
Abstract
Abstract
Background:
Transoral techniques for endoscopic thyroidectomy have recently been reported, including a robotic transoral technique to access the thyroid gland. Herein, we developed a robotic transoral periosteal thyroidectomy technique.
Materials and Methods:
The da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) robot was used in two human cadavers to perform robotic transoral periosteal thyroidectomies. In the first cadaver, the anterior neck was exposed below the platysmal muscle. The anatomical spaces and surgical planes were observed with four ports by a periosteal approach. In the second cadaver, robotic transoral periosteal thyroidectomy was performed using three ports.
Results:
A total thyroidectomy and central neck dissection were performed in two cadavers using the da Vinci robot with the transoral periosteal approach. Complete thyroidectomy and central neck dissection were possible without injury to the recurrent laryngeal nerve.
Conclusions:
Robotic transoral periosteal thyroidectomy provides superior access to the thyroid and central neck compartment. Transoral thyroidectomy using four ports is a feasible and safe method.
Introduction
A
Transoral techniques for endoscopic thyroidectomy have been reported to overcome the limitations of previous approaches.8–10 However, previous transoral approaches have also shown limitations, such as limited operative view and collision of endoscopic instruments. To overcome these limitations, Richmon et al.11,12 reported a technique for thyroidectomy using a transoral robotic approach. Although their approach was successful, technical challenges remain, including accessing the central compartment through the mouth.
The aim of this study was to define anatomical spaces and surgical planes and to develop appropriate methods for transoral robotic surgery. We developed a method with four ports and three ports that can be applied to robotic thyroidectomy using the new periosteal approach.
Materials and Methods
Two human cadavers were obtained from the University of California, San Francisco. Both were male with full dentition.
To define the anatomical spaces and surgical planes of the first cadaver, an incision was made along the lower border of the mandible extending laterally up to the mandibular angles. After the skin flap was reflected, the platysma muscle was separated from underlying structures to fully expose the anterior neck. After the neck was extended, the oral cavity was opened, and the lips were retracted with a dental lip retractor.
The periosteal approach with four ports was attempted first. A 2-cm incision was made for the camera port by sulcal incision in the buccal surface at the level of the central incisors. Bilateral vertical incisions were extended into the alveolar mucosa, and mucoperiosteal flaps on the buccal surface were raised in the midline by a periosteal elevator. Care was taken not to elevate the mentalis muscles atraumatically with the periosteal flap. Dissection continued around the inferior aspect of the mandible until the subplatysmal plane was identified. Another 2-cm incision was made in the same way in the midline floor of the mouth on the lingual surface. Two more 1.5-cm incisions were made in the gingival–buccal sulcus at the level of the first molar to avoid injuring the mental nerves. Dissection proceeded along the periosteum of the mandible into the submental area. The 8-mm bariatric cannulae were placed in the two lateral incisions, and 12-mm bariatric cannulae were placed in the two midline incisions (Fig. 1).

The anterior view after port insertion in transoral periosteal thyroidectomy using four ports.
The da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) was then brought to the bedside at an approximately 30° angle, and the cannulae were docked. A 0° endoscope was advanced through the 12-mm camera port of the buccal surface into the submental, subplatysmal area. ProGrasp™ forceps (Intuitive Surgical) were placed through the left gingival–buccal incision, and a Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH) was advanced through the floor of the mouth. Through the right gingival–buccal incision, a Maryland dissector was placed. Under endoscopic visualization, the midline raphe of the strap muscles was identified at the level of the thyroid cartilage notch, and it was divided. The strap muscles were retracted bilaterally with the Maryland dissector and the ProGrasp forceps and elevated with the Harmonic scalpel or monopolar cautery to expose the thyroid gland. The isthmus was divided with the Harmonic scalpel. The superior lobe of the right thyroid gland was grasped and retracted inferomedially using the left ProGrasp forceps. At that time, the right Maryland dissector laterally retracted the right strap muscle. This continued until the superior vascular pedicle was identified and cauterized using the Harmonic scalpel. The recurrent laryngeal nerve was identified by gentle blunt dissection at its entry point and was traced inferiorly. The thyroid gland was then further retracted medially, allowing a capsular dissection, and the right lobe was freed entirely. The left thyroid lobe was removed in a similar method, and a central neck dissection was performed. After thyroidectomy, intact mentalis muscles were observed. The midline incisions were closed by suturing the interdental papillae together.
