
Abstract
Abstract
Background:
The aims of this study were to measure the learning curve for laparoscopic choledochojejunostomy (LCJ), to describe the technical tips and to report the follow-up data.
Materials and Methods:
The results of LCJ performed on 84 patients were analyzed. Patients were divided into eight groups, by surgical order. The plateau of the learning curve was defined as the period during which the operative time showed a dramatic decrease. The exact operative time was recorded using video analysis.
Results:
Compared with the first three groups, the fourth group showed a significantly shorter LCJ time. The subsequent groups showed a plateau, indicating that there were no more significant changes in the LCJ time. After the plateau of the learning curve was reached, the average LCJ time was 27.4±4.7 minutes. Six cases of postoperative bile leakage occurred, with all occurring before the plateau of the learning curve was reached. Five of the 6 cases of bile leakage had a nondilated common bile duct.
Conclusions:
Even for a surgeon experienced in laparoscopic surgery, there is a steep learning curve for the performance of LCJ. With careful video review, education of the surgical team, and various technical tips, the learning curve can be shortened. After the learning curve, experienced surgeons can perform LCJ with acceptable results.
Introduction
T
Many forms of biliary-enteric anastomosis are used in various operations, such as pancreaticoduodenectomy (PD), 2 palliative biliary bypass for unresectable periampullary cancer, Roux-en-Y choledochojejunostomy (RYCJ), or choledochoduodenostomy (CD) for recurrent choledocholithiasis,3–5 and biliary reconstruction after choledochal cyst excision.6,7 Among several types of biliary-enteric anastomosis, choledochojejunostomy (CJ) is the most commonly used method. As in open surgery, CJ is one of the most frequently used methods for laparoscopic biliary-enteric anastomosis.
Because of the technical difficulty of laparoscopic CJ (LCJ), studies evaluating LCJ are rare.8,9 In addition, to the best of our knowledge, no studies exist that have evaluated the learning curve associated with LCJ and that could assist surgeons who begin performing LCJ. The aims of this study were to measure the learning curve of LCJ, describe the technical tips acquired by the authors, and report the results and follow-up data of the patients who underwent LCJ. For these purposes, various types of hepatobiliary and pancreatic surgeries, performed by a single surgeon, were reviewed.
Materials and Methods
Patients
LCJ was performed on a total of 84 patients in two affiliated university hospitals between September 2007 and July 2014. All of the operations were performed by a single surgeon (T.H.H.). The various procedures including LCJ can be categorized into five groups, as shown in Table 1. First, laparoscopic pancreaticoduodenectomy (LPD) was performed in patients with periampullary tumors, which were preoperatively diagnosed as borderline or low-grade malignancies. Second, palliative biliary bypass surgery was performed in patients with unresectable periampullary cancer. Third, laparoscopic RYCJ (LRYCJ) was performed in patients with recurrent choledocholithiasis. Fourth, laparoscopic Roux-en-Y hepaticojejunostomy after choledochal cyst excision was performed in adult patients with choledochal cyst types I and IV; in such cases, however, the procedure should be called hepaticojejunostomy rather than CJ. Finally, 2 patients received LRYCJ. Both were transferred to our center because of a common bile duct (CBD) injury (completely resected CBD) during laparoscopic cholecystectomy at another center.
Periampullary tumors include borderline malignancies such as intraductal papillary mucinous neoplasms, neuroendocrine tumors, solid pseudopapillary tumors, and low-grade malignancies, such as ampulla of Vater cancer and unresectable periampullary carcinoma.
CBD, common bile duct.
LCJ
Position
The patient was placed in the supine position with the legs spread in a reverse Trendelenburg position. The surgeon changed places throughout the procedure. Generally, LCJ was performed with the surgeon standing to the left of the patient.
Trocar placement
Four or five trocars were used, depending on the type of procedure. In all cases, an intraumbilical incision was made, and a videoscope was introduced into the abdomen through a 10-mm umbilical trocar. When LPD was performed, the trocar placement was focused on pancreatic surgery (Fig. 1a). A 5-mm trocar was inserted at the right mammary line at the subcostal level, and a 12-mm trocar was inserted at the right midclavicular line below the umbilicus level. A 5-mm trocar was placed at the left midclavicular line at the subcostal level, and another 5-mm trocar was placed at the left mammary line at the umbilicus level.
