
Abstract
Abstract
Background:
It is controversial whether preoperative obstruction in rectal cancers can affect prognosis or influence recurrence patterns. We investigated the association between endoscopic obstruction with survival and recurrence patterns in patients with locally advanced rectal cancers.
Materials and Methods:
An observational study and multivariate analysis were conducted to identify determinants of survival and to compare recurrence patterns between patients with obstructive or nonobstructive tumors after curative resection. Endoscopic obstruction was defined as a luminal obstruction of the rectum severe enough to prevent the colonoscope from passing beyond the tumor.
Results:
Cancer was obstructive in 91 patients (16.8%) and nonobstructive in 452 (83.2%). Median follow-up was 50 (range, 3–161) months. Local recurrence occurred in 17 patients (14 nonobstructed [5.4%] and 3obstructed [5.5%]; P=1.0) and systemic recurrence in 83 (62 nonobstructed [23.8%] and 21 obstructed [38.2%]; P=.042]). Endoscopic obstruction was a significant prognostic factor in stage III rectal cancers (P=.001) but not in stage II tumors. The multivariate analysis showed that endoscopic obstruction was an independent prognostic factor for overall survival, but not for disease-free survival, in patients with stage III rectal cancers. Endoscopic obstruction was associated with multiple-site systemic recurrence that was unsalvageable (salvageable surgery, 24 nonobstructed [40%] and 2 obstructed [10%]; P=.014).
Conclusions:
Endoscopic obstruction in patients with stage III rectal cancer predicted worse overall survival and was associated with multiple-site systemic recurrence.
Introduction
A
Materials and Methods
Patients
In total, 909 patients were treated for rectal cancer at Korea University Ansan Hospital (Gyeonggi-do, Republic of Korea) and Korea University Guro Hospital (Seoul, Republic of Korea) between January 2000 and December 2010. All patients had primary rectal adenocarcinoma that was located below 15 cm of the anal verge. Tumor stages were coded as described by the 7th edition of the American Joint Committee on Cancer tumor-node-metastasis (TNM) grading system. Inclusion criteria included patients with localized advanced rectal cancers (stages II and III) who underwent curative resection. Exclusion criteria were stage 0 patients (n=15), stage I patients (n=175), stage IV patients (n=85), undergoing local excision (n=22), loss to follow-up after the operation (n=14), colonic perforation (n=2), other cancers present (n=23), preoperative chemotherapy or radiotherapy (n=30). Patient demographics, tumor characteristics, and postoperative course were assessed. The types of rectal operations performed included low anterior resection, abdominoperineal resection, and Hartmann's resection. Total mesorectal excision was performed for tumors in the middle and distal rectum, whereas the mesorectum was excised at least 5 cm distal to the tumor for those in the upper rectum.
Endoscopic obstruction was defined as a luminal obstruction of the rectum severe enough to prevent the colonoscope from passing beyond the tumor, regardless of clinical signs of obstruction (abdominal distension, peristaltic abdominal pain, nausea, or vomiting) or radiologic findings of obstruction (dilated bowel loop).
The current standard care for locally advanced rectal cancers is to operate 6–8 weeks after the completion of chemoradiotherapy. However, except for low rectal tumors for sphincter-sparing surgery, clinical T4 disease, or lateral pelvic node positivity, surgeons in this study did not routinely perform preoperative chemoradiotherapy for locally advanced rectal cancers. This policy was in accordance with the growing evidence suggesting that a highly selective approach to the use of neoadjuvant chemoradiotherapy may be more appropriate than widespread application given concerns regarding toxicity and the lack of impact on overall survival (OS) rates. 8 Postoperative chemotherapy was generally applied to the patients with stage II and III tumors, if they did not have a severe comorbidity or refused further therapy, within 8 weeks after surgery. Six cycles of intravenous 5-fluorouracil/leucovorin as in the Mayo regimen was the most frequently administered chemotherapy, followed by oxaliplatin. Postoperative radiotherapy could be considered to the patients with T4 disease and significant nodal burden. A total dose of 50.4 Gy of pelvic radiation divided over 6 weeks in conjunction with concurrent chemotherapy was applied.
Follow-up studies consisted of a physical examination, digital rectal examination, and measurement of serum carcinoembryonic antigen (CEA) levels every 3 months for the first 2 years and biannually for the next 3 years. Chest radiography and abdominal/pelvic computed tomography were performed biannually for 2 years and then annually for 3 years. Colonoscopy was performed once every other year. If recurrence was suspected, patients were subjected to further diagnostic methods. Local recurrence was defined as clinical or radiologic tumor regrowth within the pelvic or operation field. Systemic recurrence was considered as tumor growth in any other area. We considered cases with local and systemic recurrence to be systemic recurrence cases. Further therapy for recurrence or metastasis included surgical resection, chemotherapy, or radiotherapy. The last follow-up was performed on December 16, 2013.
