
Abstract
Abstract
Introduction:
The aim of this meta-analysis was to determine whether laparoscopic splenectomy (LS) and LS with esophagogastric devascularization (LSED) were the minimally invasive alternative for portal hypertension.
Materials and Methods:
A meta-analysis of comparative clinical trials was performed to assess our questions noted above. The databases PubMed, ScienceDirect, and Springerlink were searched.
Results:
In total, 725 patients with liver cirrhosis and/or portal hypertension from eight published comparative trials were included. The operation time in the laparoscopic group was more than that in the open group [weighted mean difference (WMD) 35.24 (16.74, 53.74); P<.001]. However, there were less intraoperative blood loss [WMD −194.84 (−321.34, −68.34); P=.003] and a shorter postoperative hospital stay [WMD −4.33 (−5.30, −3.36); P<.001] in the laparoscopic group. The incidence of complications was similar in the two groups. In the subgroup studies about LS versus open splenectomy, no significant differences were found in operation time, intraoperative blood loss, and complication rates. The postoperative hospital stay in the LS group was apparently decreased [WMD −4.07 (−4.93, −3.21); P<.001]. Although the operation time of LSED was longer [WMD 43.23 (17.13, 69.32); P=.001], LSED was associated with less intraoperative blood loss [WMD −189.26 (−295.71, −82.81); P<.001] and a shorter postoperative hospital stay [WMD −5.41 (−7.84, −2.98); P<.001]. Meta-analysis did not favor either LSED or open splenectomy with esophagogastric devascularization in term of complication rates.
Conclusions:
The results of this meta-analysis were in favor of LS and LSED for being a safe, minimally invasion alternative for patients with liver cirrhosis and portal hypertension.
Introduction
L
Splenectomy has been always considered as the effective surgical therapy for liver cirrhosis and portal hypertension.5,6 Splenectomy could not only cure hypersplenism and consequently abolish bleeding tendency due to thrombocytopenia, but also prevent bleeding from esophagogastric varices successfully via reducing pressure of the portocaval system and ligating dilated vessels, such as short gastric veins, partially around the esophagus and stomach.7,8 On the other hand, liver function is also improved after splenectomy, owing to the supply of more blood and growth factors to the liver from the portal vein. 9 Splenectomy was also found to improve portal hypertensive gastropathy. 10 Open splenectomy (OS) and esophagogastric devascularization (ED) have been confirmed to manage hypersplenism and bleeding from esophagogastric varices synchronously with a low incidence of hepatic encephalopathy and was recommended in China as the first choice for the treatment of portal hypertension more than 10 years ago, especially for liver cirrhosis due to chronic viral hepatitis infection. 7
Since laparoscopic splenectomy (LS) was introduced by Delaitre and Maignien 11 in 1991, it has been considered as the standard alternative for most indications, including idiopathic thrombocytopenic purpura, hereditary spherocytosis, thalassemia, and other hematologic diseases with normal-sized spleen for splenectomy worldwide.12–15 Because of the limited operation space caused by splenomegaly and the high bleeding propensity of varicose veins around both the esophagus and stomach, liver cirrhosis and portal hypertension have long been regarded as the contraindication for LS.16–18 As a result of advances in laparoscopic equipment devices and skills, LS and LS with ED (LSED) have recently been performed increasingly on patients with liver cirrhosis and portal hypertension. Several articles have been published on LS or LSED for liver cirrhosis and portal hypertension.19–21 In this study, we reviewed the current literature and carried out a meta-analysis to evaluate differences in operation time, intraoperative blood loss, risks of major complication, and postoperative hospital stay between LS (LSED) and OS (OS with ED [OSED]).
Materials and Methods
All aspects of the Cochrane Handbook for Interventional Systematic Reviews were followed, and the study was written according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 22
Literature search strategy
The primary sources of the reviewed studies without restriction on both regions and date were PubMed, Springerlink, and ScienceDirect (Elsevier). Only articles written in English were incorporated into this meta-analysis. We combined the following database-specific search terms: “laparoscopic splenectomy,” “laparoscopic devascularization,” “liver cirrhosis,” and “portal hypertension.” Study abstracts were reviewed, and full-text article on pertinent subjects were obtained. The computer search was supplemented with manual searches for reference lists of all retrieved review articles, original clinical studies, and abstracts from meetings to search other comparative clinical studies not found in the computer search. When the same group published more than one relevant research articles, only the most recent and complete data were included.
