
Abstract
Abstract
Objective:
To describe a novel surgical technique, laparoscopic stepwise-cut double initial stay suture (LASDISS) pyeloplasty for ureteropelvic junction obstruction (UPJO). Additionally, we evaluated the safety and short-term results.
Materials and Methods:
This was a nonrandomized study with a series of 6 patients with UPJO, operated on between March 2012 and August 2013. Perioperative and short-term outcomes were evaluated. In brief, a “T shape cut” was performed from the dilated pelvis to the ureter. The initial stay suture was placed between the lower edge of the pelvis and the distal end of the spatulated anterolateral part of the ureter. The pelvis was closed with a continuous suture starting from the opened upper edge of the pelvis that was secured after leaving enough space for ureteral anastomosis. The second initial stay suture was placed after passing the ureter and pelvis two times. The dilated part of the renal pelvis and the stenotic segment were excised. A double-J stent was inserted. The remaining space between the two initial sutures was closed with these continuous sutures.
Results:
We performed the LASDISS pyeloplasty technique in all cases. Median operation time was 177 minutes (range, 100–290 minutes). Mean follow-up was 7.5 months (range, 3–18 months). The mean pre- and postoperative split renal function on diuretic renography was 33% (range, 25%–56%) and 42% (range, 30%–52%), respectively.
Conclusions:
The LASDISS pyeloplasty surgical technique represents a safe and effective option in surgical treatment of UPJO.
Introduction
U
On the other hand, the learning curve is one of the factors that certain modifications in the technique would help in overcoming some difficulties of laparoscopic pyeloplasty and minimizing the operative time and complications. Here we present our initial experience with a new laparoscopic surgical technique, termed laparoscopic stepwise-cut double initial stay suture (LASDISS) pyeloplasty, in a large-volume renal pelvis. We also evaluated the safety and perioperative and short-term outcomes of this technique.
Materials and Methods
Six patients with an intermittent flank pain (n=4) and decreasing unilateral renal function (n=2) were enrolled into the study. UPJO (3 in the right, 3 in the left) was diagnosed in all patients. Patients' mean age was 34.5 years (ranging between 13 and 45 years). Four patients were male, and 2 were female. LASDISS pyeloplasty was performed by the retroperitoneal route in 5 patients and the transperitoneal route in a 13-year-old boy. The selection criterion was primary intrinsic stenosis, especially with dilated pelvis. In 1 patient with concomitant renal stones, laparoscopic pyelolithotomy was also performed. Preoperative differential renal function, operative time, postoperative complications (pain, drain output, fever), hospital stay, and renal functions were recorded. Complications were assessed by using modified Clavien–Dindo classifications. 13 Patients were assessed with ultrasonography 6 weeks after LASDISS, and a diuretic renogram was performed 3 months after surgery. A complete physical examination was also performed in every clinical visit. Treatment success was defined as symptomatic relief with either stable or improved renal function or improved washout shown on diuretic renogram or excretory urography, when the postoperative renal functions were higher than preoperative ones.
Surgical technique
All retroperitoneal procedures were performed in the flank position, and the transperitoneal case was performed in the supine position. As Gill and Rassweiler 14 described, access to the retroperitoneal space was obtained with the open technique through a 1.5-mm subcostal incision performed at the tip of the petit trigon, at first. A 10-mm balloon dilating trocar (Herloon®; Aesculap Division, BBraun AG, Tuttlingen, Germany) was used for providing adequate working space. Then a 10-mm trocar was placed. It was fixed to the musculature with a purse-string suture in order to avoid air leakage and development of subcutaneous emphysema. Two additional trocars were placed under visualization: a 5-mm (left-hand side) trocar on the hemiclavicular line, just above the iliac spine and caudally to the optics port, and a 10-mm trocar at the posterior axillary line, forming a triangle. The retroperitoneal space was dissected just over the fascia of psoas just parallel to the ureter. Thus, it enabled us to see the psoas easily for orientation, during the entire procedure. A longitudinal incision was made in Gerota's fascia, parallel and close to the psoas muscle, for accessing the ureteropelvic junction. A precise dissection in the upper side of the ureter and pelvis was performed until the renal parenchyma. These movements were also performed for revealing the exact cause of UPJO, and thus the lower and middle poles of the kidney were clearly identified. Adequate dissection of the renal pelvis led to easy reconstruction during the entire procedure. This was one of the main points of our surgical technique. The ureteropelvic junction was examined to see whether there was an aberrant artery or not. In all cases there was no aberrant artery. Our technique was only useful in primary intrinsic stenosis, especially with a dilated pelvis.