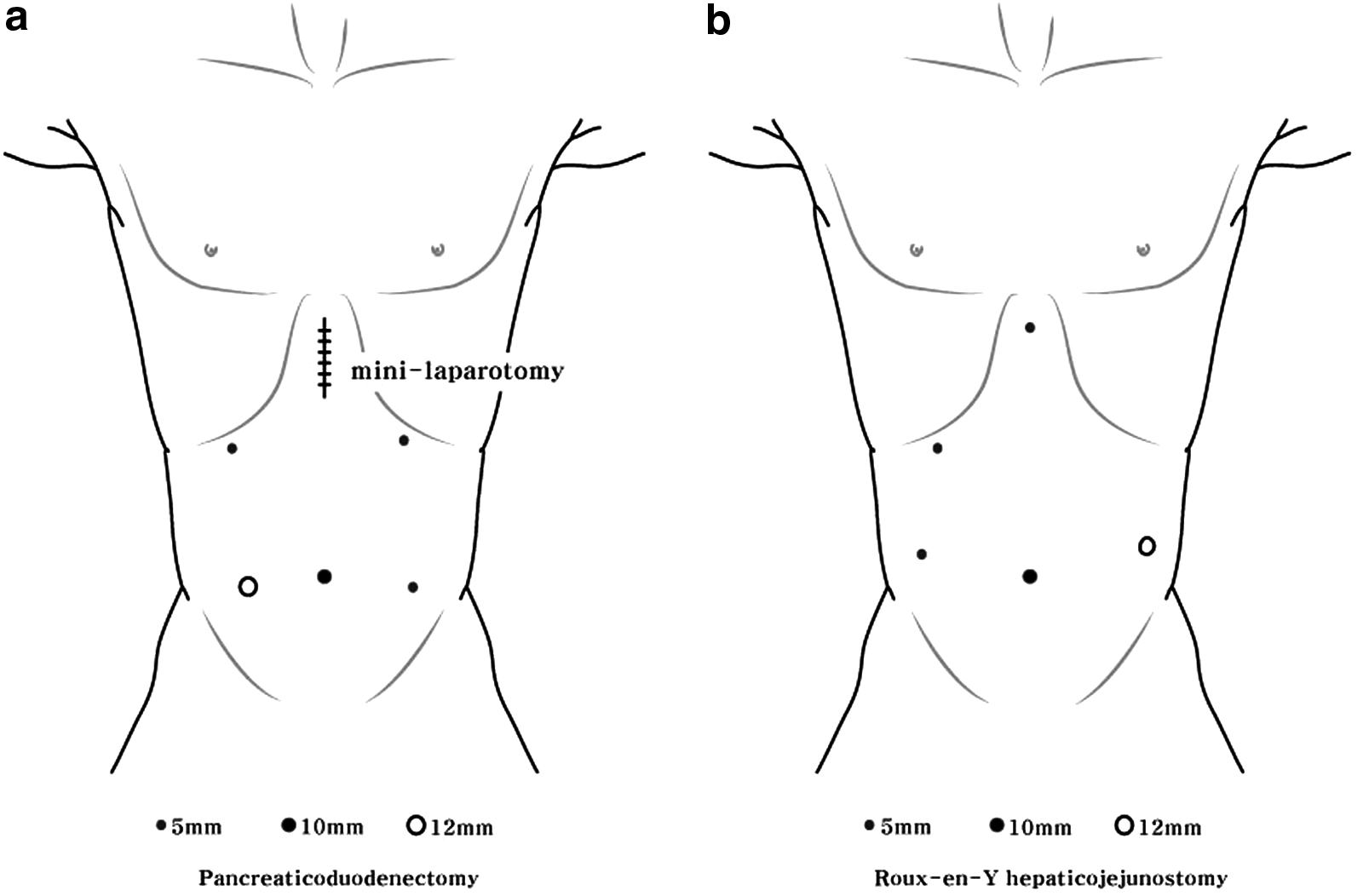
Trocar placement for
When LRYCJ or laparoscopic Roux-en-Y hepaticojejunostomy was performed, the trocar placement was focused on biliary surgery (Fig. 1b). Four trocars were used in general, but in some cases of laparoscopic choledochal cyst excision, five trocars were used. When four trocars were used, a 12-mm trocar was inserted slightly beneath the xiphoid process, and then two 5-mm trocars were placed, similar to the trocar placement for a four-port cholecystectomy. When five trocars were used, the 12-mm trocar was placed at the left flank on the anterior axillary line, slightly above the level of the umbilicus, and three 5-mm trocars were placed in the left upper quadrant, right upper quadrant, and right flank area.
Preparation of the CBD
Preparation of the CBD for anastomosis was different according to each operation. When LPD was performed, the CBD was resected en bloc with the pancreas. In some diseases, lymph node dissection of the hepatoduodenal ligament was performed. Because a considerable amount of time elapses from the transection of the CBD to CJ, the CBD stump was clamped with an endo-bulldog.
When LRYCJ for palliative biliary bypass was performed, the CBD was transected, and the stent, previously placed by endoscopy, was removed, along with bile debris (because this procedure was generally performed on patients for whom multiple endoscopic treatments had failed). A choledochoscope was introduced through a trocar, and the proximal CBD was examined to confirm that there was no residual debris. The distal CBD was suture-ligated.