Study selection
Clinical trials were evaluated for inclusion or exclusion by two independent researchers (X.Z. and Xiaohong Gai) for the relevance to the subject. Two supervisors (Q.L. and Y.Y.) conducted the random check. We performed study selection through three phases of study screening. The eligibility of potential titles and abstracts was considered by two independent investigators (X.Z. and X.G.), and the chosen full-text articles were obtained. Then, full-text articles were reviewed and evaluated for the meta-analysis.
The inclusion criterion required that clinical trials described the perioperative data of both LS (LSED) and OS (OSED) performed for patients with liver cirrhosis and portal hypertension including operation time, intraoperative blood loss, and incidences of complication after surgery.
The exclusion criteria included review, letter, editorial, case reports, and research articles investigating nonhumans, infants, and adolescents. Any discrepancies in inclusion or exclusion of clinical trials were resolved by mutual discussion.
Data extraction and quality assessment
Data from the selected clinical trials were extracted by two researchers (X.Z. and Q.L.), and the discrepancies were resolved by discussion between them with supervision of the third researcher (Q.L.). The quality of the nonrandomized studies was evaluated by using the Newcastle–Ottawa Scale with some modifications to match the needs of this study. The quality of the studies was assessed by evaluating three items: patient selection, comparability of LS and OS groups or LSED and OSED groups, and assessment of perioperative clinical data, including operation time, intraoperative blood loss, incidence of major complication after surgery, and postoperative hospital stay (Table 1). All studies recruited here were graded on an ordinal star scoring scale, with higher scores representing studies of higher quality. A study can be assigned a maximum of one star for each numbered item within the selection category, and a maximum of four stars can be given for the comparability of the two groups.
Comparability variables: a=age; b=gender; c=etiology of liver cirrhosis and portal hypertension; d=liver function (Child–Pugh Classification); e=bleeding from esophagogastric varices; f=spleen size.
Statistical analysis
All analysis was carried out using Review Manager software version 5.2 (Cochrane Collaboration, Nordic Cochrane Center, Copenhagen, Denmark). For continuous data, including operation time, intraoperative blood loss, and postoperative hospital stay, weighted mean differences (WMDs) were calculated to allow overall comparisons to be made in consideration of individual study size and mean with standard deviation (SD) as described in the individual trials. When the values of mean and SD were not reported, they were estimated crudely from median values and ranges according to the protocol introduced by Hozo et al. 23 For the dichotomous data involved in each trial, such as incidence of major complication after surgery, we assessed them using random-effect models because there were some small differences on the detailed operation techniques existing in the selected trials. The odds ratio (OR) and 95% confidence interval (CI) were obtained using the Mantel–Haenszel method. Heterogeneity of parameters between studies was tested using Q and I 2 statistics. If there was significant heterogeneity (P<.1 or I 2 >50%), a random-effect model was used to calculate the summary estimates and 95% CI. Overall results were measured using the Z test. A funnel plot was constructed to assess publication biases for each outcome. All tests were two-sided, and a P value of <.05 was considered as statistically significant.
Results
After the initial search, 390 relevant articles were obtained by searching through the databases, and 3 additional articles were identified via other resources. Of the 390 articles, 9 articles were identified in which the comparative study of LS versus OS or LSED versus OSED in liver cirrhosis and portal hypertension was performed and detailed perioperative data were described. Eight articles were cohort studies. One publication 20 from our group was excluded because it was the first report about LSED versus OSED for portal hypertension, and all of its data were covered completely by another article published later from our group. 24 The PRISMA study flow diagram for the systemic reviews was described in Figure 1. The meta-analysis was conducted using the eight articles noted above; the characteristics of these clinical trials are shown in Table 2. The data on operation time, intraoperative blood loss, risks of major complication, and postoperative hospital stay are presented in Table 2. The quality assessment and scores are summarized in Tables 1 and 3.

