clearly identified with accurate localization of the vessels to avoid inadvertent injury. We insist on visualizing the posterior surface of the stomach prior to stapling, to ensure that we are in the correct plane and will be able to proceed cranially toward the base of the left crus. When we are confident that we are in the lesser sac and the vessels are protected, a vascular load stapler is fired across the gastrohepatic ligament up to the edge of the lesser curve of the stomach. Next, a green load with buttressing material is fired transversely across the stomach. Before the stapler is fired, the bougie is directed down to the stapler load to ensure proper placement of the staple line. After the first staple fire, the posterior dissection continues until the base of the left crus is clearly identified and a clear window is created for placement of the next staple load. This staple load is directed superiorly, toward the angle of His, creating a small gastric pouch of approximately 20–30 mL (Fig. 6). We find that keeping the oral gastric tube or bougie in the proximal stomach helps to calibrate an appropriately sized pouch.
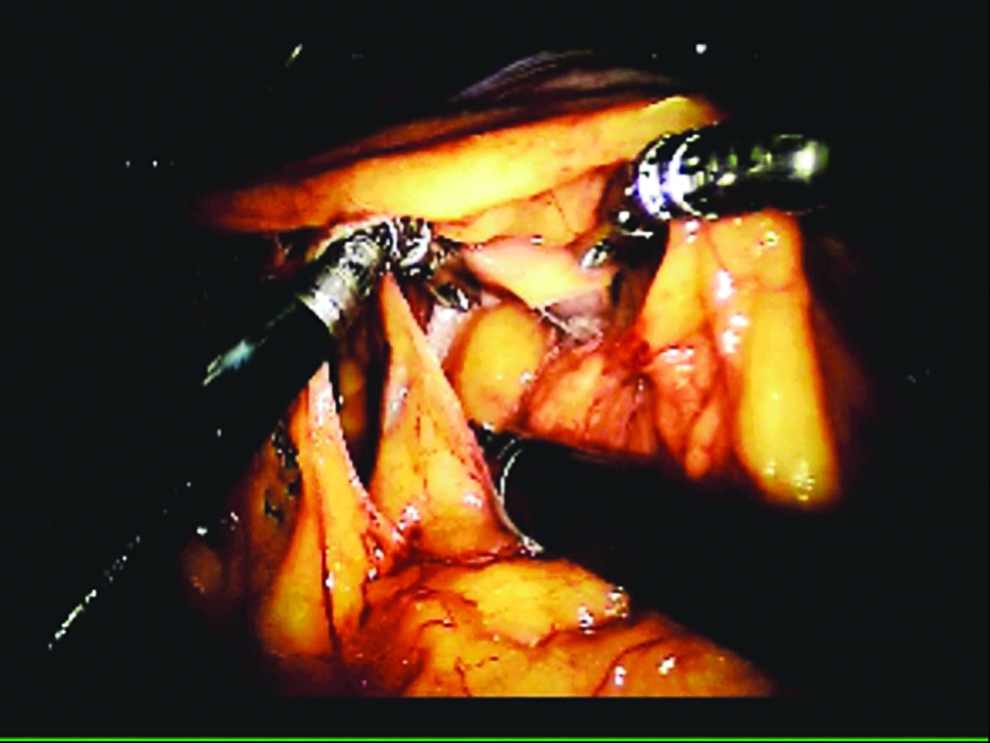
The pars flacida is opened to see the posterior stomach and identify the left gastric vessels.