For the second cadaver, a modification method using three ports was used, as described by Richmon et al. 12 The camera-port incision was made by sulcal incision in the buccal surface of the central incisors instead of by buccal–gingival incision. The three-port and four-port methods differ in the lingual surface incision.
Results
We performed a total thyroidectomy using the new transoral periosteal approach by the da Vinci robot surgical system in two human cadavers.
For the first cadaver, we made an incision along the lower border of the mandible to define the anatomical spaces and surgical planes. The external view was observed during dissection to reveal that the subplatysmal plane is found easily as one dissects along the inferior aspect of the mandible (Fig. 2). Using four ports in the first cadaver, a surgeon could more easily deal with bleeding and manipulate the thyroid and surrounding tissues better than with three ports. However, it proved very difficult to connect the robotic arms to each port, and collisions between instruments occurred frequently. The position and height of the ports must be altered to alleviate these issues.
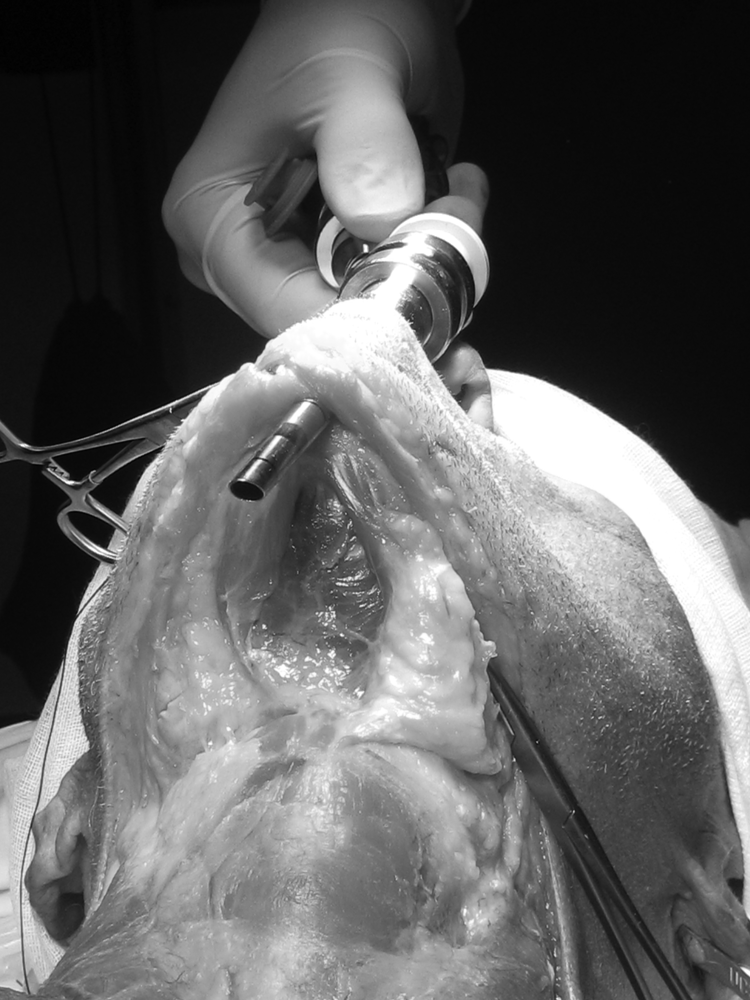
The external view of port placement for the camera in transoral periosteal thyroidectomy. The dissection plane is made naturally at the subplatysmal area without any artificial force.
For the second cadaver, we performed a robotic transoral periosteal thyroidectomy (TOPOT) using three ports. There was no injury to maxillary teeth or the nose when using three ports. Collision between robotic instruments was not observed. However, there are some disadvantages, including difficulty controlling emergency bleeding and managing the thyroid with thyroiditis.
Discussion
Recently, several groups described transoral thyroidectomy with varying methods.8–10 Transoral techniques that use endoscopic instruments still have limitations, such as a limited operative view and the collision of endoscopic instruments. We believe that transoral robotically assisted thyroidectomy can overcome these limitations to facilitate the technique in two previous reports by Richmon et al.11,12 They concluded that transoral robotically assisted thyroidectomy is attractive because it embodies minimally invasive principles, including limited tissue dissection and retraction, close access to the thyroid gland, natural orifice surgery, and no cutaneous scar or deformity. 12 However, this technique is still experimental and needs modification to be more realistic and potentially less harmful. We compared the advantages and disadvantages of a variety of methods and studied the points that require development.
