
Abstract
Abstract
Aims:
To explore the feasibility of sleeve gastrectomy (SG) as a treatment for polycystic ovary syndrome (PCOS) and its potential to improve clinical efficacy in PCOS patients with symptoms of oligomenorrhea.
Patients and Methods:
Twenty-four obese patients with PCOS underwent laparoscopic SG. Simultaneously, 24 obese patients with PCOS received lifestyle modification therapy (LMT). Follow-ups were conducted at 3–6 months. Weight loss, menstruation, and improvements in hirsutism and metabolic symptoms were compared.
Results:
In the SG group, 20 patients were restored to normal menstrual cycles and ovulation at 3–6 months after surgery. Their average androgen levels decreased significantly following surgery (P=.012). Conversely, only 6 patients in the LMT group were restored to normal menstrual cycles and ovulation after receiving 3 months of treatment. Their average preoperative and postoperative androgen levels showed a nonstatistically significant decrease (P>.05). Compared with the LMT group, the SG group showed more pronounced improvements in menstruation. Additionally, body mass and body mass index were significantly reduced in patients in the SG group 3 months after the surgeries, with maximum weight loss observed at approximately 6 months after surgery. Patients who received LMT showed a gradual weight reduction such that body mass decreased significantly after 3 months (P<. 001). Compared with patients in the LMT group, patients in the SG group showed greater weight loss results (P<.0001).
Conclusions:
In patients with PCOS, SG resulted in more marked weight loss and better improvements in clinical symptoms compared with LMT.
Introduction
P
Weight loss is the first-line treatment for controlling PCOS symptoms. Studies have shown that abdominal obesity and weight gain in adulthood promote the development of PCOS. However, as long as normal body weight is maintained, 30%–40% of PCOS cases can be prevented effectively. 8 Gynecological medications alone are ineffective in treating PCOS-related obesity 9 ; however, weight loss surgeries applied as potential treatments for PCOS have provided promising clinical results.10,11
Bariatric procedures in widespread use include the Roux-en-Y gastric bypass, sleeve gastrectomy (SG), and laparoscopic adjustable gastric banding. Among them, SG has been recently reported to effectively improve the metabolic, behavioral, and reproductive outcomes in an obese rat model of PCOS.12,13 Due to the paucity of studies regarding the feasibility of these different bariatric procedures as treatments for PCOS and their potential to improve clinical efficacy in patients with PCOS with symptoms of oligomenorrhea in particular, the aim of the current study assessed outcomes for patients with PCOS after SG surgery compared with treatment with conventional lifestyle modification therapy (LMT).
Patients and Methods
Patients
Between April 2010 and May 2014, 24 obese (average weight, 99.8 kg [range, 86–140 kg]) patients with PCOS received SG for PCOS and obesity. During the same period, an additional 24 obese (average weight, 89.7 kg [range, 74–120 kg]) patients with PCOS chose to undergo LMT due to concerns regarding perceived risks of surgery to treat their conditions. All patients sought medical attention in our hospital mainly due to obesity and oligomenorrhea. Among the 48 cases, 29 had hyperandrogenism, 23 had luteinizing hormone/follicle-stimulating hormone level ratios of >2, and 31 had polycystic ovary detected by B-mode ultrasound (Table 1). All patients signed an informed consent before receiving treatments. The study was approved (ethical approval code EASTH1003151SH) by the research committee and the institutional review board of East Hospital of Tongji University (Shanghai, China).
LH/FSH, luteinizing hormone/follicle-stimulating hormone; PCOS, polycystic ovary syndrome.
Laparoscopic SG
Surgery was performed using laparoscopy. The procedures began with patients in the supine position, with a head elevation angle of 20–30° and legs separated by 60° and fixed. Two 5-mm trocars were placed in the left subcostal midclavicular line and xiphoid process, respectively, for auxiliary operation. Additionally, 10-mm and 12-mm trocars were placed at the umbilicus and upper right side of the umbilicus, respectively, to introduce a 30° laparoscope lens and a linear cutting stapler, respectively. An ultrasonic dissector was used to separate the omentum along the gastric wall starting from the middle of the greater curvature of the stomach to the angle of His. The fundus and upper body of the stomach were fully separated, followed by separation along the greater curvature of the stomach until a position 5–6 cm above the pylorus was reached. A 32-French probe was inserted through the mouth until it reached the distal gastric antrum (Fig. 1A). A linear cutter stapler (60 mm) was used for continuous incisions and sutures starting from 5–6 cm above the pylorus until reaching the angle of His. The fundus and most of the gastric body were resected, accounting for approximately 65%–70% of the whole stomach (Fig. 1B). If small amounts of anastomotic stoma bleeding were observed, a small piece of gauze was used to stop bleeding by compression. If significant amounts of bleeding were observed, 3-0 absorbable sutures and the “figure-of-8” suture technique were used for hemostasis. The resected stomach specimen was removed through the 10-mm hole at the umbilicus.