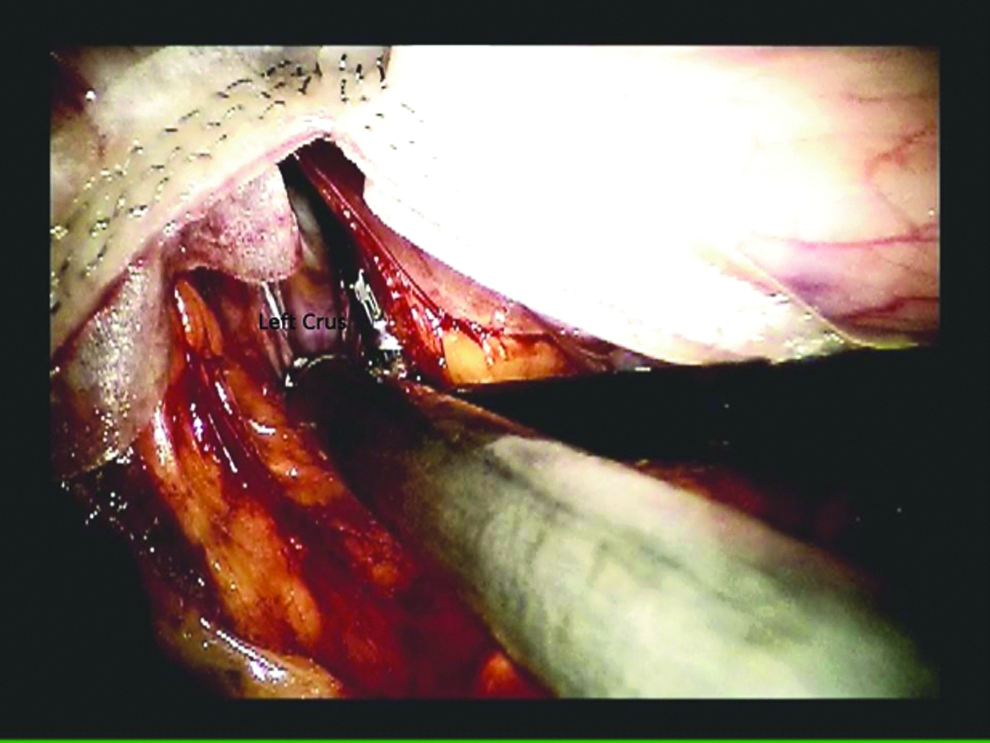
The base of the left crus is clearly seen, and a window is widened to accommodate the last green load.
At this point, the pouch and remnant stomach are completely separated by firing the blue staple load without buttress material (Fig. 7), and the remnant stomach is placed under the fat of the greater curvature to decrease the likelihood of a fistulous connection.
The pouch is completely separated from the remnant stomach.
Positioning of the jejunal loop
After the pouch has been created, the omentum is retracted cephalad to expose the transverse colon and the ligament of Treitz. The jejunum is then run in a loop-like fashion (proximal bowel to the patient's left, distal bowel to the patient's right) to the small pouch to set up the creation of the hand-sewn gastrojejunostomy. The length of the biliary limb is determined at this time. Typically a 75-cm biliary limb is created. In our practice, the omentum is only divided if it is very thick and it is difficult to place the jejunum adjacent to the gastric pouch. This is rare, occurring in less than 10% of cases. The jejunal loop is held in place with the #3 bowel grasper (Fig. 8).
The loop is held in place with the #3 bowel grasper, and the #1 and #2 arms are equipped with needle drivers.
Creating the gastrojejunostomy
The bipolar grasper and bowel grasper in arms #1 and #2 are replaced with needle drivers. A purple, 2-0 polyglactin 910 (Vicryl®; Ethicon, Cincinnati, OH) suture cut to 9 inches in length is inserted through the assistant port. This will form the posterior and anterior outer rows of the anastomosis. The suture is started at the medial aspect of the pouch and run toward the lateral edge for the posterior row (Fig. 9).

The back row is run from the medial to lateral aspect of the small pouch.
After the posterior, outer row is completed, a 1.2-cm gastrotomy is created using monopolar shears (Fig. 10). It is important to ensure that the orogastric tube or bougie being used to create the pouch is sitting anterior to the staple line to facilitate correct placement of the gastrotomy. About a 5-mm rim of stomach is left anterior to the back row to allow adequate tissue for the inner, posterior row of the anastomosis. An enterotomy of equal size is created adjacent to the gastrotomy. The orogastric tube or bougie is passed through the gastrostomy to ensure an adequate diameter.

