
Abstract
Abstract
Introduction:
Diagnosis of metastatic breast carcinoma to the internal mammary lymph nodes is important both as a prognostic factor and for planning adjuvant chemoradiotherapy. Establishing lymph node dissection is often performed by Chamberlain's procedure, which involves intercostal incision with spreading of the pectoralis and the intercostal muscles and can be associated with complications, including bleeding from the internal mammary artery or damage to intercostal vessels and nerves. A technique is presented for video-assisted thoracoscopic internal mammary node dissection using both sentinel node evaluation and dissection.
Patients and Methods:
This technique was performed on 2 female patients undergoing internal mammary node evaluation after they presented with invasive ductal breast carcinoma.
Results:
Video-assisted dissection of the thoracoscopic internal mammary lymph nodes was successfully performed with no intraoperative complications. The postoperative course was uneventful.
Conclusions:
This approach can avoid damage to the internal mammary artery and intercostal spaces while providing useful information for the guidance of further therapy and achieving local control if clinically indicated.
Introduction
A
Patients and Methods
We performed a video-assisted thoracoscopic technique for IMN dissection and evaluation in 2 female patients diagnosed with invasive ductal breast carcinoma.
Case 1
A 65-year-old woman with history of left-sided invasive ductal breast carcinoma presented with local recurrence 2 years after lumpectomy and negative sentinel axillary lymph node biopsy. Positron emission tomography (PET)–computed tomography (CT) revealed PET-positive, enlarged ipsilateral IMNs (Fig. 1A).
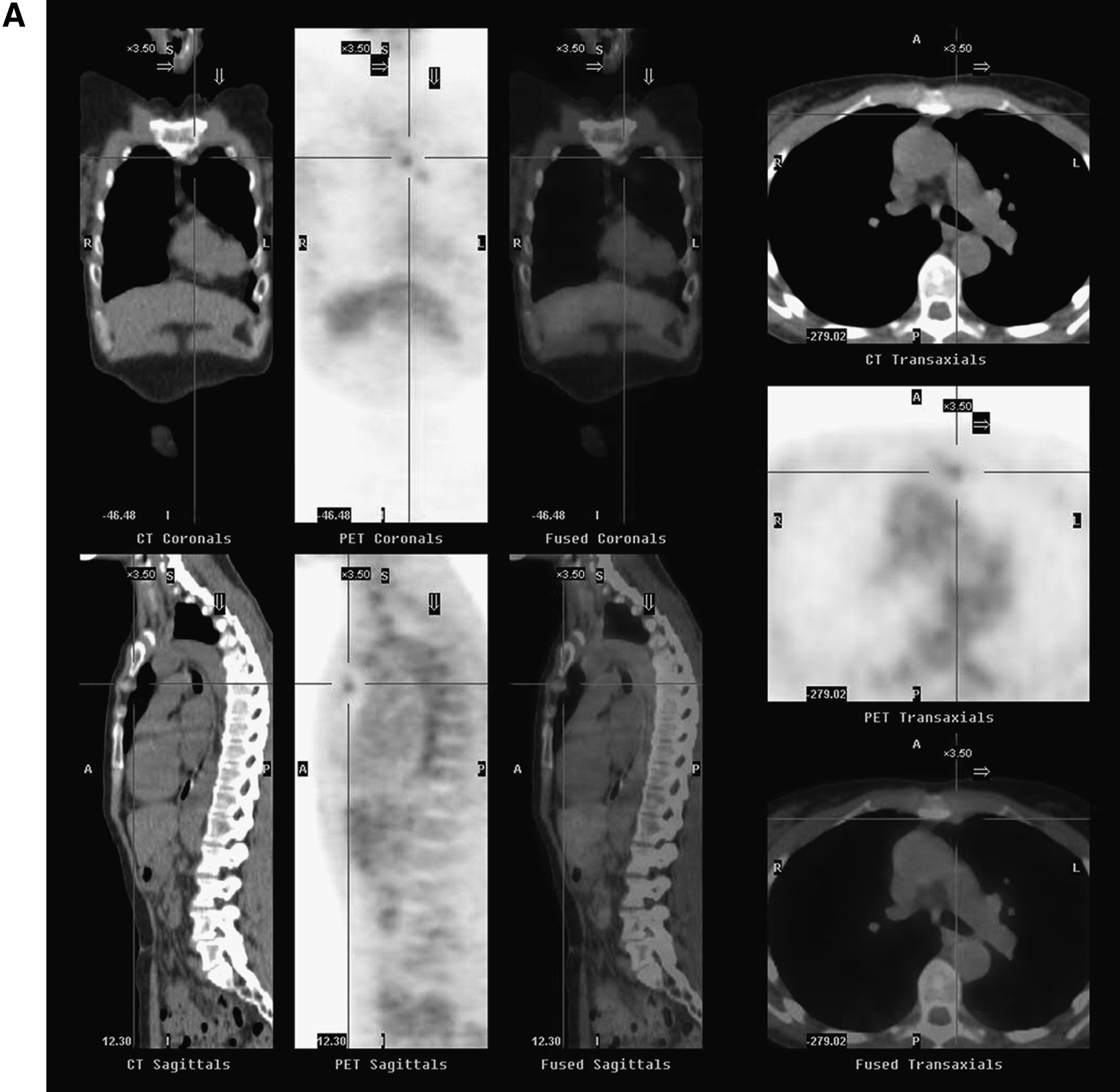
Breast magnetic resonance imaging and positron emission tomography (PET)–computed tomography (CT) showing PET-positive, enlarged ipsilateral internal mammary nodes.