PRISMA study flow diagram.
LS, laparoscopic splenectomy; LSED, laparoscopic splenectomy with esophagogastric devascularization; NA, the relevant data are not described in the article; OS, open splenectomy; OSED, open splenectomy with esophagogastric devascularization.
Operation time
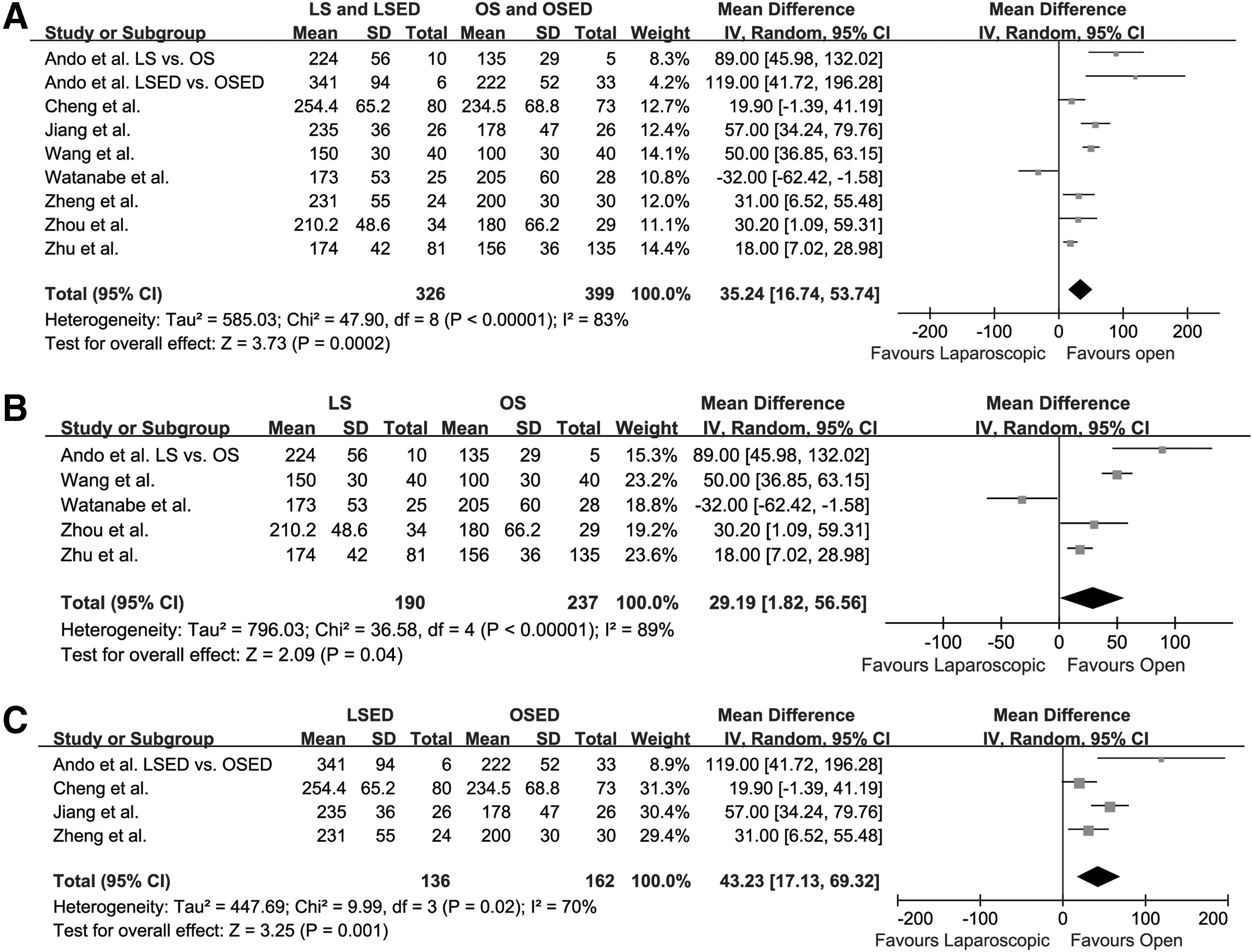
All eight trials describing data of operation time were included for meta-analysis, with a total of 725 patients. The mean operation time in the laparoscopic group (LS and LSED) (range, 150–341 minutes; median, 224 minutes) was significantly longer than that in the open group (OS and OSED) (range, 135–234.5 minutes; median, 180 minutes) [WMD 35.24 (16.74, 53.74); Z=3.73; P<.001] (Fig. 2A). The funnel plot is shown in Supplementary Figure S1 (Supplementary Data are available online at www.liebertpub.com/lap). Individually, there were five studies comparing operation time between LS and OS for liver cirrhosis and portal hypertension, with a total of 427 patients. Meta-analysis found that the mean operation time was longer in the LS group (range, 150–224 minutes; median, 174 minutes) than that in the OS group (range, 100–205 minutes; median, 156 minutes) [WMD 29.19 (1.82, 56.56); Z=2.09; P=.04] (Fig. 2B). The funnel plot is shown in Supplementary Figure S2. In order to compare operation time