Statistical analysis
The chi-squared or Fisher's exact test was used to compare categorical data between obstructed and nonobstructed patients. Survival curves were estimated according to the Kaplan–Meier method, and statistical significance was tested by the log-rank test. Events were defined as rectal cancer recurrence or cancer-related death. Patients who were alive at the last follow-up were censored, as were patients who died of causes other than rectal cancer. A multivariate analysis was performed using the Cox proportional hazard model to determine the independent prognostic effect of preoperative obstruction after adjusting for confounding variables. All data were analyzed using SPSS version 15.0 software (SPSS, Inc., Chicago, IL), and P values of <.05 were considered significant.
Results
Overall, 543 patients with stage II (n=229) and stage III (n=314) cancer were included in the study. The median follow-up duration was 50 months (range, 3–161 months). Endoscopic obstruction occurred in 91 patients and nonobstruction in 452 patients. Among the 91 patients with obstruction, emergency ileostomy was initially performed in 2 patients and stent insertion in 14 patients. The remaining 75 patients were placed on a fast or a liquid diet without any decompression before elective resection. Compared with nonobstruction, endoscopic obstruction was related to a higher tumor location (P<.001), deeper tumor depth (P<.001), and higher preoperative CEA level (P=.010) (Table 1).
Data are number of patients (% of group).
T and N indicate pathological factors according to the 7th edition of the American Joint Committee on Cancer tumor-node-metastasis grading system.
ASA, American Society of Anesthesiologists; CEA, carcinoembryonic antigen.
Disease-free survival (DFS) at 5 years was 61% in the obstructed group compared with 74% in the nonobstructed group (P=.004) (Fig. 1a). OS at 5 years was 64% in the obstructed group compared with 82% in the nonobstructed group (P<.001) (Fig. 1d).
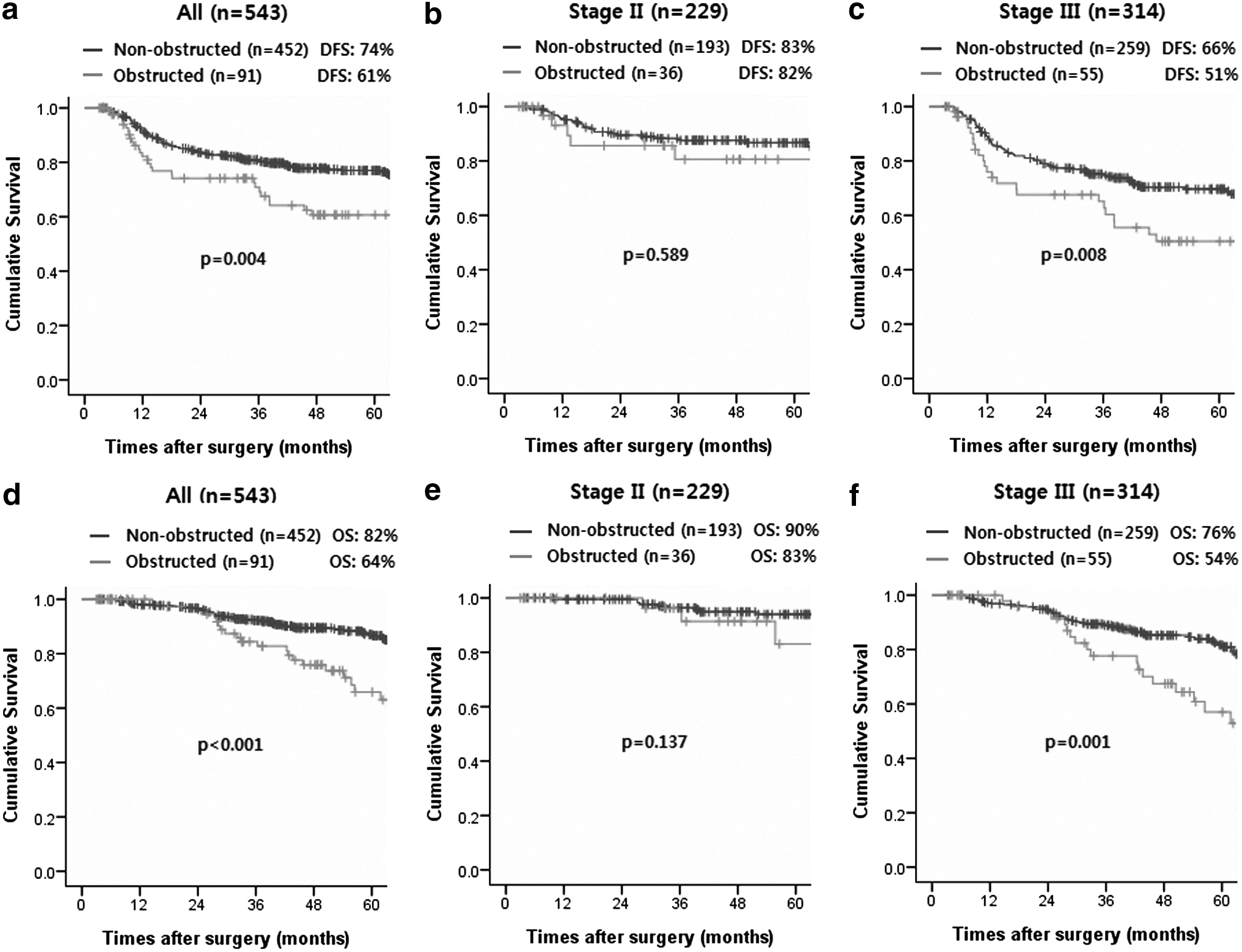
Kaplan–Meier analysis of 5-year
Overall recurrence occurred in 29 patients (31.9%) in the obstructed group and 102 (22.6%) in the nonobstructed group (P=.061). Local recurrence was diagnosed in 23 patients: 3 (3.3%) in the obstructed group and 20 (4.4%) in the nonobstructed group (P=.781). The median interval from surgery to local recurrence was 38.0 months (range, 18.0–82.0 months) for the obstructed group and 12.3 months (range, 5.1–68.9 months) for the nonobstructed group (P=.350). Systemic recurrence occurred in 26 patients (28.6%) in the obstructed group and 82 patients (18.1%) in the nonobstructed group (P=.030). Median interval from surgery to systemic recurrence was 11.7 months (range, 5.0–47.0 months) in the obstructed group and 15.4 months (range, 4.4–105.0 months) in the nonobstructed group (P=.294).
Survival analysis and recurrence patterns in stage II rectal cancer
The 5-year DFS was 82% for obstructed versus 83% for nonobstructed patients (P=.589) (Fig. 1b). The 5-year OS was 83% for obstructed versus 90% for nonobstructed patients (P=.137) (Fig. 1e).
