
Abstract
Abstract
Background:
This study evaluates the efficacy of intraoperative neuromonitoring (IONM) on voice performance in robotic thyroidectomy.
Materials and Methods:
The study was based on a prospective randomized series. Between June 2011 to September 2012, 50 patients with thyroid cancer who underwent robotic thyroidectomy were enrolled. The IONM and non-IONM groups consisted of 25 patients each. Voice Handicap Index (VHI), voice range profile (VRP), and laryngoscopy were used to assess voice function before surgery and at 2 weeks, 3 months, and 6 months after the operation.
Results:
No palsy was diagnosed by laryngoscopy in either group. VHI values were similar in both groups. In the IONM group, there was significantly earlier recovery in VRP minimum intensity compared with the non-IONM group. However, there were no differences of mean change of VRP maximum frequency and intensity or minimum frequency between the two groups.
Conclusions:
We found that IONM facilitated more rapid recovery of voice function, especially in VRP minimum intensity, during robotic thyroid surgery.
Introduction
V
The high-resolution three-dimensional image magnification and the precise movements through articulating instruments available only in robotic surgery facilitate the identification of laryngeal nerves and parathyroid glands, providing visual discrimination among different tissues and depths and meticulous fine technique of dissection.
Many surgeons now apply intraoperative neuromonitoring (IONM) during thyroid surgery. IONM has gained widespread acceptance as an adjunct to the gold standard of visual nerve identification.8–10 Several studies have shown IONM added value to clinical outcomes of thyroidectomy in terms of preserved individual voice performance and reduced incidence of vocal cord palsy.11–13
Most previous studies have reported on the feasibility, safety, and efficacy of IONM after conventional open14–16 or endoscopic thyroidectomy.17,18 De facto, nerve laryngeal palpation (tactile sensation) or the use of magnifying glasses as an intraoperative technique for identifying the RLN or the EBSLN during endoscopic thyroidectomy is not feasible for the small cervical incision or the remote cervical access. Endoscopic thyroidectomy requires the surgeon to rely more fully on visual cues from the monitor. Other authors have confirmed that IONM is complementary to video-endoscope magnification.17,18
To date, no study has examined voice outcomes after robotic thyroidectomy with IONM. Here we evaluated the efficacy of IONM for voice performance after robotic thyroidectomy.
Materials and Methods
The study included 50 papillary thyroid cancer patients who underwent robotic thyroidectomy using the bilateral axillo-breast approach at the Korea University College of Medicine (Seoul, Korea) from March 2011 to September 2012. Permission to perform this prospective, randomized clinical trial was obtained from the Korea University Anam Hospital Institutional Review Board (protocol number MD1108).
This study was conducted in accordance with the principles of the Declaration of Helsinki and “good clinical practice” guidelines. The study and procedure were explained to all patients preoperatively. Written informed consent was obtained from each patient in advance. Participants were assured anonymity. Included in the study were patients older than 18 years who were scheduled to undergo robotic surgery and were able to provide informed consent. Only cases with malignant thyroid nodules that were confirmed by cytology of fine-needle aspiration were included.
The recruited patients were randomized into two groups (IONM and non-IONM) using a block randomization method.
Selection criteria for both group patients for robotic thyroidectomy were the same.
Exclusion criteria were diffuse toxic goiters (Graves' disease), nodules >4 cm, recurrent goiters, patients with RLN palsy, and patients who had undergone previous neck surgery.