Gastrotomy being made with monopolar shears.
The inner rows of the gastrojejunostomy are created using two 2-0 Vicryl sutures that have been sutured together to form a double-armed suture (Fig. 11). The length of each arm is 12–15 cm. The posterior inner row is started with the lateral suture placed inside the stomach at the lateral corner of the gastrotomy and then outside to it on the jejunum. The medial suture is placed in a similar fashion next to it and run from lateral to medial to create the entire posterior inner row. Once this posterior inner row is brought to the medial corner of the gastrotomy, the lateral suture is picked up again and run around the lateral corner to begin the anterior row.

A double-arm Vicryl suture is used to create the posterior and anterior inner rows.
At this time, the bougie is passed across the anastomosis (Fig. 12). It is inserted into what will become the Roux limb for about 15 cm, and then the #3 robotic arm is placed on top of this for downward traction and proper alignment of the anastomosis for final closure. This third arm can also be used as the surgeon approaches the medial corner to expose the most medial aspects of the anastomosis. The key to this is to keep this instrument low so there is no interference with the needle drivers.

The bougie is passed across the gastrojejunostomy after the posterior inner row is completed.
The anterior inner row is completed in a running fashion from lateral to medial, until it meets the posterior inner row suture. The needle is removed from one of the sutures, and the two ends are tied to complete the inner row of the anastomosis.
The outer row is continued anteriorly with the same suture used to create the posterior row. It is picked up from the lateral aspect, and a continuous, Lembert suture is performed (Fig. 13). This is run until the tail of the original posterior suture is met, and the sutures are tied. The gastrojejunostomy is now complete.

The outer anterior row of Vicryl suture is started laterally and run medially.
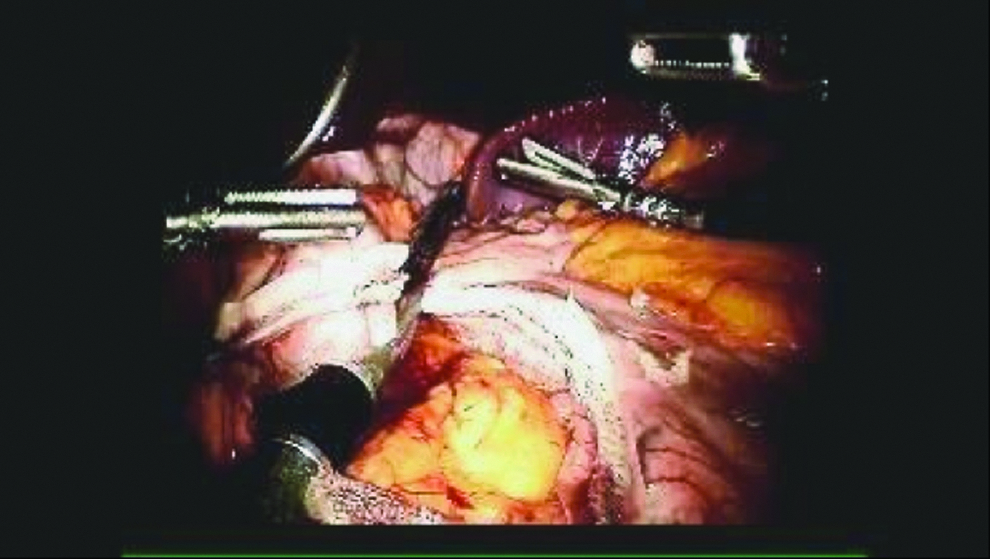
The bougie is then removed, and the Roux and biliary limbs are created. This is done by creating a small mesenteric window just lateral to the gastrojejunostomy. Two needle drivers are used to bluntly dissect a window just large enough to accommodate the the stapler. Mesenteric division is unnecessary when using this technique. The white staple load is used to transect the bowel as close to the anastomosis as possible to limit the amount of defunctionalized bowel or “candy cane” left at the pouch (Fig. 14). By dividing the bowel here, the biliary limb remains in the left upper quadrant, and the Roux limb is run so that the bowel lies open toward the right upper quadrant. This technique facilitates the completion of the operation in a single quadrant, allowing for an efficient totally robotic gastric bypass.