When LRYCJ was performed for recurrent choledocholithiasis, a partial transverse incision was made in the anterior wall of the CBD. Stones were extracted using a stone basket and saline flushing. In difficult cases, a stone forceps could be directly introduced into the abdomen through one of the trocar incisions after removal of a trocar. A choledochoscope was inserted through the epigastric trocar. After the complete extraction of stones was confirmed, the CBD was completely resected, and the distal part was suture-ligated.
When laparoscopic choledochal cyst excision was performed, the complete excision of the CBD required a considerable amount of time. The distal part of the choledochal cyst was resected after identification of the transition zone at the intrapancreatic portion of the CBD. The proximal portion of the cyst was divided at the confluence of the right and left hepatic ducts.
Preparation of the Roux-en-Y limb
When LPD was performed in our center, instead of using a Roux-en-Y limb, the distal jejunum was pulled through the transverse colon mesentery in a retrocolic fashion and anchored to the Glissonian sheath, near the bile duct, to be anastomosed. When anchoring was performed, a long blind limb, approximately 5–6 cm in length, was left to use as a handle during CJ (Fig. 2).
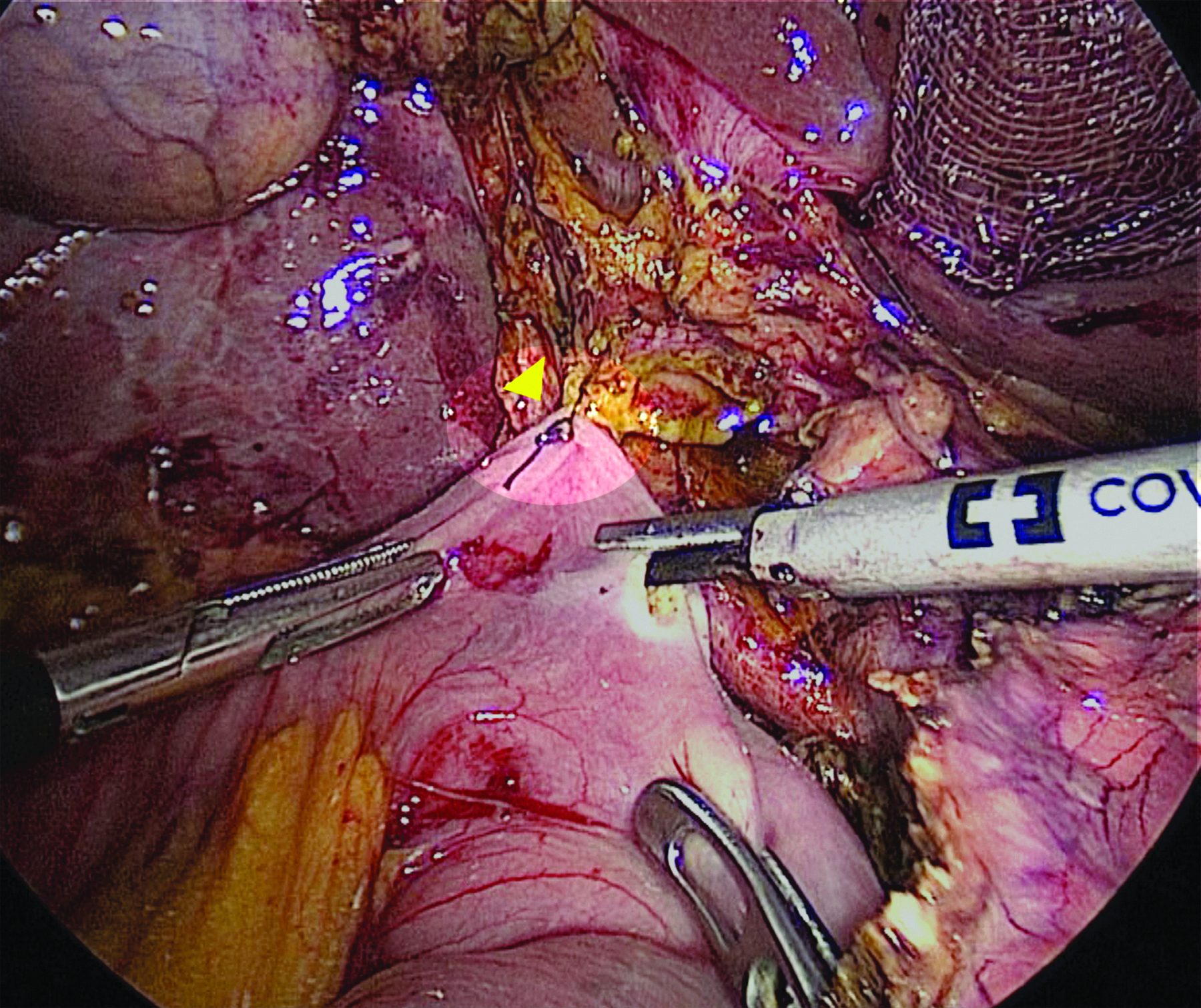
Long blind limb left after anchoring suture (arrowhead) during laparoscopic pancreaticoduodenectomy.