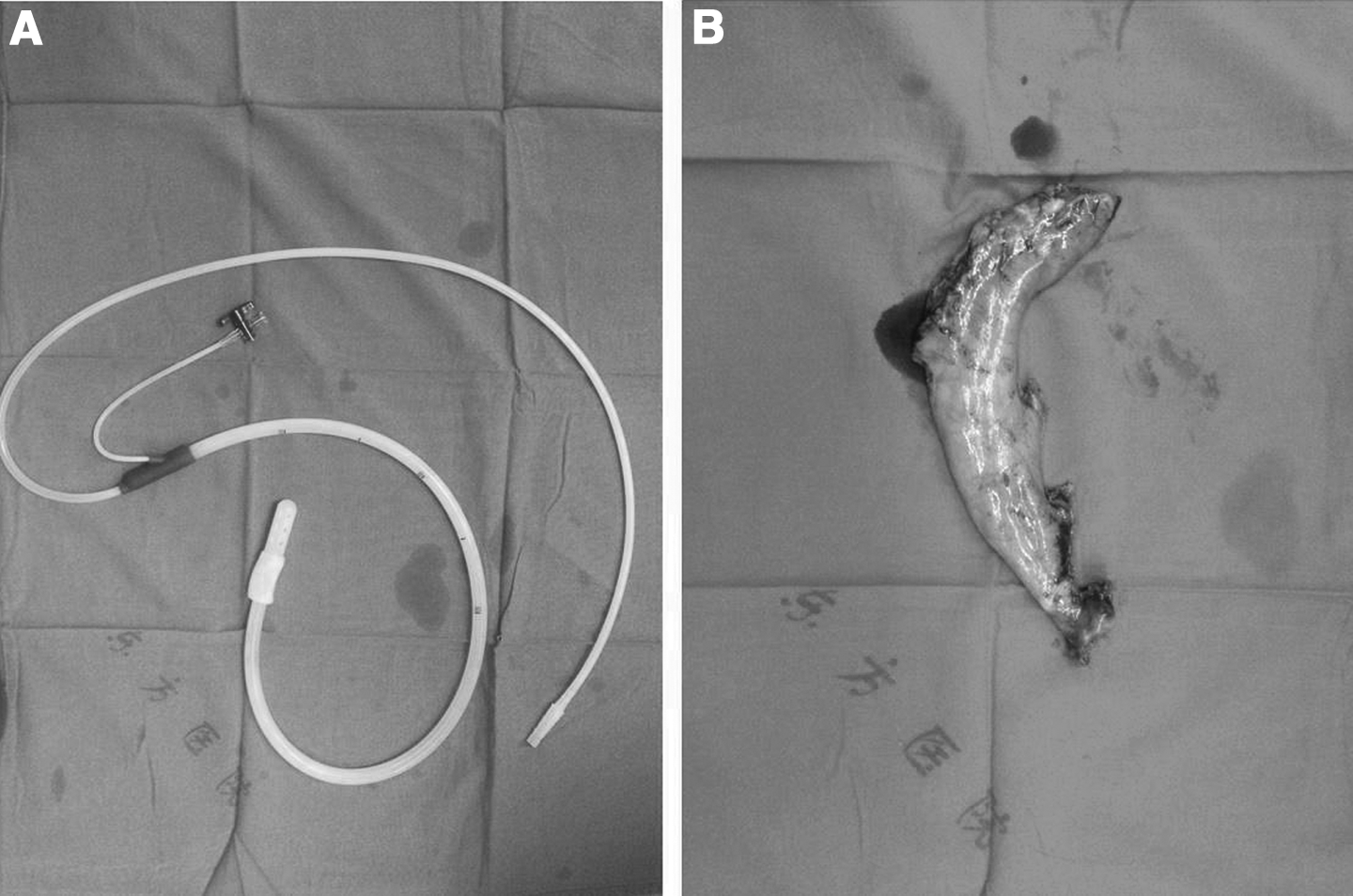
Laparoscopic sleeve gastrectomy.
LMT
The LMT includes dietary, exercise, and behavioral therapies. The dietary therapy mainly uses low-calorie diet, which combined nutrients in different categories based on the ratio of carbohydrate, protein, and lipid. Exercise therapy is to decompose triglyceride stored in the adipose tissues through exercise, which allows the body to balance energy intake and usage, resulting in fat reduction and weight control. The main method was allowing obese PCOS patients to exercise for at least 150 minutes weekly, of which 90 minutes were for aerobic exercises (at least two-thirds of the total muscles in the body were involved, including jogging, aerobics, swimming, and cycling). The exercise intensity levels reached medium or high levels (the evaluation standards were based on the heart rates during exercise). The heart rates for medium- and high-intensity levels were 125–150 beats per minute and over 150 beats per minute, respectively. The duration of exercise therapy was at least 3 months. Behavior therapy required assistance from psychiatrists and family members to address patient mental status and lifestyle, as well as to facilitate adherence to physician instructions pertaining to weight loss goals.