The jejunum is divided lateral to the gastric pouch to form the biliary and Roux limbs.
Creation of the jejunojejunostomy
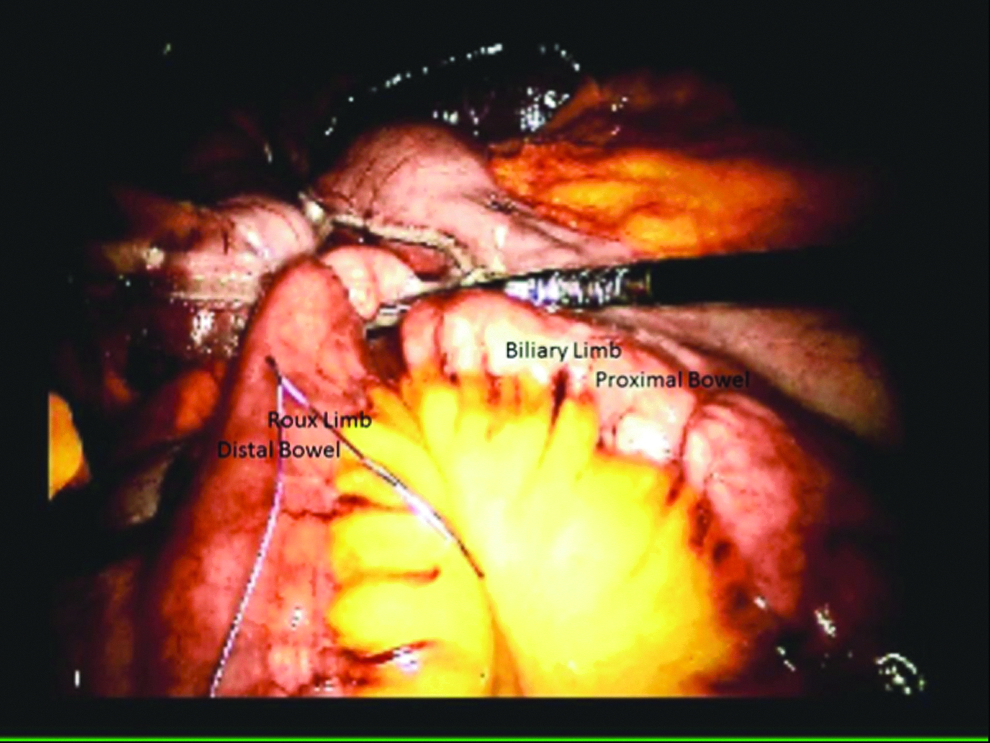
The Roux limb is then run to its desired length (generally about 150 cm) and brought up in a side-to-side fashion with the biliary limb. A simple interrupted silk suture is placed in each limb to join them together and facilitate the enteroenterostomy (Fig. 15). The suture is taken on the biliary limb first, and it is placed about 15 cm proximal to the stapled end to allow adequate length for the stapler to be inserted. This stay suture is then held with the #3 grasper, to keep the limbs together in the left upper quadrant. The needle driver in the #1 arm is used to position the limbs together for anastomosis. Once the two limbs are apposed, enterotomies are created adjacent to one another, using the assistant's energy device. Note that the enterotomies are kept as small as will accommodate the stapler, to minimize the size of the common enterotomy.

A stay suture is placed from the biliary limb to the Roux limb in a side-to-side fashion.