When LRYCJ was performed, the jejunum approximately 50–60 cm distal to the Treitz ligament was divided using an Endo-GIA® stapler (Ethicon Endosurgery Inc., Cincinnati, OH). The distal portion of the divided jejunum, which was the Roux limb, was pulled up in an antecolic or retrocolic fashion and anchored to the Glissonian sheath near the bile duct to be anastomosed.
CJ
CJ was the most important procedure. Using a Harmonic® scalpel (Ethicon Endosurgery Inc.), an incision was made on the antimesenteric side of the anchored Roux limb. An end-to-side anastomosis was performed using 4-0 absorbable, coated monofilament sutures (Monosyn®; B. Braun, Melsungen, Germany). Before beginning the anastomosis, a single bite was taken from the duct wall and jejunum, and a knot on the right side of the patient was made outside the duct wall. This suture was used to make a single continuous row of sutures, running from the right side of the patient to the left and anastomosing the posterior wall of the duct to the jejunum. After completion of the posterior wall suture, this suture was tied to an independent suture placed at the edge of the anastomosis, on the left side of the patient (Fig. 3). In the presence of bile duct enlargement, the anterior wall of the duct was sutured continuously in the same fashion. A separate 4-0 monofilament suture was used to anastomose the anterior row continuously in the same direction, which was also tied to the independent edge of the suture. When there was no enlargement of the ducts, a continuous suture was made on the posterior wall, and interrupted sutures were made on the anterior wall.
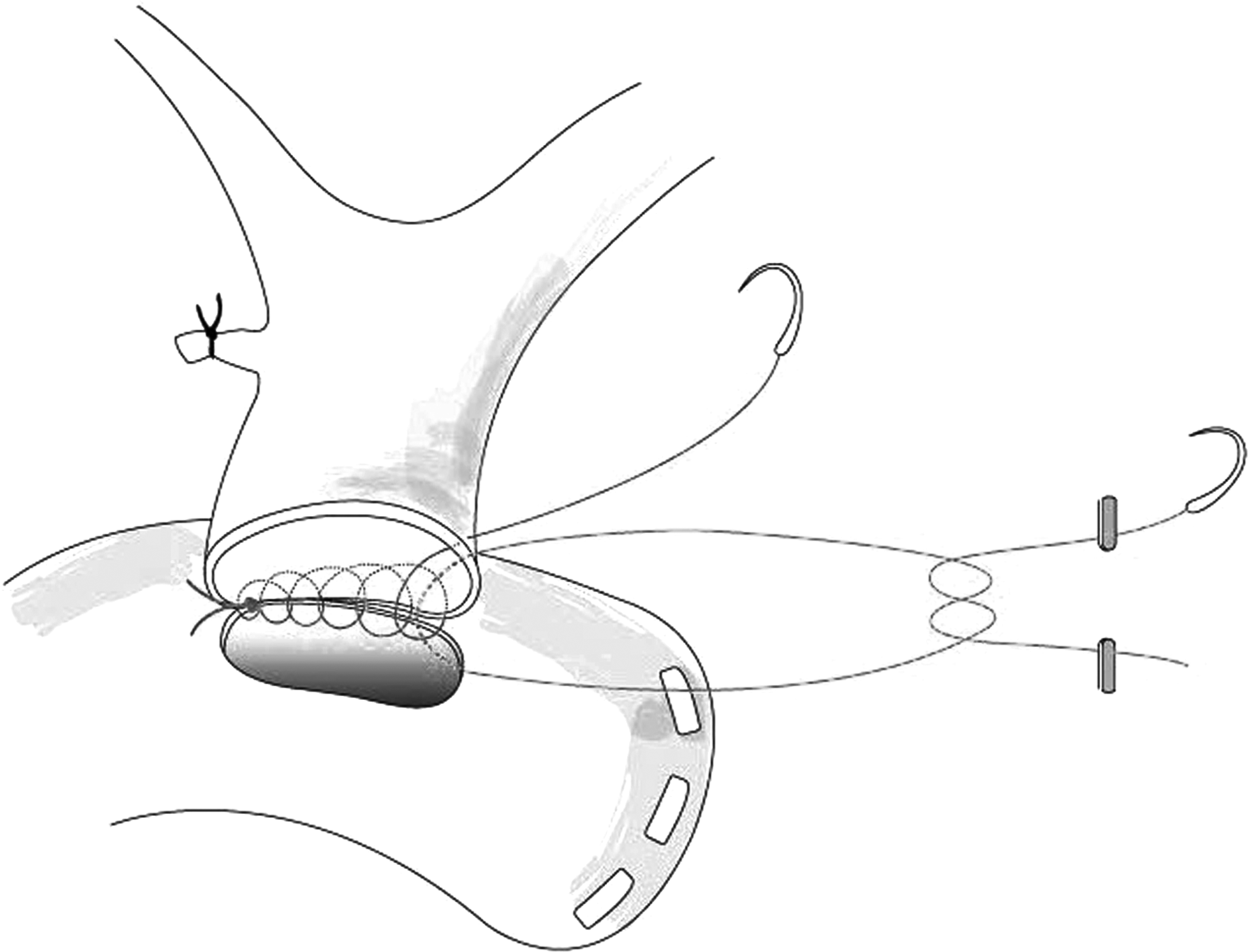
Posterior wall suture and independent edge suture of the choledochojejunostomy.