Perioperative data and complications were prospectively recorded. The technique applied was identical, and procedures were performed by the same surgeon (H.Y.K.) with more than 10 years of experience in robotic surgery. The NIM 2.0 system (Medtronic Xomed Surgical Products, Jacksonville, FL) was used for neuromonitoring of the IONM group according to the international standards guideline. 8
A robotic thyroidectomy using a standard bilateral axillo-breast approach was performed with the da Vinci®-S Surgical System (Intuitive Surgical, Mountain View, CA) in both groups. 19 For a robotic thyroidectomy using a standard bilateral axillo-breast approach, the blunt dissection into the subplatysmal space in the neck was extended superiorly to the level of the thyroid cartilage and to the medial border of each sternocleidomastoid muscle laterally. The robotic camera was inserted through the 12-mm right breast port, and the ultrasonic shears (Harmonic® scalpel; Ethicon Endo-Surgery Inc., Cincinnati, OH) or the monopolar electrocauterization device was inserted through the 8-mm left breast port. The 8-mm bilateral axillary robotic trocars were used as working ports with the ProGrasp™ forceps (Intuitive Surgical) and Maryland forceps. The Harmonic scalpel used to ligate thyroid vessels, to dissect thyroid tissues at the isthmus, and to detach the thyroid gland from the trachea. After complete procedures, precise bleeding control was achieved, and a 3-mm closed suction drain was inserted through the 8-mm axillary port in the left side.
In the IONM group, all patients underwent endotracheal intubation with electromyography tube surface electrodes integrated for monitoring. No additional neuromuscular blocking agents were used following intubation. Also, during the operation, both RLNs were identified using a nerve stimulator with low pulse stimulation of 0.5–1.0 mA. We used the permanent cautery hook (number 400183) for the da Vinci equipment (Intuitive Surgical) as a stimulator probe that connected to the NIM 2.0 system. The interrupted stimulation technique was conducted at 1 mA, impulse duration of 100 milliseconds, and frequency of 4 Hz.
In both groups, the whole cervical course of the RLN is traced and identified before sealing the inferior thyroid artery. In the non-IONM group, the RLN is identified and exposed solely with the endoscope, giving a magnified view of the nerve. In the IONM group, the standard technique for IONM is to stimulate both the vagus nerve and the RLN before thyroid dissection and after complete thyroidectomy. 8
RLNs were checked repeatedly at each step of robotic thyroidectomy according to the needs of the surgeon in both groups. After complete thyroidectomy and hemostasis, we ensure the integrity of laryngeal nerves with the optical magnification of the endoscope in the non-IONM group and with the functional integrity of the RLNs and vagus nerves by stimulation in the IONM group. All RLNs in the IONM group can identified by the NIM 2.0 system, so visual identification of RLNs was not an essential surgical process in the IONM group.
The primary end points were transient or permanent laryngeal nerve lesions, either uni- or bilateral, Voice Handicap Index (VHI), and voice range profile (VRP).
The VHI-30 survey, which consists of 30 questions including functional, physical, and emotional subscales, measuring defects in verbal communication, was used for evaluation of voice quality. 20 Each item on the VHI is scored using a 5-point scale ranging from 0 to 4.
Objective acoustic voice analysis was performed for the VRP, including maximum and minimum frequency (in Hz) and maximum and minimum intensity (in dB) of the voice range. In VRP tests, participants produced an A note at a comfortable pitch and proceeded to step or glide up to the greatest sustainable F0, including falsetto (Fmax). They then phonated at a comfortable pitch and stepped or glided down to the least possible F0, excluding vocal fry (Fmin). These procedures were repeated three times and averaged in each direction.
Laryngoscopy was performed to check for changes in vocal cord motility. In laryngoscopic findings, we defined no movement of vocal cords at least ipsilaterally as vocal cord palsy.
VHI, VRP, and laryngoscopy were used to test voice function before surgery and at 2 weeks, 3 months, and 6 months after the operation.
Dysfunction was considered permanent if it persisted for 12 months. Measurement of the RLN palsy rate was based on the number of nerves at risk.
Cancer patients, after surgery, were subjected to thyroid remnant ablation by radioactive iodine (131I) and placed under thyroid-stimulated hormone–suppressive
All patients' data were collected in a prospective manner. The sample size was estimated based on the principle of detecting a difference of −10 units for VRP and of −5 for VHI between the mean of the IONM and non-IONM groups with a 90% probability at P < .05, using power curve and sample size tools for one-way analysis of variance (i.e., a sample size of 25 subjects per group should provide 90% power to detect an VHI or VRP difference between the IONM study group and the non-IONM study group).
Pearson's chi-squared test was used for binomial analysis. The independent t test or the Mann–Whitney U test was used to compare continuous variables. Statistical analyses were performed using PASW Statistics version 18.0 (SPSS Inc., Chicago, IL). Reported P values are two-sided, and statistical significance was set at P < .05.