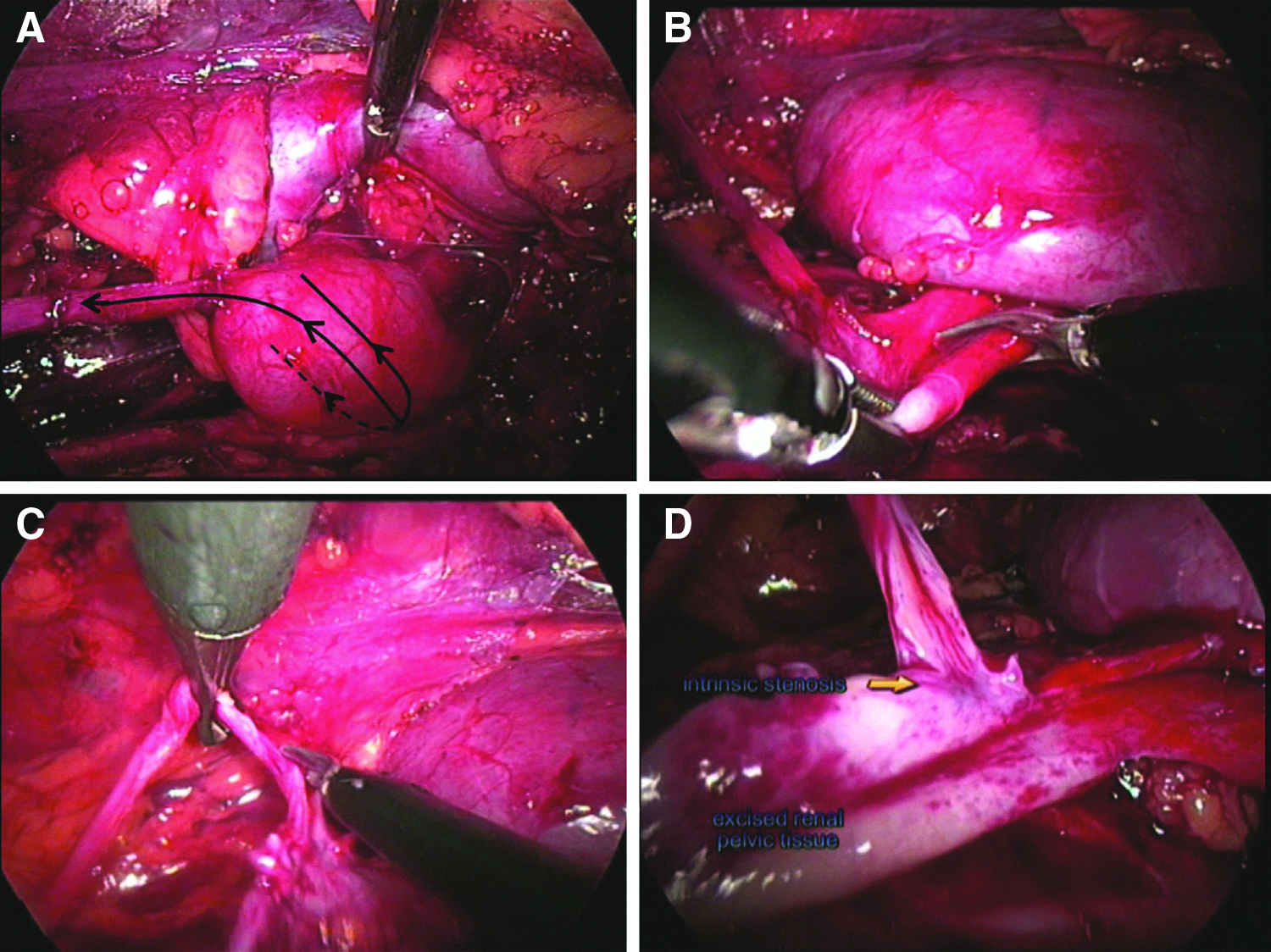
The first step included incision of the pelvis. A “T shape cut” was made to the pelvis and ureter (Fig. 1A). The incision began from the lateral side of the pelvis, which was close to the camera at the retroperitoneal space, and went to the stenotic segment (Fig. 1B). The incision was extended from the anterolateral side of the ureteropelvic junction to 2–3 cm distal to the ureter (Fig. 1C). Excessive pelvic tissue was cut. Then, the renal pelvis was redacted with the maintenance of the inferior–medial part of the pelvis and the superior–medial side of the ureter. Partial opening of the pelvis and ureter provided better visualization of the stenotic segment at the ureteropelvic junction (Fig. 1D).