between LSED and OSED, 298 patients from four studies was used in the meta-analysis, which showed that the LSED group (range, 231–341 minutes; median, 235 minutes) had an apparently longer mean operation time than the OSED group (range, 178–234.5 minutes; median, 200 minutes) [WMD 43.23 (17.13, 69.32); Z=3.25; P=.001] (Fig. 2C). The funnel plot is shown in Supplementary Figure S3.
Intraoperative blood loss
Intraoperative blood loss was described in all eight trials, with a total of 725 patients. After meta-analysis, the mean intraoperative blood loss in the LS and LSED group (range, 129.1–531 mL; median, 191.2 mL) was significantly lower than that in the OS and OSED group (range, 100–778 mL; median, 415.5 mL) [WMD −194.84 (−321.34, −68.34); Z=3.02; P=.003] (Fig. 3A). The funnel plot is shown in Supplementary Figure S4.
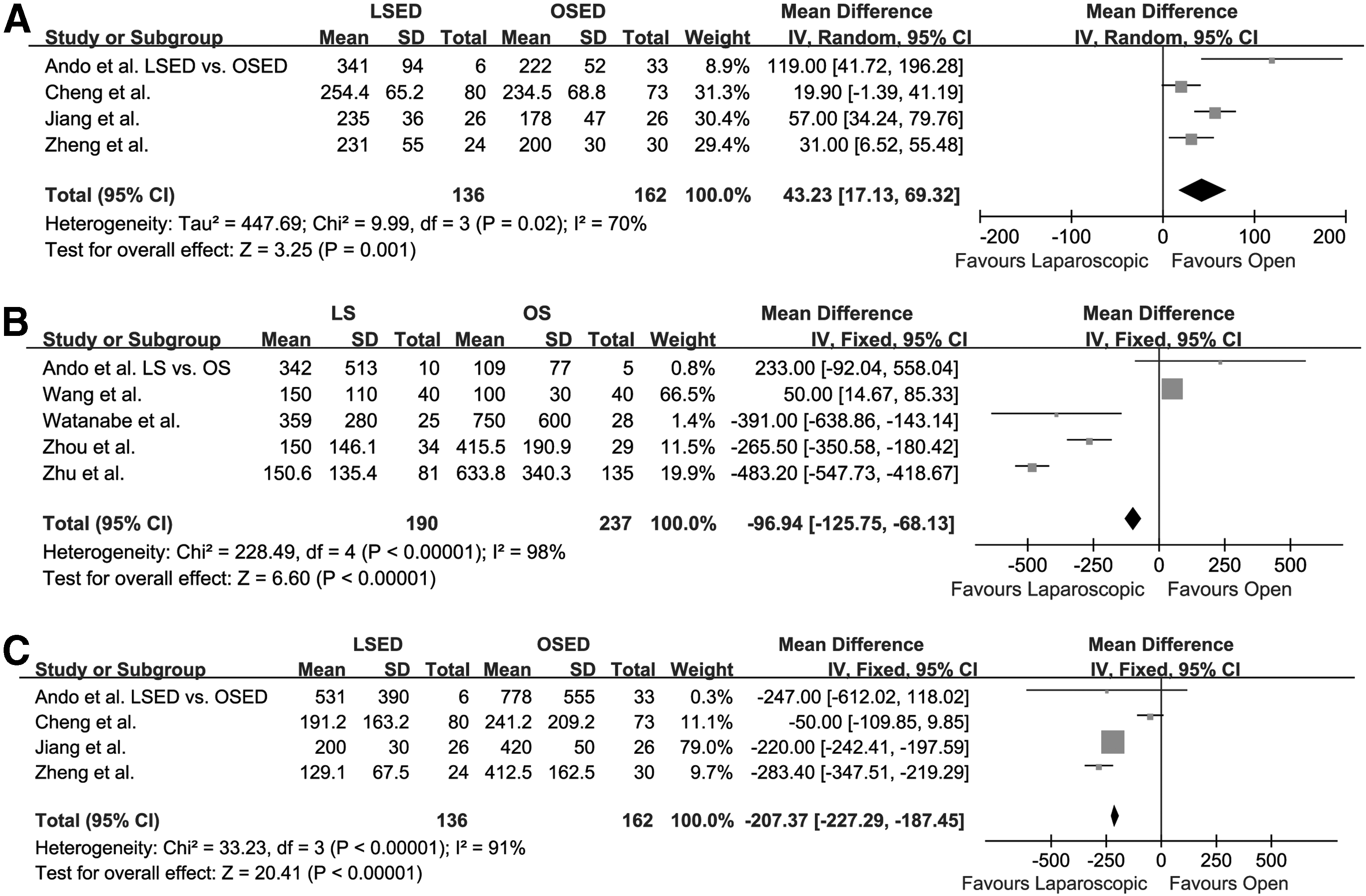
With a total of 427 patients from five articles, the intraoperative blood loss between LS and OS was calculated by meta-analysis. There was no difference found in mean intraoperative blood loss between the LS group (range, 150–359 mL; median, 150.6 mL) and OS group (range, 100–750 mL; median, 415.5 mL) [WMD −183.10 (−466.26, 100.06); Z=1.27; P=0.21] (Fig. 3B). The funnel plot is shown in Supplementary Figure S5.