Results
In total, 50 patients were enrolled; the IONM and non-IONM groups consisted of 25 patients each. The non-IONM group included 19 women and 6 men with a mean age of 41.7 years (range, 27–59 years). The IONM group was composed of 23 women and 2 men with a mean age of 44.2 years (range, 20–66 years). All patients underwent robotic thyroidectomy using the bilateral axillo-breast approach. There was no statistical difference between the two groups in terms of body mass index, pathologic diagnosis, and tumor size. There was no difference between the two groups in total operation time and hospital stay. No transient or permanent vocal cord palsy occurred. There was no case of permanent hypocalcemia. The incidence of transient hypoparathyroidism in the IONM group was 36%, and that in the non-IONM group was 16%; however, there was no significant difference of transient hypoparathyroidism between the two groups (Table 1).
Data are mean ± standard deviation values (range), number of subjects, or number (%) as indicated.
FVPTC, follicular variant papillary thyroid carcinoma; LT4, levothyroxine; TG, triglyceride.
There were no intraoperative complications or instances of equipment malfunction or interferences between IONM and robotic accessories.
The non-IONM and IONM groups had similar VHI results. A declining trend was observed in both groups as time progressed. Decreased movement on laryngoscopic examination was found in 3 patients in each group at 2 weeks and 3 months postoperatively. However, at 6 months after surgery, only 1 case was observed in the non-IONM group versus none in the IONM group. Vocal cord palsy was not found in either group (Table 2).
Data are mean ± standard deviation values or number (%) as indicated.
VHI, Voice Handicap Index.
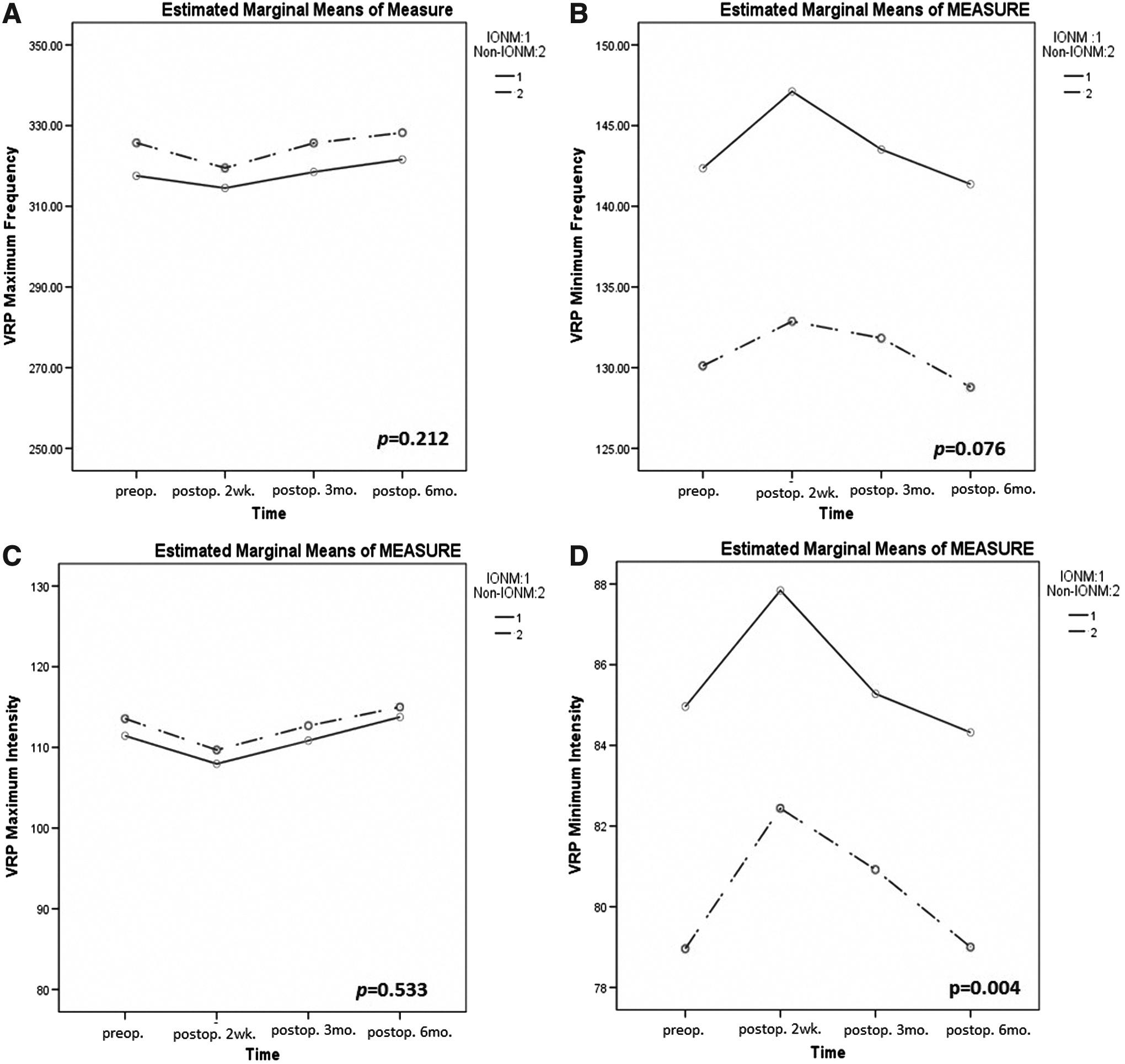
There were no significant differences in VRP maximum frequency and intensity between the two groups preoperatively or postoperatively. In both groups, VRP maximum frequency and intensity values were decreased at 2 weeks postoperatively compared with the preoperative values but had returned to preoperative levels by 6 months postoperatively. VRP minimum frequency and intensity were statistically different between the two groups preoperatively. However, the patterns of change of VRP minimum frequency and intensity were similar in the IONM and non-IONM groups. VRP minimum frequency and intensity values were increased at 2 weeks postoperatively compared with the preoperative values and then returned to preoperative levels by 6 months postoperatively (Table 3 and Fig. 1B and D).