Performing the laparoscopic stepwise-cut double initial stay suture: cutting
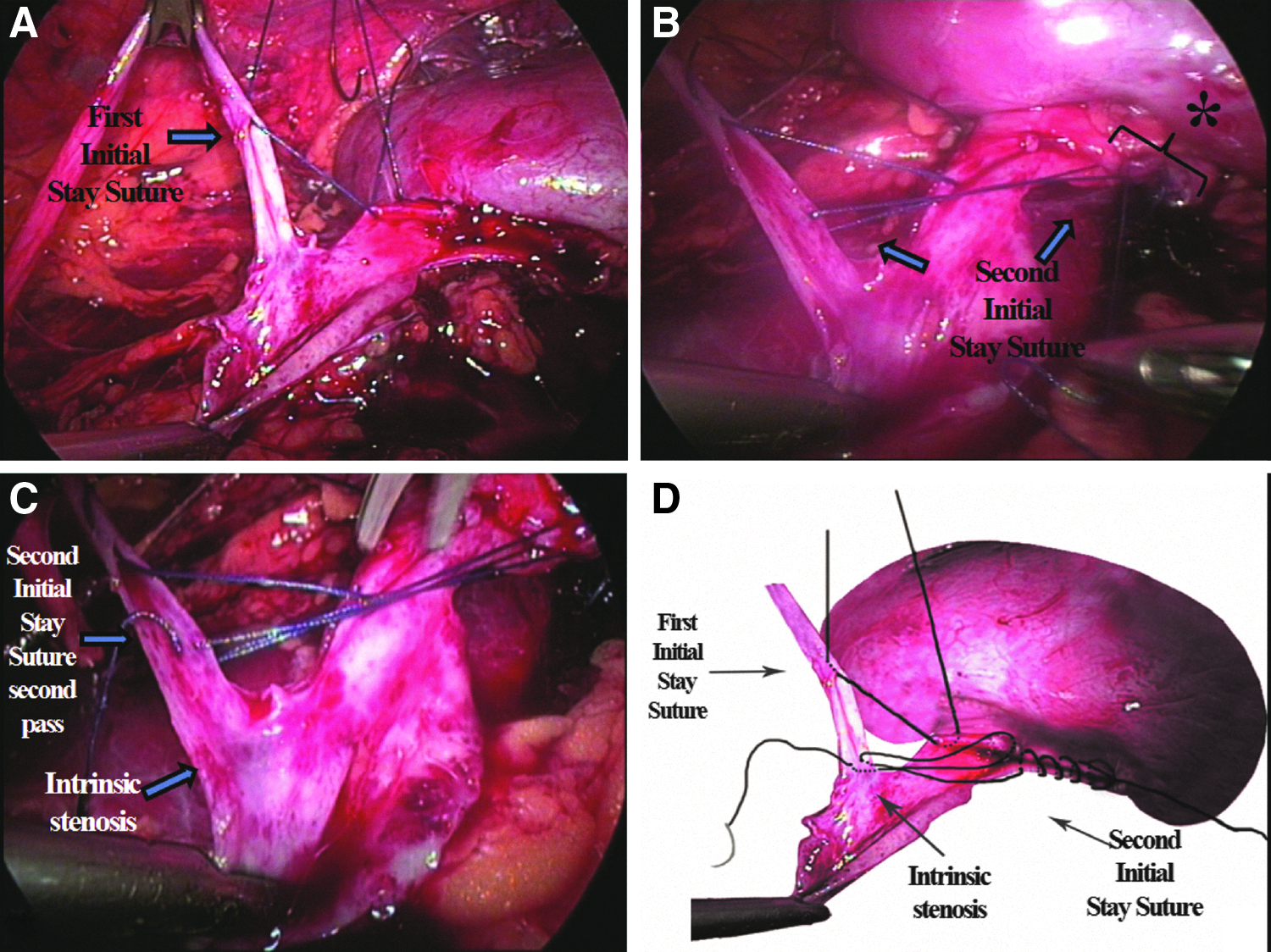
Before the ureter and pelvis were dismembered (complete excision of the intrinsic segment and dilated pelvis), the first initial stay suture was placed between the lower edge of the incised pelvis and the distal end of the spatulated anterolateral part of the ureter (Fig. 2A). Then the dilated pelvis was closed with continuous sutures using absorbable 4-0 suture (Fig. 2B). Continuous suturing was secured after leaving enough space for ureteral anastomosis. The same suture was placed at the longer edge of the ureter