
Abstract
Abstract
Objectives:
Urachal anomalies typically arise from abnormalities in the process of urachal closure. Urachal pathology causes morbidity (pain, umbilical drainage) and may harbor malignancy. Robotic-assisted laparoscopic surgery may be an attractive alternative to the open approach, which has only been studied in rare case reports. Herein, we report our experience with robotic surgery for benign urachal anomalies.
Materials and Methods:
From 2007 to 2013, we identified 11 patients (8 adult, 3 pediatric) who underwent robotic-assisted laparoscopic surgery for urachal pathology. Surgery was performed with a transperitoneal approach with careful dissection starting lateral to the median umbilical vessels, ensuring removal of all urachal tissue from the umbilicus to the bladder. When necessary, cystoscopic evaluation was performed to assist with the intravesical dissection. Patient demographics, postoperative narcotic use (morphine milligram equivalents), pathologic data, and operative time were evaluated.
Results:
There were 4 female and 7 male patients with a median age of 51 years (range, 12–72 years). Median operative time was 85 minutes (range, 51–224 minutes), and median blood loss was 20 mL (range, 5–400 mL). Only 6 patients required narcotics for pain control postoperatively, with a median of 7.5 mg of peroral morphine used. Median length of hospital stay was 1 day (range, 1–2 days), and median duration of catheterization was 5.5 days (range, 1–10 days). One patient underwent concurrent robotic prostatectomy. Pathology was benign in all cases. Median follow-up was 15.5 months (range, 1–18 months). Surgery was well tolerated as only 1 patient had a complication (Clavien class 1; a urinary tract infection treated with oral antibiotics).
Conclusions:
Urachal pathology is well suited to robotic-assisted laparoscopic surgery. The urachus is immediately visualized upon entry into the abdomen. The procedure can be performed safely, with short hospitalization and minimal narcotic pain control required.
Introduction
T
Previously, open management was advocated to ensure wide local excision of the umbilicus and a cuff of bladder. However, as more benign lesions have been diagnosed, an effort has been made to decrease the morbidity of this aggressive approach. Accordingly, laparoscopic and minimally invasive techniques have been popularized for urachal excision, beginning in the early 1990s. 4 However, laparoscopic excision may prove difficult, particularly if portions of the bladder and/or umbilicus need to be removed with the specimen. With the increasing popularity of robotic-assisted laparoscopic surgery, urologists have quickly applied the same techniques used for radical prostatectomy and other complex pelvic surgeries to the excision of urachal anomalies. We report our experience with robotic-assisted laparoscopic surgery for urachal anomalies.
Materials and Methods
After receiving approval from the Institutional Review Board, we reviewed medical records of all patients who underwent robotic surgery for an urachal anomaly. From 2007 to 2013, we identified 11 patients (8 adult, 3 pediatric) who underwent robotic-assisted laparoscopic surgery for urachal pathology. All patients underwent a complete evaluation, including history and a physical, as well as laboratory testing and radiographic imaging. All patients were advised of different forms of treatment, including the open and the minimally invasive/robotic approach. If there was concern regarding potential malignancy, frozen sectioning was performed, and patients were counseled about complete umbilectomy and pelvic lymphadenectomy if malignancy was encountered.
When necessary, cystoscopic evaluation was performed to assist with the intravesical dissection. Patients were placed in the lithotomy position, and after placement of a urethral catheter, pneumoperitoneum was established via a Veress needle. In adult patients, a 12-mm trocar was placed supraumbilically with an additional two 8-mm robotic trocars placed in a lateral position, approximately 8 cm lateral to the 12-mm port. One assistant port was placed lateral to one of the 8-mm trocars. In 1 pediatric patient an incision was made directly through the umbilicus, and an 8.5-mm insufflating camera trocar was under direct vision. An additional two robotic trocars were placed inferior to the Pfannenstiel line and medial to the anterior superior iliac spine (Fig. 1).