There were four studies showing the data of intraoperative blood loss of both LSED and OSED, with a total of 298 patients. After meta-analysis, a significantly less mean intraoperative blood loss was found in the LSED group (range, 191.2–531 mL; median, 129.1 mL) compared with the OSED group (range, 241.2–778 mL; median, 412.5 mL) [WMD −189.26 (−295.71, −82.81); Z=3.48; P<.001] (Fig. 3C). The funnel plot is shown in Supplementary Figure S6.
Incidence of major complication after surgery
The incidence of major complication after surgery was presented in eight studies, with a total of 725 patients. The meta-analysis revealed that incidence of complications in the LS and LSED group was similar to that in the OS and OSED group [OR=0.74 (0.52, 1.06); Z=1.63; P=.100] (Fig. 4A). The funnel plot is shown in Supplementary Figure S7.

There were five studies providing complication risks of both LS and OS with a total of 427 patients. Similarly, no difference was detected in risks of complication between the LS and OS groups [OR 0.88 (0.56, 1.37); Z=0.56; P=.57] (Fig. 4B). The funnel plot is shown in Supplementary Figure S8. Additionally, after analyzing 298 cases from four studies, we did not find any significant difference of complication incidence between LSED and OSED [OR=0.55 (0.30, 1.00); Z=1.95; P=.05] (Fig. 4C). The funnel plot is shown in Supplementary Figure S9.