Case 2
A 63-year-old woman presented with left-sided invasive ductal breast carcinoma and PET/CT positivity of IMNs (Fig. 1B). The patient underwent neoadjuvant chemotherapy with excellent response and no evidence of uptake on follow-up imaging.
Surgical technique
Both patients underwent preoperative lymphoscintigraphy to aid in the identification of the IMNs and axillary lymph nodes. 2 Only 1 patient showed areas of high radioactivity, which were marked preoperatively by the radiologist and confirmed by gamma probe. Patients were positioned supine with the arm perpendicular on a support board, and general double-lumen endotracheal tube anesthesia was induced. Sterile draping was performed so the sternum, clavicle, and anterior axilla were exposed and accessible.
Case 1 underwent a standard mastectomy, repeat axillary lymph node dissection, and IMN dissection. Mammary nodes were able to be localized both by the gamma probe trans-sternally and by gross visualization. The lung was rendered atelectatic, and a 3-mm port and 30° videoscope were introduced into the left ipsilateral thorax from the anterior axilla at the fourth intercostal chest space. A second 5-mm port was placed in the third intercostal space (Fig. 2A). The internal mammary artery and the IMNs were easily visualized. A biopsy forceps was used to remove the grossly enlarged and adjacent IMNs (Fig. 2B). There was no residual gamma positivity remaining in this region after removal of nodes. The pneumothorax was evacuated with a suction catheter, and the lung was re-insufflated.
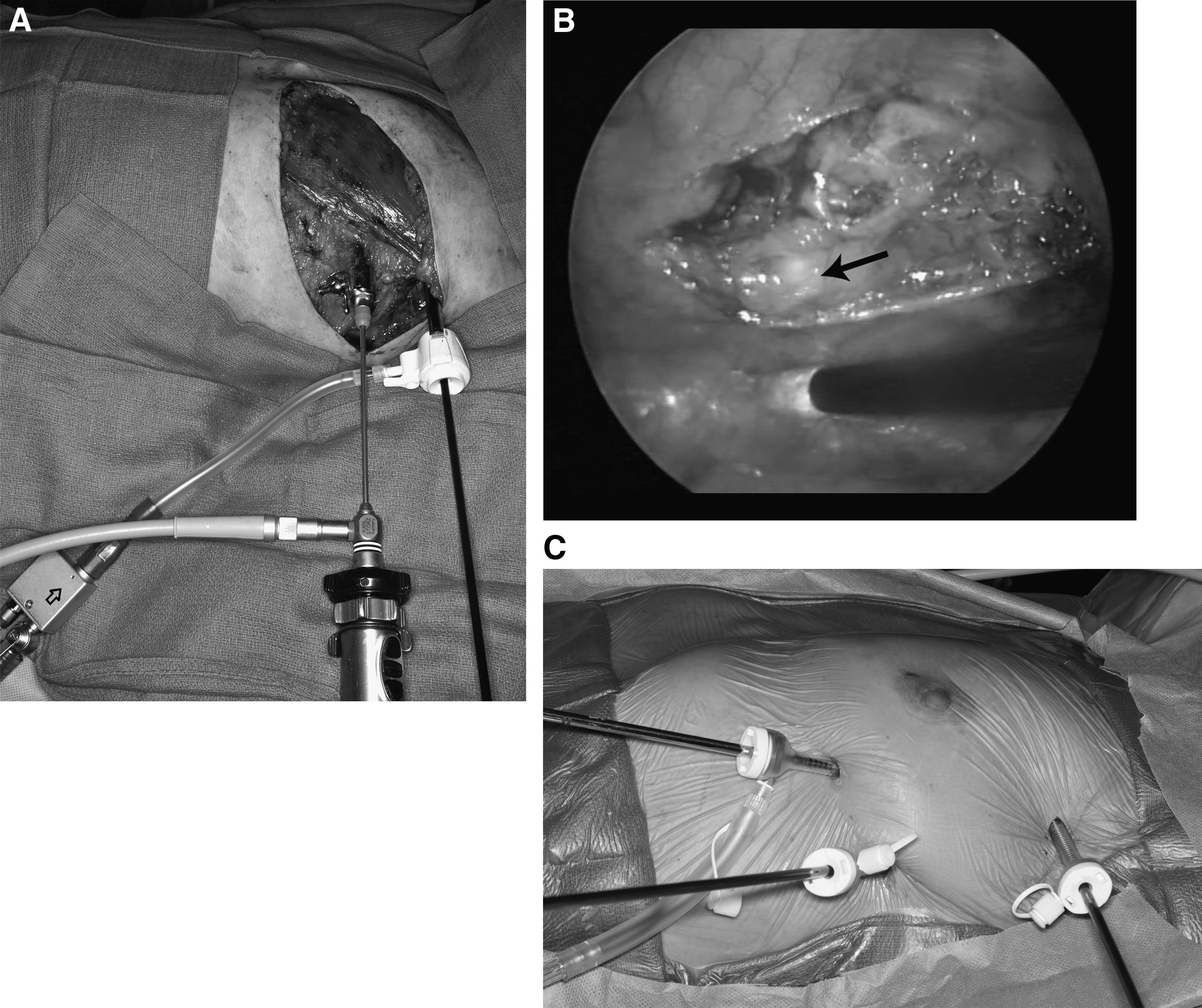
Case 2 had no accumulated gamma activity; therefore methylene blue was injected into the tumor site intraoperative prior to resection. A segmental mastectomy and axillary dissection was performed followed by IMN dissection. A 5-mm port was first inserted in the fourth intercostal space, and the camera was introduced. No blue uptake was noted in the IMNs; therefore full dissection of the mammary chain superior to the seventh rib was undertaken. Two additional 5-mm ports were placed in the third and fifth intercostal spaces (Fig. 2C). All fat and nodal tissue were resected along the artery and sent as specimens. A 16-French chest tube was placed through the lower port and left overnight because of mild serosanguineous drainage from the IMN dissection site.
Results
IMNs were easily identified and dissected with the use of video-assisted thoracoscopy.
The pathology in Case 1 revealed a 0.9-cm, poorly differentiated, invasive ductal cell carcinoma with none of three axillary sentinel lymph nodes involved and two of six IMNs. The patient subsequently underwent adjuvant chemotherapy and radiation.