Jejunojejunostomy or duodenojejunostomy
When performing LPD, the authors used a method in which CJ was first performed laparoscopically. 10 After this procedure, a mini-laparotomy approximately 5 cm in length was placed in the epigastrium, directly over the pancreatic stump. Through this incision, the pancreaticogastrostomy and end-to-side duodenojejunostomy were performed (Fig. 4). The inset in Figure 4 shows how to perform pancreaticogastrostomy through such a small incision.
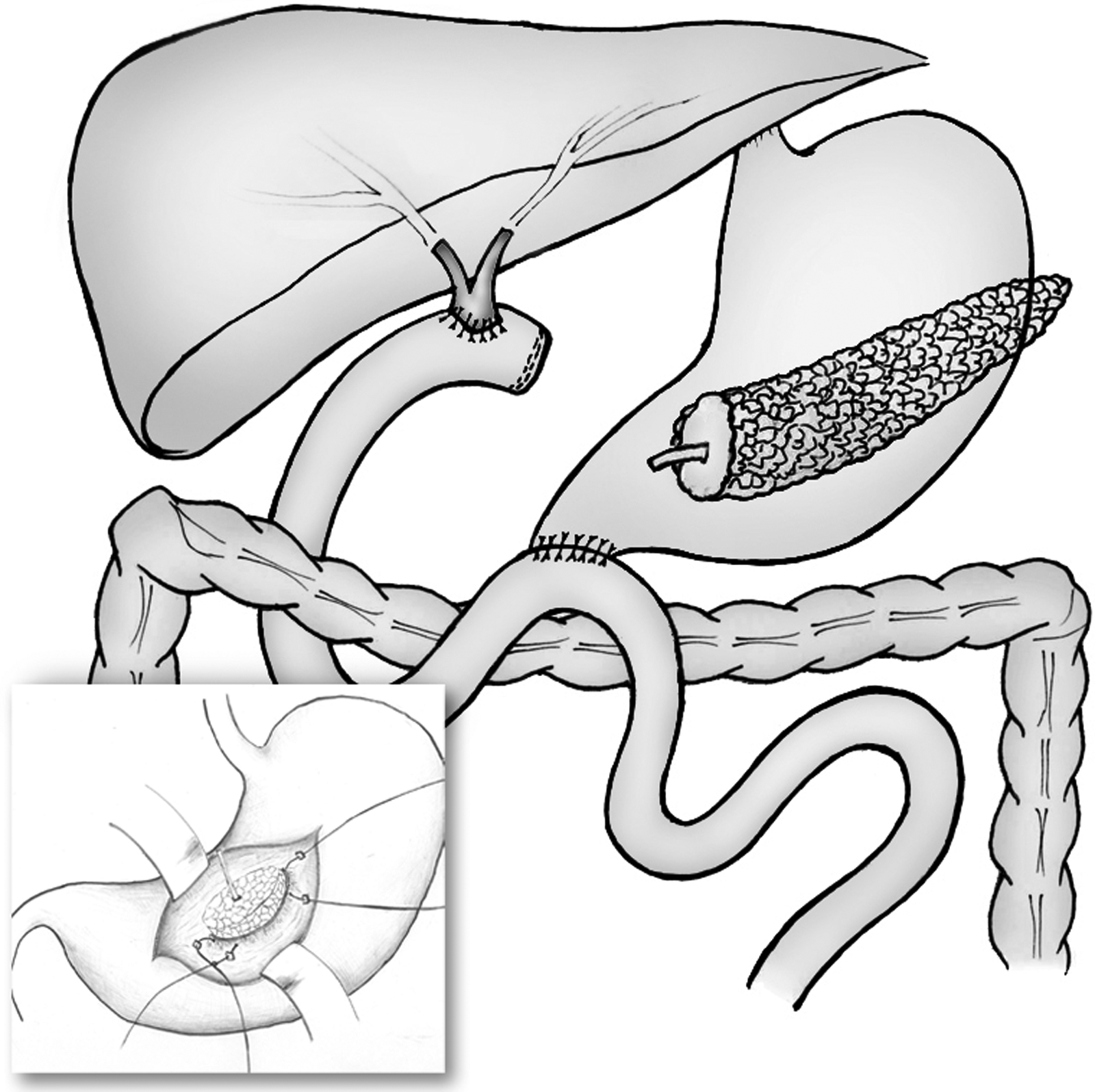
Reconstruction after laparoscopic pancreaticoduodenectomy.