opposite to the spatulated part, just distal to the stenotic segment of the ureter, which will be excised (Fig. 2C and D). When conventional laparoscopic pyeloplasty is performed, losing the tension of the first suture is one of the major problems during the anastomosis. To overcome this problem, the second initial stay suture was placed after passing the ureter and pelvis two times. Therefore, the longer part of the suture was placed in the nonspatulated part of the ureter. At this step, the dilated part of the renal pelvis (Fig. 3A) and the stenotic segment (Fig. 3B) were excised. Then they were taken out from the distal part of the stenotic segment and proximal to the first initial suture. This allowed us to perform more accurate excision to the ureter (not too much or not too little).
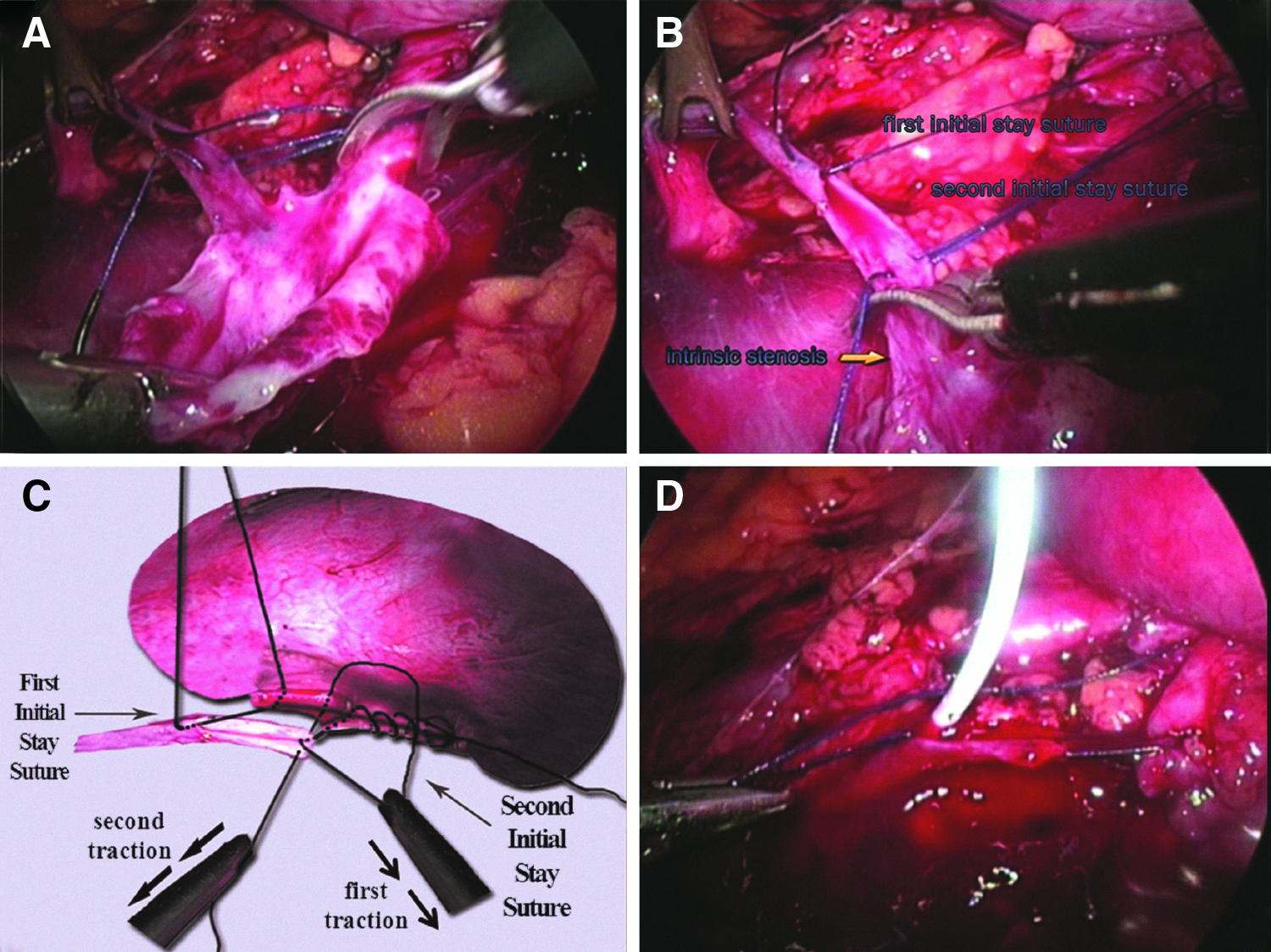
Excision of
Thereafter, the second initial suture was passed from the pelvis again. Thus, the first and second initial sutures had been placed. Sutures that had been passed two times from the pelvis and ureter were pulled one by one so that the tension was not lost (Fig. 3C). By this pulling system, the approached ureter and pelvis could not lose tension and locked together. A 4.7-French 26-cm double-J stent was placed first to the ureter and then to the renal pelvis through the 5-mm trocar intraoperatively over its guide wire (Fig. 3D).