Postoperative hospital stay
To determine whether LS or LSED could reduce the length of postoperative hospital stay, we examined a total of six studies including 618 patients with liver cirrhosis and portal hypertension. The meta-analysis showed that mean postoperative hospital stay in the LS and LSED group (range, 6.1–19.8 days; median, 8.2 days) was dramatically less than that in the OS and OSED group (range, 10.1–35.6 days; median, 11.9 days) [WMD −4.33 (−5.30, −3.36); Z=8.79; P<.001] (Fig. 5A). The funnel plot is shown in Supplementary Figure S10.
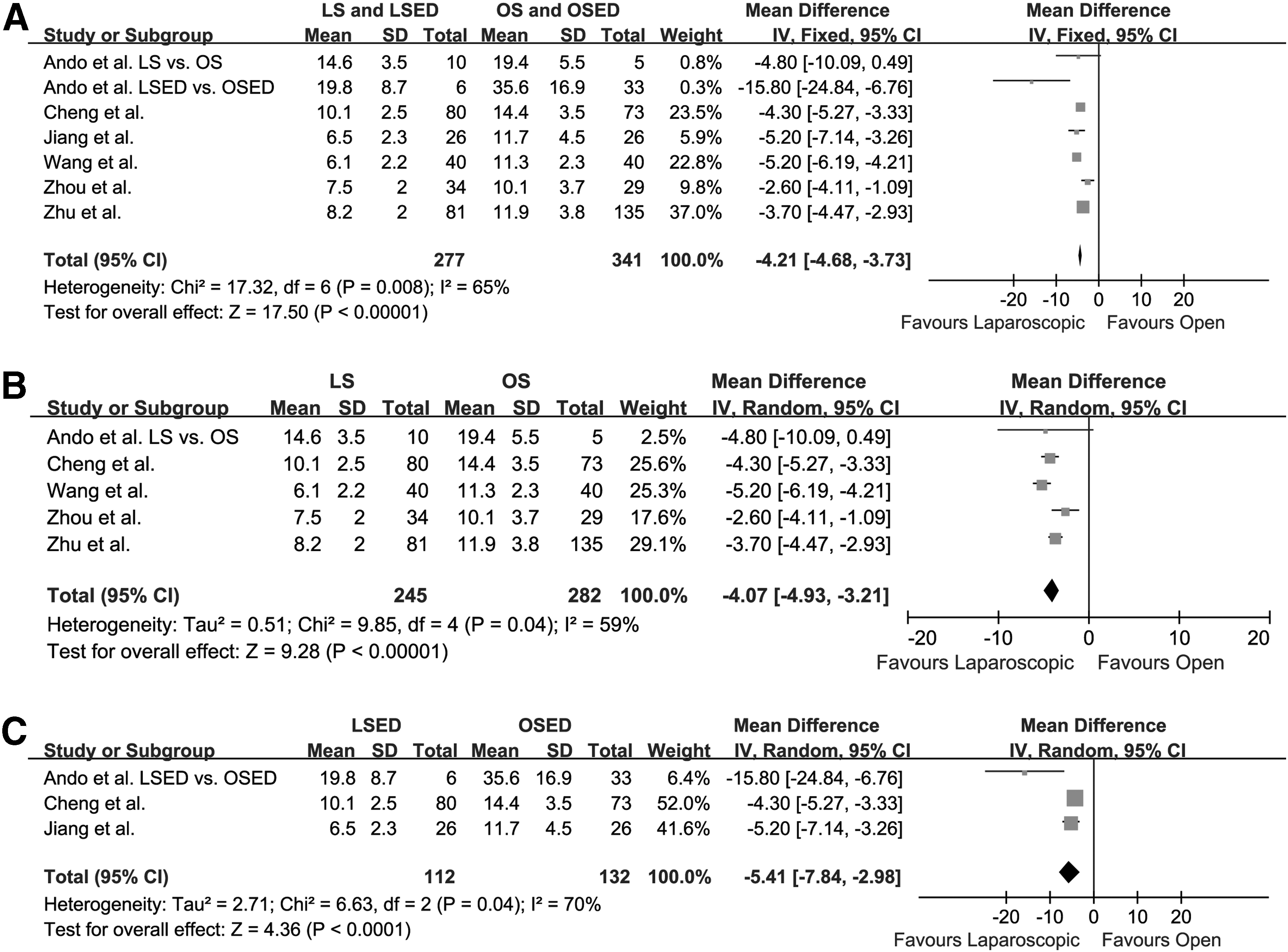
In the investigation of subgroups, there were five studies including 527 cases giving data about postoperative hospital stay of both LS and OS groups. After meta-analysis, the mean postoperative hospital stay in the LS group (range, 6.1–19.8 days; median, 8.2 days) was also significantly decreased compared with the OS group (range, 10.1–19.4 days; median, 11.9 days) [WMD −4.07 (−4.93, −3.21); Z=9.28; P<.001] (Fig. 5B). The funnel plot is shown in Supplementary Figure S11.