Local recurrence was diagnosed in 6 patients, all in the nonobstructed group (3.1%) (P=.593). Systemic recurrence occurred in 5 patients (13.9%) in the obstructed group and 20 (10.4%) in the nonobstructed group (P=.561). The most common recurrence site was the liver, followed by the lungs, in both groups.
These results suggest that endoscopic obstruction is not associated with survival or recurrence patterns in patients with stage II rectal cancers.
Survival analysis and recurrence patterns in stage III rectal cancer
Postoperative chemotherapy was performed in 49 patients (89.1%) in the obstructed group and 243 (93.8%) in the nonobstructed group (P=.242). Postoperative radiotherapy was done in 10 patients (18.2%) in the obstructed group and 41 (15.8%) in the nonobstructed group (P=.688). Endoscopic obstruction was significantly associated with poorer DFS (P=.008) (Fig. 1c) and poorer OS (P=.001) (Fig. 1f). The 5-year DFS was 51% for obstructed versus 66% for nonobstructed patients. The 5-year OS was 54% for obstructed versus 76% for nonobstructed patients. The Cox proportional hazard model was applied to estimate the effect of endoscopic obstruction on survival. After controlling for various clinicopathologic factors, the adjusted hazard ratio of preoperative obstruction in patients with stage III rectal cancers was 1.48 (95% confidence interval, 0.71–3.07; P=.294) for DFS (Table 2) and 2.35 (95% confidence interval, 1.09–5.09; P=.030) for OS (Table 3). These results suggest that endoscopic obstruction in patients with stage III rectal cancer is an independent risk factor for OS, but not for DFS.
T and N indicate pathological factors according to the 7th edition of the American Joint Committee on Cancer tumor-node-metastasis grading system.
CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio.
T and N indicate pathological factors according to the 7th edition of the American Joint Committee on Cancer tumor-node-metastasis grading system.
CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio.
Local recurrence was diagnosed in 17 patients: 3 (5.5%) in the obstructed group and 14 (5.4%) in the nonobstructed group (P=1.0). Systematic recurrence occurred in 21 patients (38.2%) in the obstructed group and 62 (23.9%) in the nonobstructed group (P=.042). In the nonobstructed group, the lung (22 patients, 35.5%) was the most common recurrence site, followed by the liver (15 patients, 24.2%) and multiple sites (12 patients, 19.4%). In the obstructed group, multiple-site recurrence (9 patients, 42.9%) was the most common, followed by the liver (4 patients, 19.0%) and the lung (4 patients, 19.0%). Preoperative obstruction was significantly associated with multiple-site recurrence (P=.044) but not with other forms of recurrence. Among patients with systematic recurrence, salvage surgery was performed in 2 patients (10.0%) in the obstructed group and 24 patients (40.0%) in the nonobstructed group (P=.014) (Table 4).