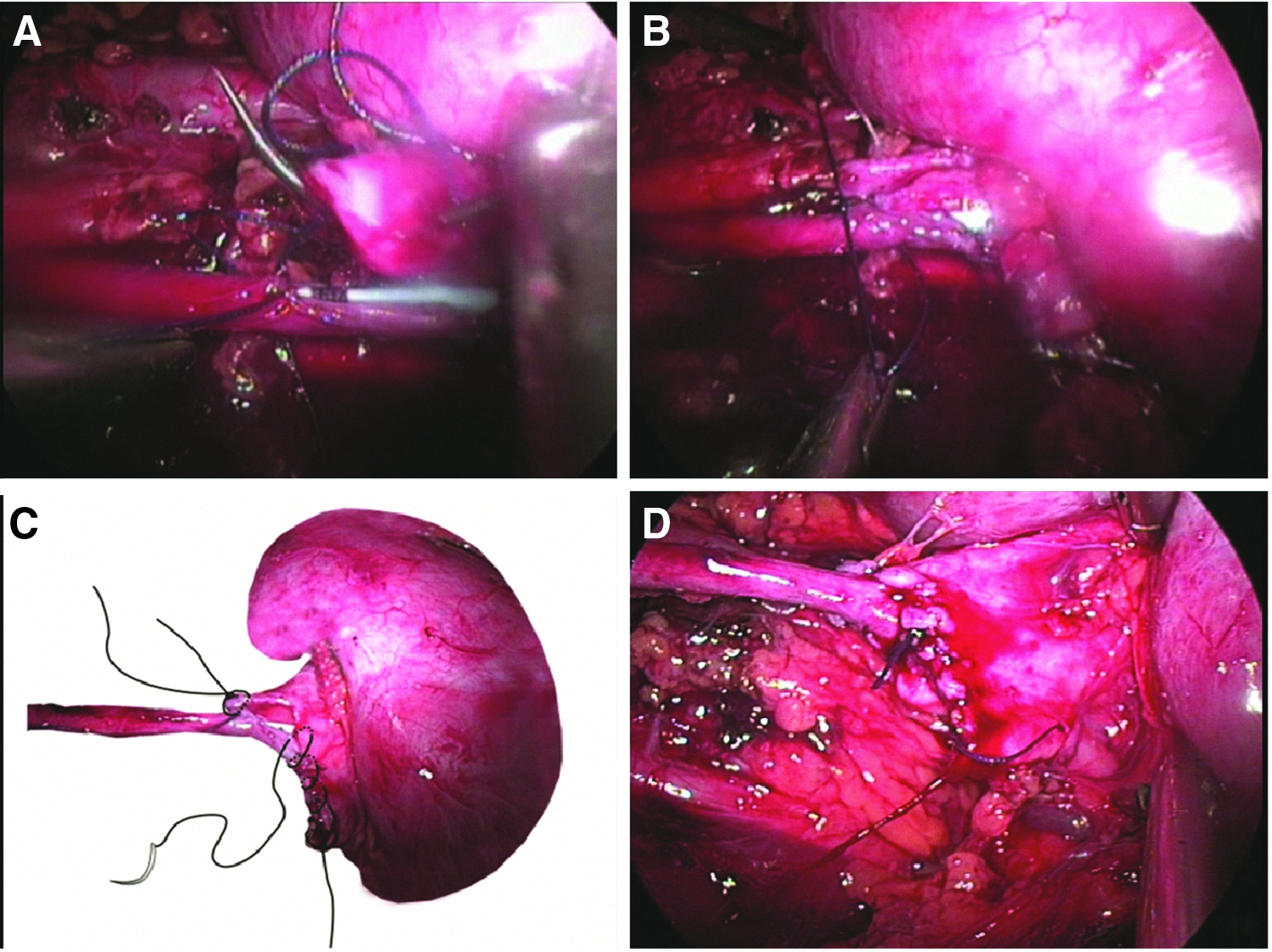
After the first initial stay suture at the spatulated part of the ureter was drawn near to the inferior edge of the incised renal pelvis, the second pass of the first initial stay suture was performed (Fig. 4A). Then, the knot was secured (Fig. 4B). Whether the spatulated ureteral part was completely connected to the incised pelvis was checked. After this step, the remaining space between the two initial stay sutures was closed with these continuous sutures. Whereas the first initial stay suture was taken to the starting point of the second initial stay suture, the second initial stay suture was taken to the starting point of the first initial stay suture (Fig. 4C). Both sutures were fixed with a knot, and the anastomosis was completed (Fig. 4D).