We also investigated three studies showing postoperative hospital stay of both LSED and OSED groups by meta-analysis and found that the LSED group (range, 6.5–19.8 days; median, 10.1 days) had a significantly mean shorter postoperative hospital stay than the OSED group (range, 11.7–35.6 days; median, 14.4 days) consistently [WMD −5.41 (−7.84, −2.98); Z=4.36; P<0.001] (Fig. 5C). The funnel plot is shown in Supplementary Figure S12.
Discussion
Owing to poor liver function and dysfunction of coagulation secondary to thrombocytopenia, patients with liver cirrhosis and portal hypertension have an unsatisfied tolerance for operation. Thereby, although traditional OS and OSED have a definite effect on reversing hypersplenism and preventing bleeding from esophagogastric varices, there is an urgent need to find an efficacious and minimally invasive alternative. In Western countries such as the United States, conservative therapies have been considered as the preferred option to stop or prevent bleeding from esophagogastric varices, including transjugular intrahepatic portosystemic shunt, endoscopic sclerotherapy and banding, and β-blocker treatment. 25 However, owing to the unfortunate long-term results, both endoscopic sclerotherapy/banding and β-blocker treatment are not recommended to manage refractory esophagogastric variceal bleeding. Additionally, there is high risk of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. The minimally invasive operation, which not only controls bleeding effectively but also reverses hypersplenism with limited impairment of liver function, still plays an important role in the treatment of liver cirrhosis and portal hypertension.
Despite the fact that LS has gained popularity as the standard procedure for hematologic diseases and spleen tumor with the normal-sized spleen, it remains controversial16,17,20 to perform LS or LSED on patients with liver cirrhosis and portal hypertension because of the lack of working space, bleeding tendency secondary to thrombocytopenia, and potential massive bleeding owing to damaged, dilated veins or the splenic capsule. With the application of color Doppler flow imaging and multi–detector-row computed tomography, surgeons can obtain information about spleen size and dilated vessels around esophagus and stomach easily before surgery, which is very helpful to select suitable patients and avoid converting the procedure to an open operation. In addition, satisfactory intraoperative hemostasis can be achieved with the help of Harmonic® shears (Ethicon Endo-Surgery, Cincinnati, OH), the LigaSure™ vessel sealing system (Covidien, Mansfield, MA), and a vascular stapler. With these advancements of medical equipments and therapy strategy, it is feasible and safe to perform LS and LSED for liver cirrhosis and portal hypertension, which has been confirmed by a growing body of clinical studies.20,21,26–28
Meta-analysis has verified that LS for hematologic diseases is associated with longer operation time, shorter hospital stay, and lower complication risk compared with OS.29,30 In this investigation, we searched for clinical comparative studies of LS and LSED versus OS and OSED for liver cirrhosis and portal hypertension in three databases (PubMed, Springerlink, and ScienceDirect). No randomized controlled trials were found, and eight retrospective cohort studies were used in the meta-analysis according to the inclusion criterion. After meta-analysis, it was found that operation time in the LS and LSED group was significantly longer than that in the OS and OSED group. Consistently, in the subgroup study, it was found that the LS group had a longer operation time than the OS group, and operation time in the LSED group was longer than that in the OSED group. There are three potential reasons for longer operation time in the laparoscopic group: (1) it takes more time to conduct finer manipulation during laparoscopic operation in order to prevent intraoperative bleeding; (2) limited surgery space affects the speed of manipulation apparently; and (3) there is a technical challenge to put the enlarged spleen or massive spleen into the retrieval bag and extract it through the trocar port site. However, based on the investigation about operation time of LS, the difference of operative time between the laparoscopic group and the open group may continue to decline as improvements occur in both experience and technology.