Data are number of patients (% of group).
Among 21 patients with systematic recurrence, 1 patient was transferred to another hospital.
Among 62 patients with systematic recurrence, 2 patients were lost to follow-up.
Discussion
The definition of obstruction varies from partial obstruction to complete obstruction, which requires emergency decompression. No universally accepted consensus definition exists, but most studies have not reported the outcomes of endoscopically obstructive colorectal cancers. The increase in prevalence of colonoscopic screening for colorectal cancers has resulted in an increased number of reports of endoscopic obstruction with or without obstructive symptoms. Furthermore, owing to the paucity of rectal obstruction cases, most studies have reported combined results of the colon and rectum.2,4–6 In the present study, we investigated obstructive rectal cancers in a large patient cohort using a clear definition of endoscopic obstruction.
In our study, more patients in the obstructive group than in the nonobstructive group were diagnosed with a T4 tumor, which is a known risk factor for advanced stage and worse prognosis. 9 Furthermore, preoperative CEA level was significantly greater in the obstructive group than that in the nonobstructive group; a high preoperative CEA level is associated with occult metastasis and poorer survival.10,11 Although the obstructive and nonobstructive groups had similar tumor stages, nodal status, lymphatic or vascular invasion incidence, and tumor differentiation status, our findings suggest that obstruction may reflect more advanced disease. However, because of the limited number of patients enrolled in our study, we divided the patients into two intermediate stages (stages II and III). Subdivision of the stages would have resulted in a loss of statistical power.
In the univariate analysis, endoscopic obstruction predicted a poor DFS and OS in patients with stage III cancer, but not those with stage II cancer, consistent with a previous report. 4 We performed a multivariate analysis in patients with stage III rectal cancer to adjust for potential confounding factors. Nodal status and preoperative CEA level were independent prognostic factors for DFS, whereas preoperative obstruction and nodal status were independent prognostic factors for OS. It is universally accepted that nodal status predicts poor survival in colorectal cancers; therefore, it is clinically used in TNM substaging. 12 Although the usefulness of preoperative CEA level as a prognostic marker has been debated,10,13 our results indicate that a high preoperative CEA level was associated with poor DFS. It is unclear based on previous studies whether preoperative obstruction can affect prognosis.1–4 This may be due to various definitions of obstruction, mixed stages, or differences in resectability rates. Thus, we focused only on patients who underwent curative resection for endoscopically obstructive rectal cancers. Each stage was separately analyzed; endoscopic obstruction predicted poor OS in patients with stage III rectal cancer, but not in those with stage II rectal cancer.
Endoscopic obstruction was not associated with local recurrence, in accordance with Carraro et al. 5 They suggested that obstruction does not influence local recurrence and that adequate local control is related to surgeon-related factors. 5 If appropriate decompression can be performed before curative resection, inadequate resection or tumor disruption during surgery related to local recurrence can be avoided. However, our local recurrence rate (3.3% in the obstructive group) was far below the reported values of 12%–14%.5,6 Because our definition of obstruction included less severe forms than other studies,5,6 our results should be interpreted with caution.
Systemic recurrence was more common in obstructive stage III rectal cancers, consistent with the findings of Katoh et al. 4 Increased metastatic potential of obstructive lesions suggests the presence of a higher proportion of occult metastasis.4,5 Endoscopic obstruction was significantly associated with multiple-site recurrence but not with other forms of recurrence. When systemic recurrence occurred in stage III rectal cancers, salvage surgery was performed less frequently in the obstructed group than in the nonobstructed group (10% versus 40%; P=.014). The liver is the most commonly reported site of distant failure in colorectal cancer, whereas we found that multiple-site recurrence was more common than liver recurrence for obstructive rectal cancers. In patients with rectal cancer, an obstructing lesion in a narrow pelvis may contribute to changes in lymphatic or venous flow, which can affect recurrence patterns. If recurrent cancer can be detected when limited in site or number, representing potentially resectable or curable cancer, the success rate of salvage therapy is likely to increase.
This study had some limitations. First, it was retrospective in nature. Second, the two groups were not completely comparable, indicating that further studies are required to validate our conclusions. A larger study is required to enable subdivision of stages to confirm that obstructive rectal cancer represents more advanced disease. Third, we considered combined cases of local and systemic recurrence as systemic recurrence cases. However, it is disputable whether local recurrence occurs simultaneously or is disseminated from the systemic recurrence.
Conclusions
Endoscopic obstruction in patients with stage III rectal cancers predicted worse OS and was associated with multiple-site systemic recurrence. Endoscopic obstruction may be a novel marker indicating the need for more intensive adjuvant therapy and follow-up in patients with stage III rectal cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.