Patient monitoring
Patients fasted routinely for 3 days after the operation and were provided with proper hydration. Breathing, heart rate, position of the nasal gastric tube, amount of drainage from the peritoneal drainage catheter, and the morphology of the drainage were monitored. On confirmation of postoperative anastomotic stoma bleeding or leakage, a timely re-operation was performed. Because gastric leakage is one of the most serious complications of SG, perioperative practices were focused on monitoring patients and gauging their responses. Patients who were morbidly obese or had preoperative tracheal stenosis could receive intensive care unit transitional care after surgery.
The monitored perioperative diet consisted of a liquid diet during the first week after surgery and avoidance of excess food intake. Patients were allowed to ingest solid food during the second week after surgery. In our hospital, the amount of solid food increased generally during the third week after surgery, and normal diet was given at the fourth week after surgery. Patients were provided with instructions on how to form correct eating habits when discharged, which included avoidance of overeating, eating three meals a day, chewing and swallowing food slowly, allowing 20–30 minutes for each meal, eating a diet of protein-rich food while avoiding high-caloric intake, supplementing with vitamins and minerals if needed, drinking sufficient amounts of liquid, and avoiding carbonated drinks and alcohol.
Surgery patients were reviewed regularly at the metabolic and bariatric surgery and gynecology clinics after discharge. All patients received follow-ups at 1, 3, 6, and 12 months after treatment. Changes in body weight, body mass index, PCOS-associated hirsutism, and menstrual conditions were recorded. Hirsutism was evaluated using the Ferriman–Gallwey scoring system conducted by a physician before surgery and during follow-ups. Hirsutism was defined with an Ferriman–Gallwey score of >5. Additionally, gynecological B-mode ultrasound was performed in order to detect new complications and to assess whether existing complications had been alleviated.
Statistical analysis
SPSS 20.0 statistical software (IBM Corp., Armonk, NY) was used for data analysis. Paired t tests were used to compare parameters before and after surgery.
Results
The SG laparoscopic surgery is a more executable procedure
All 24 cases of SG laparoscopic surgery were completed successfully and without a switch to laparotomy. The operative time was 72±18 minutes, and the time to the first postoperative flatus was 20±10 hours. The nasogastric tube was removed after the first flatus, and a small amount of water and liquid food was provided. All postoperative recoveries were successful, and the average postoperative hospital stay was 5.5±1 days. Some obese patients in the LMT group experienced mobility difficulties and impaired exercise tolerance, and 5 withdrew from the study because they could not follow the standard instruction to complete the treatment.
The SG laparoscopic surgery restored normal menstrual cycles and ovulation
All patients were asked to receive follow-up examinations at our hospital or a local hospital 3–6 months after surgery. The majority of patients in the SG group (20/24) exhibited restored normal menstrual cycles and ovulation during the 3–6 month follow-up period (Table 2). In the SG group, androgen levels decreased significantly from 0.562±0.07 ng/mL preoperatively to 0.31±0.1 ng/mL postoperatively (P=.012). Among the 24 patients who received LMT, 3 months after treatment, 6 patients (6/24) had restored normal menstrual cycle and ovulation. The LMT average androgen levels showed a nonsignificant decrease from 0.513±0.12 ng/mL preoperatively to 0.504±0.09 ng/mL postoperatively (P>.05). Therefore, more pronounced improvement in menstruation was observed in the SG group than the LMT group. It should be noted that 1 of the patients who wished to become pregnant conceived successfully and that SG had a particularly significant effect on the improvement of oligomenorrhea, as 1 patient's period began before a significant weight loss was observed at 1 week after surgery. Normal menstrual cycles resumed in all patients at 3–6 months after surgery.
Data are mean±standard deviation values or number of patients, respectively.
Statistically significant differences between sleeve gastrectomy and lifestyle modification groups.
The SG laparoscopic surgery results in a higher body weight decrease with metabolic improvement
Patients in the LMT group showed a gradual decrease in body weight such that body mass decreased significantly (4.1 kg, P<.05) at 3 months of treatment compared with before treatment (Table 2). Patients who received 6 months of treatment showed a decrease in body mass of 5.7 kg (P<.05). Compared with the LMT group, the SG group displayed a more substantial weight loss result (15.7 kg, P<.0001). All patients in the SG group showed a significant decrease in body mass and body mass index 3 months after surgery (Table 3). The maximum weight loss was observed at approximately 6 months after surgery, followed by maintenance of a relative stable weight at a steady state.