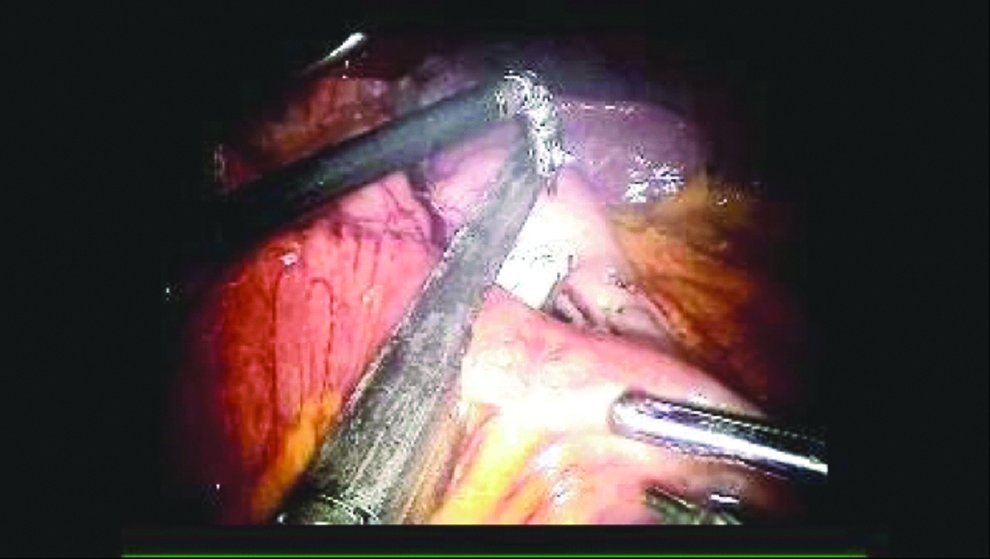
The stapler is placed into the two enterotomies. It is best to line up the stay suture and the direction of the stapler to facilitate inserting the stapler completely into the bowel (Fig. 16). Once this is done, the stapler is fired, and the common enterotomy is created as a functional end-to-end anastomosis.

The stapler is placed in-line with the stay suture in the left upper quadrant, and the common enterotomy is created.
The common enterotomy defect is closed with a continuous running 2-0 Vicryl suture. In an unusual fashion, it is preferable to close this common enterotomy defect starting at the near end and running it away from the camera (Fig. 17). This aids in visualizing the most difficult part of the closure near the mesenteric defect and ensures that good, full thickness bites are taken. The suture is completed in a single layer and tied to itself.

The common enterotomy defect is closed with a continuous running suture going away from the camera.
Closure of the mesenteric defect
The mesenteric defect between the biliary and Roux limbs is closed using a continuous running 2-0 silk suture, starting at the base of the mesentery. It is run up toward the bowel in three or four bites. The Roux and biliary limbs are incorporated into the mesenteric closure by taking small bites of each at the top of the closure. The defect is then cinched down so that the jejunojejunostomy is pulled down to the base of the mesentery. Another interrupted throw is taken across the mesentery, locked, and tied to its own tail (Fig. 18). The single-quadrant, totally robotic gastric bypass is now complete.

The mesenteric defect is closed in a purse-string fashion.
Leak test
The final steps include testing the gastrojejunal anastomosis and applying fibrin glue to raw surfaces. Because the robot is parallel-docked, access to the head and mouth is not compromised, and we can leave the robot docked for this portion of the case. This assists in visualization of an air leak, if present, with three-dimensional magnification and allows for direct repair using the robot.