In this study, the laparoscopic group was found to be correlated with less intraoperative blood loss. Although there was no difference of intraoperative blood loss between the LS and OS groups, the LSED group had significantly less intraoperative blood loss than the OSED group. This could be caused by two possible reasons: (1) more attention is paid to prevent bleeding during laparoscopic procedures because severe (and perhaps even moderate) bleeding results in serious interference with the operation sight and consequently causes conversion to an open operation; and (2) both better operation sight and a more spacious surgery field are obtained in LSED when conducting ED, which helps surgeons to ligate the dilated vessels and disconnect them effectively.
The present meta-analysis revealed that the incidence of complications in the LS and LSED group was similar to that in the OS and OSED group. The same results were obtained in the comparison of complication rates between LS and OS. However, despite that no significant differences were found, there seemed to be an overall trend in favor of LSED. Based on the previous data, LS was supposed to be related to a lower rate of postoperative complication than OS, and the lower rate of pulmonary complications was the biggest part of the reduction in complication rates after LS. 29 However, portal or splenic vein thrombosis has recently been identified as a common disorder after LS, 31 and the previous comparative clinical study revealed that there was a significantly higher incidence of portal or splenic vein thrombosis after LS than after OS. 32 Thus, although total complication rates were similar, there were more portal or splenic vein thromboses and fewer pulmonary complications in LS and LSED. On the other hand, anticoagulant therapy is important for patients receiving LS and LSED following early detection by computed tomography with contrast.
It is not surprising that a shorter postoperative hospital stay was found in the LS and LSED group compared with the OS and OSED group. Similar results were observed in the subgroup comparative studies of both LS versus OS and LSED versus OSED. The potential facts that curtail postoperative hospital stay for LS and LSED patients could include smaller surgical incision, less postoperative pain, earlier recovery of gastrointestinal function, and fewer pulmonary complications.
Limitations
Although this meta-analysis strongly indicated that LS and LSED had the advantage of minimal invasion compared with OS and OSED, studies of this nature are limited inherently by the variability in study design and reporting among different clinical trials. Differences of surgical procedures existing in the eight clinical studies included in this meta-analysis could impact the final results. Additionally, there has been no randomized control trial published about comparison of LS (LSED) and OS (OSED) for liver cirrhosis or portal hypertension, which negatively affects the credibility of the results we obtained here in part.
Conclusions
LS for hematological disorders has been verified to have remarkable benefits of minimal invasiveness compared with conventional options by meta-analysis, which showed that LS was associated with fewer postsurgical complications, less intraoperative blood loss, shorter hospital stay, and longer operative time. The same advantages of minimal invasion were found in LS and/or LSED for liver cirrhosis and portal hypertension by this meta-analysis for the first time. This is the first step in giving a definite answer as to which procedure might be the more ideal procedure for managing bleeding from esophagogastric varices and hypersplenism secondary to liver cirrhosis and portal hypertension. However, in order to determine the true value of LS or LSED in the treatment of liver cirrhosis and portal hypertension, a large randomized controlled trial is strongly recommended.
Footnotes
Acknowledgments
This study was supported by grants from the National Natural Scientific Foundation of China (numbers 81272645 and 81072052 to Q.L. and 81301743 to X.Z.) and the Research Fund for the doctoral Program of High Education of China from the Ministry of Education (number 20120201120090 to X.Z.).
Disclosure Statement
No competing financial interests exist.
X.Z., C.D., Y.Y., and Q.L. conceived and designed the experiments. X.Z. and C.D. performed the experiments. X.Z. wrote the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.