BMI, body mass index; EWL, excess weight loss.
All patients in the SG group had metabolic disorders before surgery, including hyperandrogenism, hyperinsulinemia, hypertension, and hyperlipidemia, to varying degrees. Additionally, all patients exhibited symptoms of oligomenorrhea. Three patients wished to become pregnant; however, the fertility therapy was not effective in any of these women. Six months after receiving bariatric surgery, the patients conceived after undergoing in vitro fertilization treatment. In the 3 patients with PCOS who had hyperinsulinemia, average fasting insulin levels decreased from 31.3 μU/mL preoperatively to 16.7 μU/mL postoperatively. Nine patients with hypertension had restored normal blood pressure at 6 months after surgery, and 6 patients with hyperlipidemia had restored blood lipid levels at 6 months after surgery. In 3 patients with hyperglycemia, the levels of glycated hemoglobin at the 6-month follow-up decreased from 6.8% preoperatively to 5.1% postoperatively. Two patients in the LMT group had hyperglycemia; however, no significant improvement in blood sugar levels was observed after treatment. Collectively, these findings demonstrate that the SG group exhibited more obvious metabolic improvement than the LMT group.
Anastomotic stoma leakage is the most common postoperative complication of SG and often occurs at the angle of His in the junction between the stomach and esophagus. A single case experienced leakage at the angle of His after surgery, manifesting clinically as fever, tachycardia, elevated white blood cell count, and upper left abdominal pain. In addition, a computed tomography scan showed upper left abdominal effusion and inflammation, left pleural effusion, and pneumonia. This case was treated with gastric decompression and nasogastric enteral tube feeding, antibiotics to prevent abdominal infection, somatostatin to inhibit gastric acid secretion, endoscopic stent placement, and occlusion or ligation of fistula. Leakage at the angle of His was treated aggressively, and the patient was discharged. No other SG or LMT study participants showed treatment-associated complications. Follow-up examinations did not reveal any surgery-associated gastrointestinal disorders or physical discomfort.
Discussion
SG reduces the volume of the stomach by cutting it into a sleeve-like shape that allows food to pass more quickly and removes cells responsible for ghrelin secretion in the fundus, resulting in weight loss in obese patients. The technical development of minimally invasive surgery has led to increasingly safe bariatric surgical procedures. Compared with other bariatric surgical procedures, SG does not change the structure of the gut or involve artificial implants; therefore the incidence of surgical complications is low 14 and factored heavily into our decision to select SG for treating obese patients with PCOS. One short-term clinical study involving 600 patients reported that the incidence of postoperative complications for SG was relatively low. 15 In the current study, no postoperative complications were observed among 23 patients. Collectively, these data suggest that SG should be considered a safe and effective surgical procedure.
Few studies pertaining to the feasibility of bariatric surgery as a feasible treatment for PCOS have been reported. Therefore, sufficient clinical data on the effect of bariatric surgery on metabolic symptoms, fertility, and quality of life in patients with PCOS are lacking. Escobar-Morreale et al. 11 explored the effects of bariatric surgery (pancreatic bypass or laparoscopic adjustable gastric banding) as a treatment for 17 obese patients with PCOS (mean age, 30 years). In most women (12/17), menstrual function was restored, and among these, most (10/12) ovulated autonomously. The average weight loss was 41 kg after surgery. Hirsutism and androgen levels were also significantly improved. Furthermore, the homeostatic model assessment-insulin resistance value decreased by 50%. In another study, cases in which patients with PCOS and symptoms of multiple sclerosis who underwent Roux-en-Y gastric bypass surgery from 1997 to 2001 were reviewed. Postoperative follow-ups conducted for at least 2 years suggested that menstrual function was restored in all women, and hirsutism was resolved in half. The glycated hemoglobin levels in 3 patients decreased from 8.2% to 5.1%. Hyperlipidemia, hypertension, and diabetes were almost completely resolved. 10 The clinical data from the current study are in good agreement with the data generated in the aforementioned studies.
The current study did have a few limitations. First, participating patients were selected from all over the country, which increased the difficulty of conducting postoperative follow-ups and laboratory tests. In addition, the overall follow-up period was relatively short and thus limited the generalizability of the findings regarding long-term efficacy.
Although the mechanism by which bariatric surgery alleviates symptoms of PCOS is unclear, results from the current study indicated that the body weight of obese patients who underwent SG decreased significantly, with maximum weight loss observed 6 months after surgery. Most important is that normal menstrual cycles and ovulation were restored in the majority (70.8%) of surgical patients. Although slight weight loss was observed in patients with PCOS in the LMT group, serious long-term weight rebound occurred such that patients' body weight quickly rebounded to preoperative levels once treatment had ceased. Future research will focus on methods involving multidisciplinary treatments that may obtain better clinical outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.