In cases of LRYCJ, a side-to-side jejunojejunostomy was performed approximately 60 cm distal to the CJ. Earlier, intracorporeal anastomosis was performed using an Endo-GIA stapler. At present, we usually extend the umbilical incision to approximately 3 cm, place a wound retractor (ALEXIS®; Applied Medical, Rancho Santa Margarita, CA) in this incision and perform the extracorporeal anastomosis.
Learning curve plateau
The plateau was defined as the period after which the operative time decreased dramatically. The exact operative time was recorded from the video analysis. The time for LCJ was measured in a manner that could be applied to all operations because every operation required different steps before CJ and different steps for Roux limb formation. The time for LCJ was measured from the beginning of the anchoring suture to fix the jejunum to the Glissonian sheath to the cutting of the last suture. The patients were categorized into groups of 10 in surgical order. Because 82 of the total of 84 patients were analyzed, the last group contained 12 patients. Complications of LCJ, such as the development of bile leakage or biliary stricture, were evaluated. When the drainage fluid from the drain placed beneath the biliary-enteric anastomosis was bile-colored, bile leakage was classified according to the International Study Group of Liver Surgery classification. 11 The surgical results of the patients who received surgery before and after the learning curve were compared.
Results
In total, 84 patients underwent procedures including LCJ between September 2007 and July 2014. The patients' demographics are shown in Table 2. No patients required conversion to open surgery. Thirty-one patients had no CBD dilation. Of the 84 patients, 2 were transferred to our center after iatrogenic CBD injury at another center. In both these patients, the tissue surrounding the CBD was acutely inflamed and very friable. Because of these factors, the suturing was technically very difficult. Therefore, these 2 patients were excluded from the analysis.
The first three groups included the 30 surgeries performed before the learning curve, group 4 represents the learning curve, and the last four groups included the 41 surgeries performed after the learning curve.
BMI, body mass index; CBD, common bile duct; LCJ, laparoscopic choledochojejunostomy.
The learning curve was assessed by reviewing the LCJ time. The LCJ times of each group are shown in Figure 5. The average LCJ time was 68.7±8.2 minutes for the first group, 53.4±10.1 minutes for the second group, 48.2±13.9 minutes for the third group, 28.7±3.7 minutes for the fourth group, 26.6±4.9 minutes for the fifth group, 27.3±5.4 minutes for the sixth group, 26.7±3.3 minutes for the seventh group, and 27.4±5.4 minutes for the eighth group. Compared with the first three groups, the fourth group showed a significantly shorter LCJ time. The following groups showed a plateau, indicating that there were no more significant changes in the LCJ time. After the plateau of the learning curve was reached, the average LCJ time was 27.4±4.7 minutes.