Changes of voice range profile (VRP) in the intraoperative neuromonitoring (IONM) and non-IONM groups:
Data are mean ± standard deviation values.
VRP, voice range profile.
There was no significant difference in the mean change of VRP maximum frequency and intensity between the two groups (Table 4 and Fig. 1A and C). Also, there was also no significant difference in the mean change of VRP minimum frequency between the two groups (Table 4 and Fig 1B). However, there was a significant difference in mean change of VRP minimum intensity between the two groups postoperatively (P = .004) (Table 4) In the IONM group, there was significantly earlier recovery in VRP minimum intensity compared with the non-IONM group (Fig. 1D).
VRP, voice range profile.
Discussion
IONM has been proposed as an adjunct to standard visual identification of the laryngeal nerves during thyroid surgery. Several studies have shown the advantages of IONM on laryngeal nerve palsy or voice outcome. Frattini et al. 13 evaluated the role of IONM for thyroidectomy in papillary thyroid cancer. Their study was a retrospective series comprising 76 cases of thyroidectomy alone (non-IONM group) versus 76 cases of thyroidectomy with IONM. The overall RLN morbidity was 3.9% in the IONM group and 9.2% in the control group (P < .05). There were 2 cases of permanent RLN palsy (2.6%) in the control group, one in the IONM group (1.3%), and one case of bilateral RLN injury in the control group. The incidence of temporary permanent RLN palsy in the IONM group was 2.6% versus 6.5% in the control group. These results proved that IONM is an effective adjunct for RLN preservation during thyroidectomy in thyroid cancer patients.
A recently published prospective randomized trial by Dionigi et al. 17 examined the use of IONM during video-assisted thyroidectomy. This study enrolled 72 patients divided into two groups of 36 each. This research asserted that neuromonitoring during video-assisted thyroidectomy is effective in providing identification and preserving function of the RLN and that IONM can enable surgeons to feel more comfortable with their approach to video-assisted thyroidectomy. 17 These authors have demonstrated that the IONM method improved identification of the EBSLN in video-assisted thyroidectomy: EBSLN was better identified in the IONM group than in the control group without IONM (P < .05). 17
To our knowledge, this is the first prospective randomized series of patients undergoing robotic thyroidectomy with the use of IONM.