The #1 arm is undocked, and a suction irrigator is placed into that port. The bowel clamp is placed through the right upper quadrant assistant port. The console surgeon places the endoscope down the mouth, the pouch is insufflated, and the anastomosis is tested under water while being visualized by the assistant. The scope is placed through the anastomosis, and all the air is removed after the integrity of the anastomosis is verified. If a leak is encountered and it is well visualized, then direct suture repair is performed using the robot. The endoscope remains within the lumen to stent the anastomosis. If this intervention fails to resolve the air leak, the patient is managed conservatively with nothing by mouth for 24 hours and close clinical monitoring after initiation of diet. Most small air leaks are subclinical and rarely result in clinically significant sequelae. If no air leak is detected, then the surgeon returns to the console to assist with suctioning the remaining fluid and application of fibrin glue. At this time the robotic is undocked, the assistant and camera ports are closed with the laparoscope, and the skin is closed.
Results
Methods
We reviewed a single surgeon's console and room time from 2009 to 2013 for all RARYGBs. Revision operations were excluded. There were in total 168 robotic bariatric operations in this time frame. The number of cases performed each year and the cumulative number of each operation were considered as well. The change in console time over time as related to the number of cases and the change in room time as related to the console time and number of cases were investigated. Complications during this time and their frequency were noted and described.
Simple descriptive statistics using average±standard deviation were used to show the number of cases, console time, and room time changes over time. Complication rates were reported as percentage of total cases.
Where a linear regression relationship existed within a set of data and the plotted data on the graph showed a linear relationship (R 2 >|0.75|), algebra was used to extrapolate. The Pearson coefficient (r) was used to determine the relationship between sets of data and was considered significant when r>|0.75|. Datasets were compared using a two-tailed, paired Student's t test, and significance was set at P<.05. Statistics and calculations were performed using an Excel® (Microsoft, Redmond, WA) spread sheets.
Learning curve
Console time
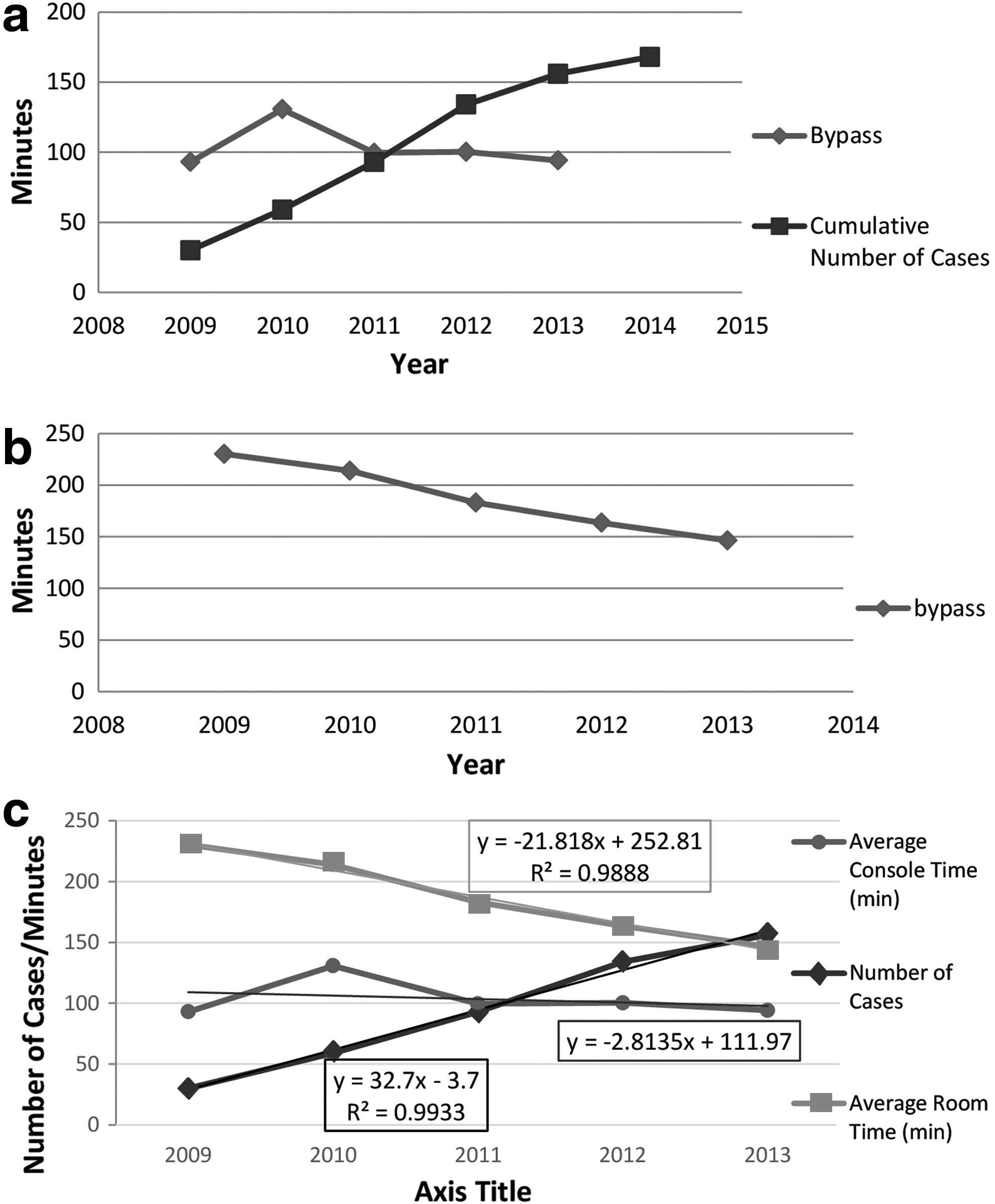
The console time for RARYGB ranged from 131±46 minutes in 2010 to 94±29 minutes in 2013 (P<.05).