Results
All procedures were successfully performed by using the LASDISS pyeloplasty technique with retroperitoneal (n=5) and transperitoneal (n=1) approaches. Median operation time was 177 minutes (range, 100–290 minutes). All patients were discharged within 48 hours of surgery. Mean follow-up was 7.5 months (range, 3–18 months). All patients had improvement in symptoms, and the nuclear scan showed nonobstructive drainage in the postoperative period. The mean pre- and postoperative split renal function on diuretic renography was 33% (range, 25%–56%) and 42% (30%–52%), respectively. Additionally, there was significant improvement for t1/2 time in the postoperative compared with the preoperative period (P=.01). Our early results were very encouraging with no serious complications. However, 1 patient had ileus and was treated by medical management (Clavien Grade 1). In addition, 1 patient had minimal urinary leakage. She was followed up in our clinic, and we changed her double-J stent under fluoroscopy, with the patient under local anesthesia (Clavien Grade 3a). There was no Clavien Grade 4 or 5 complication. Overall, successful resolution of UPJO was observed in all cases.
Discussion
Laparoscopic pyeloplasty has been able to reproduce the high success rates of open pyeloplasty, while also achieving minimal morbidity. Despite excellent results, laparoscopic dismembered Anderson–Hynes pyeloplasty is hampered by difficulties during some steps, and the steep learning curve has hindered its use. 12 We performed a new modified Anderson–Hynes technique termed LASDISS pyeloplasty for overcoming these difficulties. Our technique had some advantages when compared with the conventional dismembered Anderson–Hynes technique.
One of these advantages was that we could demonstrate better visualization of the stenotic segment by partial opening of the pelvis and ureter. Before complete excision of the stenotic segment and dilated pelvis, placing initial stay sutures provided us excellent visualization. It also obviated the requirement of a fourth trocar. The conversion rate in the literature reported following anastomosis ranges between 0.5% and 5.5%. 15 These initial stay sutures were the basic sutures in the anastomosis and were easy to place with our technique. Therefore, it provided easier suturing of the anastomosis, which was presumed as very difficult in laparoscopic surgeries.
When conventional laparoscopic pyeloplasty is performed, losing the tension of first sutures is one of the major problems during the anastomosis. We sutured the ureter and pelvis two times, and the second suture allowed us to visualize the anastomosis, by using the LASDISS technique. This pulling system helped us also to approach and to lock the ureter and pelvis without relaxing. To incise the ureter and take it out required accurate excision of the ureter (not too much or not too little). Thus, maximum ureter length could be obtained.
This incision can also allow us to access the lower calyces and pelvis for removing stones. Kumar and Mandhani 16 described their surgical technique for avoiding rotation of the ureter during laparoscopic pyeloplasty. In our technique, we used initial stay sutures before cutting the ureter, and these prevented unrecognized rotation of the ureter, before anastomosis.
Ureteral stent placement is a necessary step that may necessitate additional procedures and/or radiation exposure for placement and confirmation of the stent location. El-Feel et al. 17 concluded that inserting the double-J stent before the pyeloplasty procedure caused the operation time to be prolonged. Using the LASDISS technique, it can be easier to insert the double-J stent into the ureter preoperatively using unique patient positioning. It was performed simultaneously by using its guide wire without the need for repositioning the patient. The antegrade procedure is an easy-to-learn, safe, and reliable stenting technique using the parallel axis of the ureter and trocar. It may obviate the problem while inserting the stent in the renal pelvis during dissection and suturing. Moreover, the surgeon may need to change the patient's position to the flank position for the laparoscopic procedure. 18
Approximately 20% of kidneys have multiple renal arteries, 19 and an accessory crossing vessel is most likely the etiology of UPJO (38%–71%). 20 As we were able to perform this technique (placing the initial stay sutures before excision of the stenotic segment and dilated pelvis) only for those cases whose etiologies were pure intrinsic stenosis (absence of crossing vessels) with a large-volume pelvis, the number of cases is limited. Besides this, the follow-up time was not enough to be able to compare our results with series with long-term follow-up.
Conclusions
Although laparoscopic pyeloplasty is technically demanding, it is emerging as a viable, minimally invasive alternative to open pyeloplasty for UPJO with a success rate similar to that of open pyeloplasty. Our new laparoscopic pyeloplasty technique, the LASDISS pyeloplasty, can provide surgeons with a way to treat UPJO safely and effectively with a surgical technique that is easy to learn and to perform. These favorable initial results justify further exploration of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.