In the present prospective controlled study, voice outcomes between two robotic thyroid surgery groups—with IONM and without IONM—were compared. Our results showed that there were no significant differences in voice outcomes between the IONM and non-IONM groups in terms of VHI scores, laryngoscopic findings, or VRP maximum frequency, intensity, and minimum frequency. However, there was a significant difference in mean change of VRP minimum intensity between the two groups postoperatively. In the IONM group, there was significantly earlier recovery in VRP minimum intensity compared with the non-IONM group. This finding indicates that IONM can be a helpful and effective tool to preserve voice outcome after robotic thyroidectomy. Previously, in our institution, we did not routinely use IONM during thyroid surgery. We only used IONM during thyroid surgery with difficult cases for identifying RLNs. The stimulator itself is useful to indicate the correct plane of dissection, giving constant information during operation of laryngeal nerve function. In particular, we used the stimulator under optical guidance continually both prior (identification) and during (monitoring) the neural dissection of the tracheoesophageal groove.
In both groups, the main difference of the surgical procedure is the identification of RLNs. In the non-IONM group, the surgeon could manipulate more around RLNs than in the IONM group. This could relate to the good voice outcome in the IONM group. On the other hand, there was controversy about routine usage of IONM because the nerve stimulation could be the reason of nerve fatigue and increased incidence of temporary or permanent RLN palsy. Until now, several studies concluded that nerve stimulation with low pulse stimulation of 0.5–1.0 mA is safe for RLN function.8–10
The present study started to evaluate the efficacy of routine usage of IONM in thyroid surgery, especially in robotic surgery. In spite of several limitation of this study, we can observe the usefulness of routine usage of IONM for good voice outcome after robotic thyroid surgery through this study. To probe these results determinately, a larger number of randomized controlled studies is needed. Also, the high cost of the system for IONM is an important problem to be surmounted.
In the results of the present study, VRP minimum frequency and intensity were statistically different between the two groups preoperatively. As noted, the non-IONM group included 19 women and 6 men, whereas the IONM group included 23 women and 2 men. Thus, this difference may have been related to the higher number of male patients in the non-IONM group.
We performed robotic thyroidectomy using the bilateral axillo-breast approach by a da Vinci Surgical System in all cases. The use of robotic instruments may allow superior cosmetic results and can overcome limitations of endoscopic thyroid surgery such as an inadequate surgical view and inaccurate instrument manipulation. The robotic system provides a magnified, high-resolution, three-dimensional surgical view, a tremor filtration system, fine motion scaling, and precise and multi-articulated motion of innovative instruments. 21 These features are useful for identifying nerves and manipulation of the thyroid. We believe that the precision technology of robotic instruments with complementary IONM reduces the risk of nerve injury.
This study might be useful because it includes a prospective randomized series of patients undergoing robotic thyroidectomy with the use of IONM. Moreover, the power of our study may lie in the research protocol, which was characterized by a meticulous selection of patients for robotic thyroidectomy, which ensured homogeneity in both groups. We chose a standardized technique adapted from a study by Dionigi et al. 17 to identify and assess the function of the laryngeal nerves with IONM during operation. Our study showed slightly different results than others in that there was no statistically significant difference except for VRP minimum intensity observed between the two groups. We believe the reasons for this are as follows. First, we enrolled a small number of patients because of limitations due to the high cost of robotic surgery, and further larger trials are warranted in the future. Second, the precision of the robot itself may have prevented nerve damage, in accordance with the aforementioned advantages of robotic surgery.
Conclusions
IONM is feasible and reliable in minimally invasive thyroid surgery, and in this study the mean difference of VRP minimum intensity was more rapidly recovered in the IONM group than in the non-IONM group.
Footnotes
Acknowledgments
The research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (grant 2012R1A1013413).
Disclosure Statement
No competing financial interests exist.