Overall console time decreased over the 5 years (Fig. 19a). However, there was a significant increase in console time for the RARYGB between 2009 and 2010 (P<.01). During this year, the surgeon converted to a totally robotic RARYGB instead of the original hybrid technique. The totally robotic RARYGB includes creation of the pouch and Roux limbs at the console as described above, whereas the hybrid technique would do this laparoscopically and then dock to sew the gastrojejunostomy and common enterotomy only. Naturally, this added to the console time of the totally RARYGB. Within 18 cases, however, console time normalized to less than 98±35 minutes. This was not significantly longer than hybrid console time in 2009 (P=.314), and the console time remained this way after 2010. Despite the initial increase in console time, however, the room time steadily decreased (22 minutes per year on average; R 2 =0.99) (Fig. 19b).
The learning curve in
Console time did not correlate with all 5 years of case volume for the RARYGB, presumably because of this change in technique and subsequent increase in console time. However, considering only 2010–2013, when times normalized, there was a correlation (R 2 =0.88). Given this correlation over just this period of time, which totaled 102 cases, the surgeon was able to reduce the difference in console time by 50% within the first 35 cases (Fig. 19c).
Overall console time steadily decreased as the surgeon gained more experience and significantly correlated with number of cumulative cases (r=−0.80).
Room time
Room time for the RARYGB consistently and significantly decreased from 230±58 minutes to 147±43 minutes (P<.001, R 2 =0.92) between 2009 and 2013 (Fig. 19b). As mentioned above, this is despite the increased console time when changing from a hybrid to totally robotic Roux-en-Y gastric bypass technique in 2010. Room time for the RARYGB significantly decreased with the total number of robotic cases performed (r=−0.98) but not specifically with the total number of RARYGBs performed.
Complications
Table 1 shows the complications for the 168 cases. There were in total 22 complications, for an overall complication rate of 13.1%: four anastomotic strictures (2.4%), seven marginal ulcerations (4.2%), two gastrointestinal bleeds (1.2%), five internal hernias (3.0%), two abdominal pains requiring diagnostic laparoscopy (1.2%), and two gastrointestinal leaks (1.2%). There were no deaths.
Seven of the 22 complications were noted with the first 66 cases (10.6%), using the hybrid technique: two internal hernias (3%), one stricture (1.5%), two marginal ulcerations (3%), and two leaks (3%).