In this study, we tried to develop robotic transoral thyroidectomy using a new periosteal approach. All incisions were made along the periosteum of the mandible, so this method was named “robotic TOPOT.” Using this periosteal approach, a dissection plane at the subplatysmal level is located easily and elevated with minimal effort. Midline incisions for the camera and first port were made along the gingival margin and gingival flap. Richmon et al. 12 reported a modification method with three ports that requires a gingival–buccal incision in the midline between the mentalis muscles. This approach can potentially result in “puckering” or sagging of the mental subunit and a cosmetic deformity of the mentum. 13 However, the periosteal approach does not damage the mentalis muscle and likely lowers the risk of cosmetic deformity of the mentum. In addition to avoiding floor of mouth incisions, there is no risk of injury to Wharton's papillae and the tongue base, even with the four-port method.
Previous transoral endoscopic or robotic surgery used three or fewer ports, and this is the first report of transoral surgery using four ports in robotic thyroidectomy. All four ports are placed intraorally, and scars are not visible. The ports consist of a camera port, a surgeon's acting port, a surgeon's assisting port, and a pure assisting port. Without an additional assisting port, three-port methods are critically limited because it is essential to retract the thyroid and tissues during the procedure to identify accurate surgical planes. Excessive retraction of the thyroid and tissues may lead to severe complications such as injury to the recurrent laryngeal nerve or bleeding. In contrast, a surgeon using the four-port method can manipulate the thyroid and surrounding tissues without extreme retraction. Moreover, surgeons can easily deal with bleeding using four ports. However, the four-port method also has disadvantages. It was very difficult to connect the robotic arms to each port, and instrument collision occurred more frequently than with three ports. As a result, the position and height of the ports were frequently changed. As described by Richmon et al., 11 the port in the midline of the mouth floor impinges on the mandibular and maxillary teeth. This limitation can be overcome by using a longer bariatric port. From this study, we think that robotic TOPOT using four ports is a feasible and safe method. To prove this, the technique should be further developed and modified through more experiments.
A sulcal incision in the midline of the buccal surface was used for a camera port with the three-port method. Except for the camera port, this method is very similar to a modified method described by Richmon et al. 12 By moving the endoscopic port anterior to the mandible, we obtained excellent mobility without any restriction from the facial skeleton or injury to the patient's teeth and nose. There were also no severe collision between robotic arms (Fig. 3). However, as previously mentioned, excessive retraction of the thyroid and tissues cannot be avoided without an additional assisting port.

The external view during the transoral periosteal thyroidectomy operation using four ports. The plane of the camera port is different from that of the other three working ports.
In neck surgery, the transoral approach provides superb visibility of the central compartment to the level of the innominate artery. This method also offers midline exposure and equivalent access to both the right and left thyroid lobes and central compartments. The view from the transoral approach is similar to the view with open thyroidectomy. The four-port method allows more accurate dissection of the lymph nodes of the central neck compartment while lowering risks to recurrent laryngeal nerves and other structures. The da Vinci robot offers three-dimensional visualization for optimal depth perception, while wristed instruments enhance control and accuracy. In this study, we found that robotic TOPOT provides the safest access to paratracheal beds and the central compartment. We believe that this method may permit more comprehensive treatment of the posterolateral suspensory ligament of Berry, the recurrent laryngeal nerve, and neck lymph nodes. We expect that this method can be applied in surgery for thyroid cancer patients.
Several technical challenges remain despite the many advantages of this method. Lateral gingival–buccal port placement introduces a risk to the mental nerve. While making gingival–buccal incisions, a surgeon should avoid the area around the fourth and fifth teeth to lower risks to the mental nerve. As previously mentioned, potential risks include dentition injuries. Further evaluation of this technique should include optimal port placement and movement. Mouth guards may help avoid injuries to the maxillary teeth. Additionally, oral flora could contaminate the neck contents. However, there is no evidence that previous transoral approaches have higher risks of infection than transcervical approaches. Intravenous antibiotic administration and preoperative preparation of the oral cavity are critical for reducing the risk of infection. Although further technical enhancement is necessary before implementation on live human patients, robotic TOPOT is a promising method for minimally invasive thyroid surgery.
Conclusions
Robotic TOPOT using four ports or three ports provides superb access to the thyroid and central neck compartment.
Footnotes
Acknowledgment
The research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (2012R1A1A1013413).
Disclosure Statement
No competing financial interests exist.