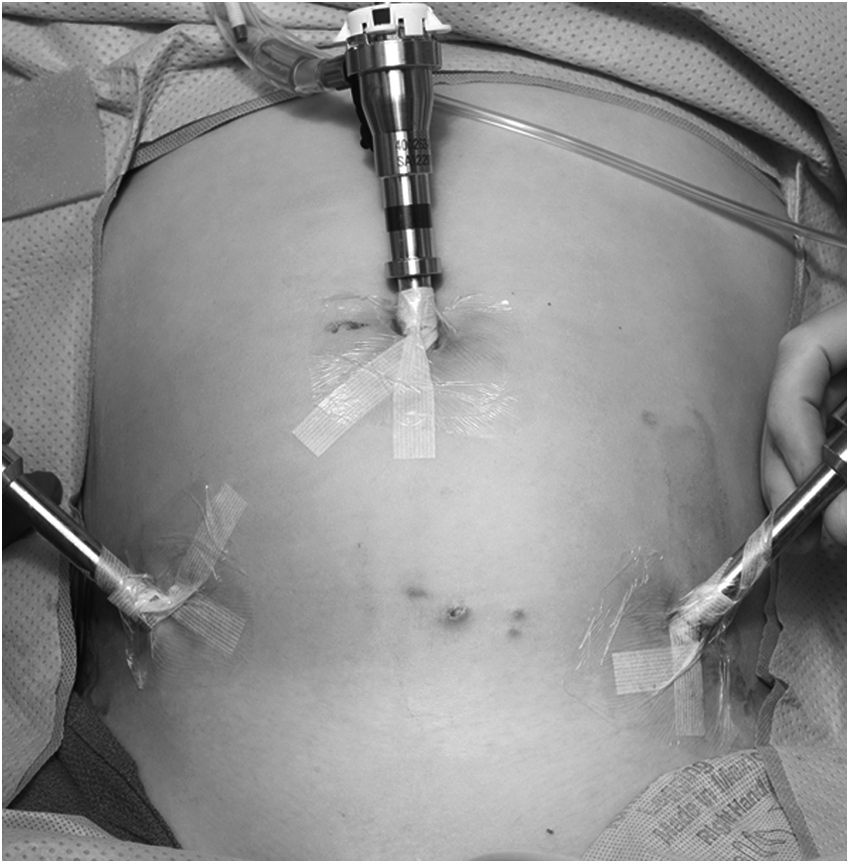
Port placement of a robotic urachal cyst excision in a pediatric patient.
Surgery was performed with a transperitoneal approach with careful dissection starting lateral to the median umbilical vessels, ensuring removal of all urachal tissue from the umbilicus to the bladder. The specimen was removed with use of an Endo Catch™ device (Covidien, Mansfield, MA). The pathologic specimen was sent for frozen sectioning if there was any concern for malignancy. If a cystotomy was performed, the bladder was closed in two layers with 2-0 polyglactin 910 (Vicryl®; Ethicon, Somerville, NJ) suture in a running fashion. All catheters were irrigated to ensure a watertight closure.
Patients were observed postoperatively and placed on a clear liquid diet and advanced as tolerated. Patients were administered a combined regimen of ketorolac, acetaminophen, and narcotic pain control as needed depending on the severity of postoperative pain. A cystogram was performed at between 7 and 10 days postoperatively if bladder closure was required. Patient demographics, postoperative narcotic use (peroral morphine milligram equivalents), pathologic data, and operative time were evaluated.
Results
We identified 4 female and 7 male patients who underwent a robotic-assisted excision of a urachal anomaly. The median age of these patients was 51 years (range, 12–72 years). Of these patients, 4 (36%) presented with symptomatic urachal problems, several with more than one: periumbilical drainage in 1 (25%), abdominal pain in all (100%), and infection in 4 (100%). The rest (n=7; 64%) were identified incidentally on imaging for other causes.
Median operative time was 85 minutes (range, 51–224 minutes), and median blood loss was 20 mL (range, 5–400 mL). Only 5 patients required narcotics for pain control postoperatively with a median of 7.5 mg of peroral morphine used. Median length of hospital stay was 1 day (range, 1–2 days), and median duration of catheterization was 5.5 days (range, 1–10 days). One patient underwent concurrent robotic prostatectomy. One patient required partial cystectomy. Pathology was benign in all cases (Table 1). Median follow-up was 15.5 months (range, 1–18 months). Surgery was well tolerated as only 1 patient had a complication (Clavien class 1; a urinary tract infection treated with oral antibiotics). At the most recent follow-up all symptoms had resolved, and no revisions were required.
F, female; M, male; Pca, prostate cancer; PO, peroral.