The subsequent 102 cases using the totally robotic technique described above, beginning in 2010, had 15 complications (14.7%): three internal hernias (2.9%), three strictures (2.9%), two gastrointestinal bleeds (2.0%), five marginal ulcers (4.9%), and two abdominal pains (2.0%). There were no leaks in this group.
Discussion
These data describe an efficient method for performing the single-quadrant, totally robotic Roux-en-Y gastric bypass operation. Console time significantly decreased over the first 3 years and then stabilized. The rate at which the console time diminished once the totally robotic technique described in this article was applied correlated with the number of cases performed and was significant. In fact, the total number of robotic cases, in general, correlated with faster learning curves (data not shown).
The ability of the robotic platform to decrease room time with the addition of other robotic steps that were traditionally done with standard laparoscopic techniques demonstrates that, in our hands at least, robotics is faster than traditional laparoscopic techniques once the short learning curve is completed. This is clearly evident by the increased console time but overall decrease in room time, which was significant. In fact, the totally robotic technique facilitated the decrease in console time within a 1-year time frame, or 35 cases. This is important knowledge to understand and to set expectations as surgeons begin to do these operations themselves for the first time.
Operative cost may be reduced by reducing operative time. In a large series published of more than 2000 LRYGBs, 6 the operative time was reported to be 155 (range, 53–493) minutes. This is certainly comparable to what we have been able to produce in fellowship-trained robotic surgeons within the first 3 years of practice (Fig. 19b). In fact, the operative time of 155 minutes reported above is higher than the total “wheels in to wheels out” room time reported in this series of 146 minutes at the end of the 5 years. The actual operative time reported in these data was only 94 minutes at the 5-year mark. With the average cost of operating room time for complex surgeries (e.g., bariatric surgery) at approximately $55/minute, 7 this time saved in the operating room has the potential to be more than $3000 per case for each hour saved.
Finally, our overall experience has demonstrated the safety and efficacy of this procedure, as well as an extremely low complication rate in the past. 2 It has been shown that when robotics can keep the leak rate of the RARYGB operation below 3%, it is cost-effective. 8 In this series, the console surgeon performed 168 RARYGBs and had a leak rate of 1.2% and a mortality of 0% within 66 cases and a 0% leak rate over the next 102 cases. The limitation of these data is, of course, that prospective comparisons cannot be made from this retrospective review; however, one can glean from these results and those previously published5,9 that robotics has a good safety record in the field of bariatric surgery and may reduce the overall cost of these operations by lowering morbidity.
Just as with any new technology that comes to market, appropriate use with adequate training is required for efficiency. Because new technological advancements, such as the introduction of the da Vinci Xi™ platform and robotic stapling devices, will lend themselves to further optimization of surgical technique and increased efficiency, we recommend this technique as the foundation from which these improved processes are founded.
Conclusions
There are many variations that may be made, dependent on surgeon preference. The combination of this approach, our experience with the da Vinci robot platform, and well-trained ancillary staff provides for an efficient and effective use of operating room time and improved patient outcomes. The fact that robotics seems to have a shorter learning curve at reducing the operative and room times for the gastric bypass operation for young surgeons just starting their bariatric career is surely due, at least in part, to the inherent efficiency of the technique described above and the economy of motion that is enhanced by the robotic platform. Nonetheless, articles like this one, which describes the technique, aim to advance this efficiency such that operative time could be much faster in the future.
We describe a totally RARYGB technique above that is as safe, cost-effective, and time-efficient as the hybrid and purely laparoscopic approaches. In fact, as the technology evolves, it is very possible that the RARYGB will become more effective with regard to these three variables compared with LRYGBs. Large prospective databases being collected at present will soon give us better answers than rather simple retrospective reviews like this one; nonetheless, these authors are convinced that robotics has a very bright future in bariatric surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.