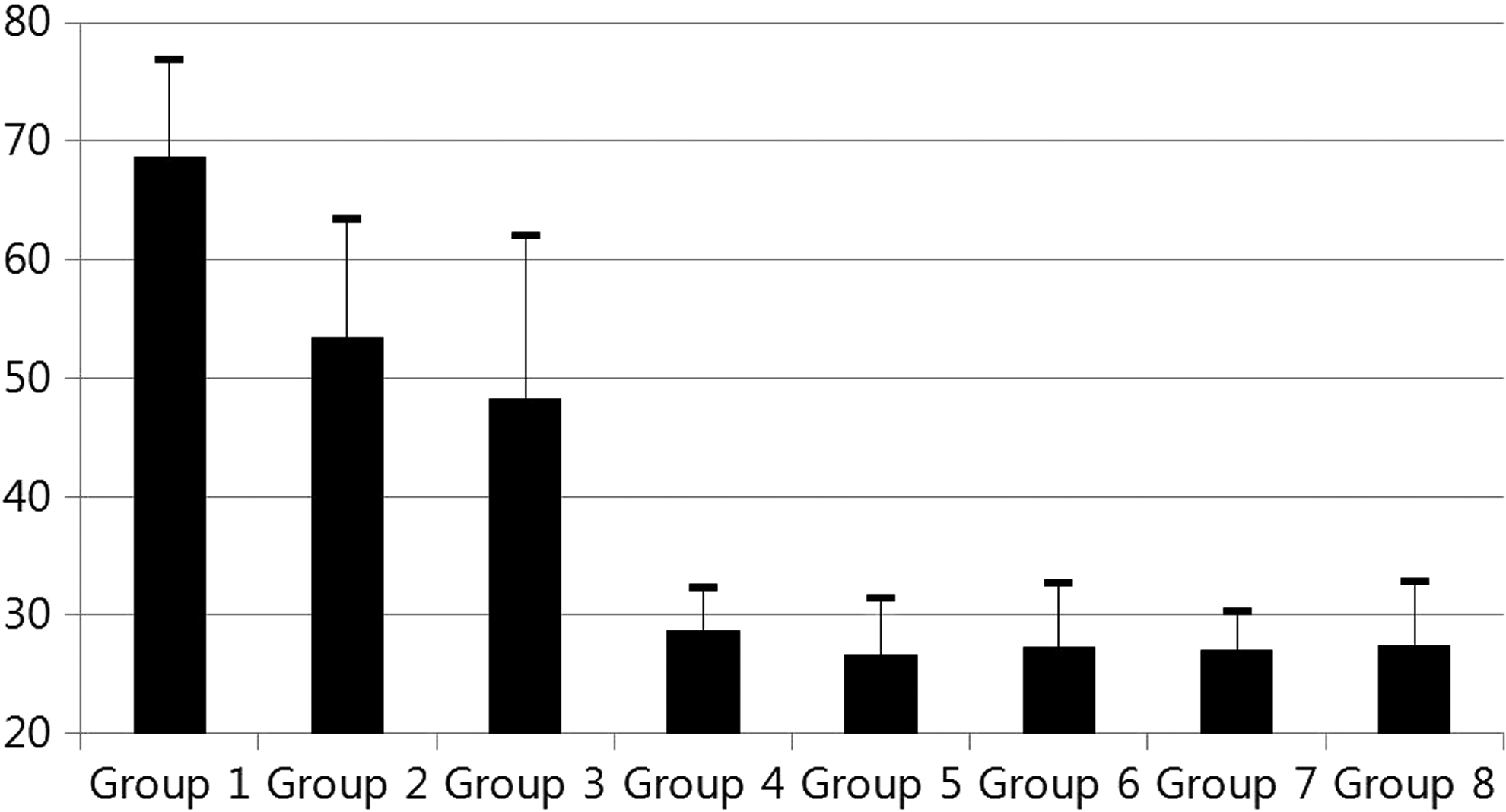
Learning curve of laparoscopic choledocojejunostomy by group.
An analysis was performed to compare the 30 operations performed before the plateau of the learning curve (the first three groups) and the 52 operations performed after the plateau (the last five groups). The numbers of each procedure performed and the distribution of normal-caliber CBD were similar between the two groups. The perioperative data are shown in Table 2. There were 6 patients with postoperative bile leakage. All 6 cases occurred before the surgeon reached the plateau of the learning curve, and 5 cases had no CBD dilation. Five of the 6 patients had grade A bile leakage. Only 1 patient, who had undergone surgery twice because of bleeding immediately after surgery, had grade B bile leakage and required additional percutaneous transhepatic biliary drainage and catheter insertion. Over the 82-month follow-up period from September 2007 to July 2014, 10 patients had biliary strictures. No correlations with regard to the learning curve were observed in these patients. After the collection of more cases, the factors associated with biliary stricture should be assessed.
Discussion
CJ is a type of biliary-enteric anastomosis often used in the field of hepatobiliary and pancreatic surgery. However, the anastomosis site is somewhat deviated from the midline and is obscured by the liver. Even in open surgery, maintaining an optimal view is difficult, and thus this procedure often results in a lengthy incision. Therefore, laparoscopic surgery has an advantage over open surgery in that a better, more magnified view can be provided for the surgeon. Experiences with LPD, performed for benign tumors and low-grade malignancies of the periampullary region, have been increasing. However, there have been difficulties in performing the reconstruction phase laparoscopically. Therefore, several authors have reported methods for placing a mini-laparotomy and performing an anastomosis through this incision. The authors of this study used a method that minimized this incision due to laparoscopic CJ performance, which deviated from the midline. 10
LRYCJ is also used in biliary bypass surgeries for unresectable periampullary tumors. After several reports proved the feasibility of laparoscopic biliary bypass, the benefits of laparoscopy over open surgery for these patients seemed clear.12,13 However, since the development of biliary stenting, many patients have been treated with this even less invasive method. Some systematic reviews have concluded that endoscopic metal stenting is the intervention of choice in patients with malignant distal biliary obstructions.14,15 Although laparoscopic biliary bypass was being actively performed at the time that these studies were conducted, there were no studies in which laparoscopic biliary bypass and biliary stenting were compared. Biliary stenting in the palliative setting incurs the risk of multiple procedures, as already described in a meta-analysis. 14 For patients with a short life expectancy, a single procedure of laparoscopic biliary bypass can be better than multiple “noninvasive” stenting procedures.