The pathology in Case 2 revealed neoadjuvant therapy changes consistent with treated residual tumor in the left breast specimen. Axillary sentinel lymph nodes and all IMNs showed no evidence of viable tumor. Postoperative radiation therapy to the residual breast tissue was performed.
There were no intraoperative complications, and both patients were discharged on postoperative Day 2 after uneventful hospitalization.
Discussion
Internal mammary lymph nodes can be the site of metastatic breast cancer in a small percentage of patients. 3 Many surgeons prefer not to evaluate the IMNs because of several reasons, including their location and the risk of tumor seeding, which may further worsen the patients' prognosis. Additionally, previous studies have failed to prove any clinical significance in regard to patients' survival after the IMNs removal, and also because these nodes are seldom the first site of recurrence.2,4,5 However, recent studies have shown the prognostic value and significance of evaluation of IMNs, as well as their underestimation and not considering the appropriate adjuvant therapy could lead to a worse outcome.2–5
Dissection and identification of these nodes can be safely performed with the use of video-assisted thoracoscopy. Up to 45% of breast cancer patients demonstrate drainage to the IMNs by using lymphoscintigraphy. 2 The first case had positive gamma uptake, and the abnormal nodes with uptake were easily identified. The second case had excellent response to preoperative chemotherapy, and no nodal uptake was identified; therefore, complete dissection of all nodal tissue along the mammary artery was performed. No significant complications were observed.
We present a minimally invasive modality with video-assisted thoracoscopic surgical approach that allows excellent visualization and assessment of IMNs. This technique requires two or three lateral ports and is an alternative approach to the standard anterior Chamberlain's procedure. 3 Direct thoracoscopic visualization from a lateral view avoids the more generous anterior spreading of the pectoralis and intercostal muscles and may increase nodal harvest. An additional benefit may be a lower risk of damage to the internal mammary artery and/or intercostal nerves. 5 The video-assisted thoracoscopic approach to IMN dissection can provide useful histological information for the guidance of further therapy and achieve local control when clinically indicated.
Footnotes
Disclosure Statement
No competing financial interests exist.