Discussion
The allantois initially is contiguous with the urinary bladder but upon constriction becomes a thick fibrous cord: the median umbilical ligament in adults or the urachus in the fetus.5–7 The urachus plays no role in bladder development in humans but is thought to act as a reservoir in lower vertebrates. The cloaca, which forms the future urinary bladder in humans, descends toward the pelvis, elongating the urachus and contracting the tube, which becomes an extraperitoneal, fibromuscular band shortly after birth.5,6
If the urachus does not elongate sufficiently to obliterate the inner lumen, urachal pathology can arise, leading to significant morbidity in both the adult and pediatric populations. Urachal anomalies are classified based on the location to the urinary bladder.7,8 Most common in the pediatric population is the patent urachus, present in 50% of symptomatic urachal anomalies, presenting typically with umbilical drainage and periumbilical inflammation. A urachal cyst is present in 30% of symptomatic cases and can present with abscess formation (Fig. 2) and systemic inflammatory response syndrome. Additionally, patients can present with localized lower abdominal pain, voiding symptoms, or even a painful, palpable mass. The umbilical–urachal sinus can present in a similar fashion to the patent urachus but does not communicate directly with the urinary bladder and presents in roughly 15% of cases. Lastly, a urachal diverticulum, found in 3%–5% of cases, can present asymptomatically from imaging or with lower urinary tract symptoms (incomplete bladder emptying, urinary tract infection, urolithiasis). 8

Cross-sectional imaging of an infected urachal cyst in a 12-year-old patient.
The first reported series of minimally invasive urachal surgery was reported by Trondsen et al. 4 in 1993 with the removal of a urachal sinus. Subsequent to the initial description there have been multiple case reports with several case series describing various laparoscopic techniques for removing urachal pathology in adults and children, which were demonstrated to be safe and efficacious.9–12 Madeb et al. 13 described the initial experience with robotic-assisted laparoscopic surgery on the urachus in a case series of 5 patients with varying urachal pathology, including malignancy. They described styles of port placement with four or five working ports, depending on the extensiveness of the procedure. Blood loss was minimal, with a mean of 118 mL, and operative times were slightly longer than our series, ranging between 120 and 300 minutes for partial cystectomy with urachal excision.
Although previous series focused primarily on patients presenting with symptomatic urachal pathology, in our series only 3 of 11 patients presented with symptoms. Naiditch et al. 14 evaluated pediatric urachal anomalies, and in the series of 103 patients, 18 were asymptomatic and were observed; only 8 patients were followed up, with 7 on repeat imaging demonstrating resolution of the urachal remnant. When patients were symptomatic and underwent excision, approximately 50% underwent minimally invasive excision; however, only 3 (8.8% of operative group) patients underwent robotic-assisted excision. The complication and re-operation rate of the entire operative group was 14.7%. 14
In our series of both adult and pediatric patients, all pediatric patients presented with symptoms that resolved postoperatively. Ashley et al. 3 reviewed a large series of both adult and pediatric patients with urachal remnants from a single institution. They identified 176 patients (130 adults, 46 pediatric) with urachal remnants over a 54-year period. Children more commonly presented with umbilical drainage and pain, whereas adults presented with hematuria and pain. In all, 51% of adults were diagnosed with malignancy. In multivariate analysis only hematuria and age >55 years were significant predictors for malignancy. 3 The authors' recommendations included excision of all urachal pathology because of the unknown risk of cancer and the poor prognosis of urachal carcinoma.
In our series we identified 8 adults and 3 children with urachal anomalies who underwent excision. Patients were discharged a median of 1 day postoperatively, and only 1 patient experienced a complication: a urinary tract infection requiring oral antibiotics (Clavien class 1). No patients required a re-operation. Patients were counseled preoperatively regarding risk for malignancy and need for completion umbilectomy if frozen section demonstrated urachal carcinoma. As no patients had malignant pathology, the umbilicus was spared in all cases, leading to a better cosmetic result for all patients. Patients had minimal pain control requirements, with a median of 7.5 mg of oral morphine required. There were 5 patients who required no narcotic pain control postoperatively.
We acknowledge the inherent weaknesses of a retrospective study and have a limited number of patients as urachal anomalies are quite rare. In addition, we recognize that our center is a tertiary referral facility, and thus our results are not generalizable.
Conclusions
Urachal pathology is well suited to robotic-assisted laparoscopic surgery. The urachus is immediately visualized upon entry into the abdomen. Umbilectomy can be avoided if frozen-section pathology demonstrates no evidence of malignancy in the operative specimen. The procedure can be performed safely, with short hospitalization and minimal narcotic pain control required.
Footnotes
Disclosure Statement
No competing financial interests exist.