The treatment of recurrent choledocholithiasis can be difficult. Generally, endoscopic retrograde cholangiopancreatography with sphincterotomy was performed. However, in cases of patients with postsphincterotomy papillary stenosis, irreversible CBD dilatation, or nonextractable recurrent CBD stones and in patients in whom endoscopic therapy has failed, surgical biliary drainage is indicated. 16 In these circumstances, the surgeon must choose between RYCJ and CD. Many authors have advocated CD, and there have been many reports of laparoscopically performed CD.5,17,18 However, there have also reports of postoperative sump syndrome and cholangitis development after CD, which rarely occur after RYCJ.19–21 In contrast, a disadvantage of RYCJ is its technical difficulty. It requires more extensive dissection than CD, including a circumferential dissection of the common duct. In addition, the biliary-enteric anastomosis is more difficult because of the proximity of the hilar plate. Finally, the creation of the Roux-en-Y jejunal limb is required. 22 However, compared with CD, RYCJ has the advantages of a lower incidence of postoperative cholangitis, better long-term patency, and more efficient biliary drainage. 16 When this procedure is performed laparoscopically, it can be of great benefit to the patient.
As mentioned in Results, the LCJ time decreased as the surgeon progressed along the learning curve. In addition, there were several cases of bile leakage during the earlier period, but there were no such cases during the later period. This drastic shortening of the LCJ time was possible because of several technical tips acquired during this study. First, an anchoring suture between the Roux limb and the Glissonian sheath near the bile duct should be placed before beginning the anastomosis. Second, leaving a blind loop of the Roux limb of sufficient length helped with the placement of exact sutures at precise locations. Because the bile duct is a fixed structure and the laparoscopic needle holder, unlike in open surgeries, has limited ranges of angles and motion, the manipulation of the jejunum can play an important role in anastomosis. Leaving a blind loop 5–6 cm in length allows the surgeon to grasp this blind loop and use it as a “handle,” thus making more precise sutures possible. During the performance of the anastomosis, coated monofilament sutures are better than multifilament sutures. Although multifilament (Vicryl®; Ethicon, Somerville, NJ) sutures are easier to handle, after a row of continuous suture is performed, there is less room for traction because of the friction between the suture and the surrounding tissue. Coated monofilament sutures are more difficult to handle, but when the suture is pulled after a row of continuous suture, there is more room for correction of any loosening. This is due to the low amount of friction that monofilament sutures have with the surrounding tissue.
In the present study, there was a relatively high stricture rate. It seems that to lower the stricture rate, it is important to consciously avoid posterior row loosening. In the earlier period, there were several cases of posterior row loosening, which may have led to bile leakage, ultimately resulting in biliary stricture. This problem can be avoided by the maintenance of tension on the posterior row suture while tying this suture with the independent edge suture after the completion of the posterior row anastomosis. After application of this technique, both bile leakage and biliary stricture decreased.
When the bile duct that is to be anastomosed is not dilated, the anastomosis takes a longer time than a dilated bile duct. Additionally, there is an increased risk of bile leakage. Our solution to this problem is to perform running sutures on the posterior row and interrupted sutures on the anterior row. The anterior sutures are also not tied individually; rather, they are tied after all the sutures are in place. Thus, accidental suturing of the posterior wall can be avoided, and the placement of sutures will be supported in near exact intervals. Using this method, the total anastomosis time was similar to that of dilated duct anastomosis. Also, the number of patient cases with bile leakage decreased.
A limitation of this study is that only factors directly related to LCJ were evaluated. Because many different types of surgery were included in the analysis, comprehensive factors such as length of stay, morbidity, or mortality were not evaluated.
To perform LCJ, the surgeon must have advanced laparoscopic skills. A steep learning curve exists, even for surgeons experienced in minimally invasive surgery. However, with a careful video review, education of the surgical team, and various technical tips, such as those described herein, this learning curve can be shortened.
Conclusions
LCJ is a safe and feasible procedure that can be used in many procedures in the field of hepatobiliary and pancreatic surgery. After a certain learning curve, experienced surgeons can perform LCJ with acceptable results.
Footnotes
Disclosure Statement
No competing financial interests exist.