
Abstract
Abstract
Introduction:
Recently a retrospective study has been published describing a significant correlation of immediate postoperative leukocytosis (IPLC) and a favorable pathological Gleason score (pGS) in patients undergoing robotic-assisted radical prostatectomy (RARP). The aim of the present study was to prospectively validate these results on an external dataset.
Materials and Methods:
In total, 346 patients undergoing RARP as first-line therapy for localized prostate cancer were included. Clinical and histopathological parameters, criteria of IPLC, and pGS were recorded prospectively. Potential association between IPLC and pGS was evaluated by univariate and multivariate analyses.
Results:
IPLC was found in 77.2% (n = 267) of all patients with a median leukocyte blood count (LBC) of 12.5 × 109/L (interquartile range, 10.2–15 × 109/L). Of these, in 255 patients IPLC was found within the range of 10–20 × 109/L, whereas an IPLC of >20 × 109/L was found in only 12 patients. Of the patients, 49.1%, 40.5%, and 10.4% presented with a pGS6, pGS7, and pGS8–10 tumor, respectively. There was neither a univariate nor a multivariate correlation between IPLC and pGS. Furthermore, no significant correlation could be detected between IPLC and other clinical, intraoperative, or histopathological criteria. In 175 (66%) patients with IPLC normal LBC levels were measured on postoperative Day 4.
Conclusions:
IPLC was not associated with more favorable tumor biology (lower pGS, better tumor stage) and not influenced by patient conditions (age, body mass index, American Society of Anesthesiologists score, smoking) or intraoperative parameters (blood loss, operating time, surgeon). In addition, there was no significant correlation with serious complications (Clavien–Dindo Grade 3a/b) within a period of 90 days.
Introduction
T
Basically, concerning postoperative leukocytosis, we need to distinguish between a complication caused by systemic inflammatory response and a physiologically induced host response by cytokines. 7 In a study by Anderson et al., 8 of 50 laparoscopic urological procedures (42% of these were radical prostatectomies) performed without any complications, immediate postoperative leukocytosis (IPLC) occurred in 36%. Recently Patel et al. 9 reported the results of a retrospective study including 768 patients undergoing RARP and found that IPLC varied significantly depending on race, with a lower frequency in African American patients. Additionally, IPLC was less frequent in patients with a pathological Gleason score (pGS) of 8–10. 9 Unfortunately, the authors did not provide any data regarding frequency of IPLC after RARP. Moreover, correlation between IPLC and either intraoperative parameters (e.g., blood loss and time of surgery) or complications in short-term follow-up has not been analyzed. 10
To address these questions, we aimed at proving three hypotheses using a prospective study design: (1) IPLC may suggest favorable tumor biology, (2) IPLC is associated with certain intraoperative parameters like “higher blood loss” and “longer operating time,” and (3) IPLC is not associated with a higher rate of serious complications (according to Clavien–Dindo classification).
Materials and Methods
In total, 346 white patients were enrolled in the present study, based on a prospective dataset including all patients undergoing primary RARP for localized PCA at the Department of Urology, St. Elisabeth-Klinikum Straubing, Straubing, Germany between 2008 and 2013. RARP or open radical prostatectomy was offered to each patient. Except for absolute contraindications of RARP (not allowing for extreme Trendelenburg position), no other exclusion criteria were defined.5,11 Clinical and pathological data were collected after informal consent was obtained according to the local ethical committee.
RARP was performed using a transperitoneal approach including regional lymph node dissection by two surgeons with different expertise in robotic surgery. Conversion to open surgery was not performed in the study cohort. Perioperative intravenous antibiotic prophylaxis was standardized taking into account individually known allergies (usually cefuroxime in three dosages of 1.5 g, with first application directly before RARP). 11
Leukocyte blood count (LBC), platelet count, and C-reactive protein were recorded in all patients at three different time points: (1) 1 day before RARP (d–1), (2) on the day of surgery immediately after RARP (d0) and (3) on the third or fourth postoperative day (d3–4). The following clinical and histopathological parameters were recorded: age, body mass index, American Society of Anesthesiologists physical status, Eastern Cooperative Oncology Group performance status, active smoker status, prostate-specific antigen level, clinical tumor stage, biopsy Gleason score, surgeon, operating time (incision–suture time), intraoperative blood loss, intraoperative complications (occurrence of unforeseen organ injury), nerve-sparing surgery, number of lymph nodes removed, pGS, and surgical margins. Histopathological assessment of RARP specimens was performed at one pathological institute and reviewed by a senior pathologist with uropathological expertise (Dr. Werner Mohren, Pathology Institute of St. Elisabeth Hospital Straubing). Furthermore, the 90-day complication rate was evaluated according Clavien–Dindo classification during standardized follow-up. 10
Serum parameters were recorded as metric absolute values (interval scaled) and categorized by means of specific normal values (NVs): NV, >NV up to 2× NV-upper limit, and >2× NV-upper limit. For LBC, platelet count, and C-reactive protein, the upper limit of NV was set at 10 × 109/L, 350 × 109/L, and 10 mg/L, respectively. 12 Medians and interquartile ranges were generated for continuously coded variables, and frequency and proportion were used for categorical variables. Mann–Whitney and chi-squared tests were used to assess differences in medians and proportions, respectively. Between the categorically distributed and metrically measured serum parameters at time point d0 and various previously categorized respective metric study criteria, bivariate correlations were calculated according to Spearman rank correlation coefficient (Spearman ρ). Spearman ρ presents a dimensionless number with a range between –1 and 1 (ρ < 0 and ρ > 0 show a negative and a positive correlation, respectively).
Finally, a multivariate logistic regression model (MLRM) was generated to examine the independent influence of various criteria on IPLC. LBC as a dependent variable and end point (EP) for the MLRM was categorized based on two dichotomizations: (1) EP1, leukocytosis at time d0 versus any other option; and (2) EP2, leukocytosis at d0 and d3–4 versus any other option. The quality of the adjustment of MLRM was assessed by the likelihood function; the reproduced coefficient of determination R2 after Nagelkerke expresses the proportion of variance that is explained by logistic regression. In other words, the R2 coefficient acts as a surrogate for the performance of the MLRM. By development of the MLRM, a R2 of 0.35 was at least provided (claim, R2 ≥0.35). The influence of various independent variables on the dependent variable was represented by odds ratio and 95% confidence intervals. Internal validity of individual variables in the MLRM was examined by the bootstrap technique (with 1000 resamples). The difference between the coefficients in the original sample and bootstrap samples as reflected by the slope index is the measure for the amount of optimism. Normally, slope values range from 0 and 1. A slope value of 1 indicates no optimism. The slope index was used as a shrinkage method by multiplying coefficients with this slope index to correct for optimism.
Statistical analysis was performed using SPSS version 21 software (2011 release; IBM Corp., Armonk, NY). Values of P < .05 were considered statistically significant.
Results
LBC, platelet count, and C-reactive protein values of all 346 patients are displayed for the different time points (Figs. 1–3). IPLC was evident in 77.2% (n = 267) of the patients after RARP at time point d0, whereas 22.8% (n = 79), 73.7% (n = 255), and 3.5% (n = 12) showed no leukocytosis, leukocytosis within ≤2× NV-upper limit, and >2× NV-upper limit, respectively. Clinical and histopathological parameters are shown in Table 1. pGS6, pGS7, and pGS8–10 tumors were found in 49.1%, 40.5%, and 10.4% of the patients, respectively. Positive surgical margins were detected in 28.9% (n = 100) of the patients.
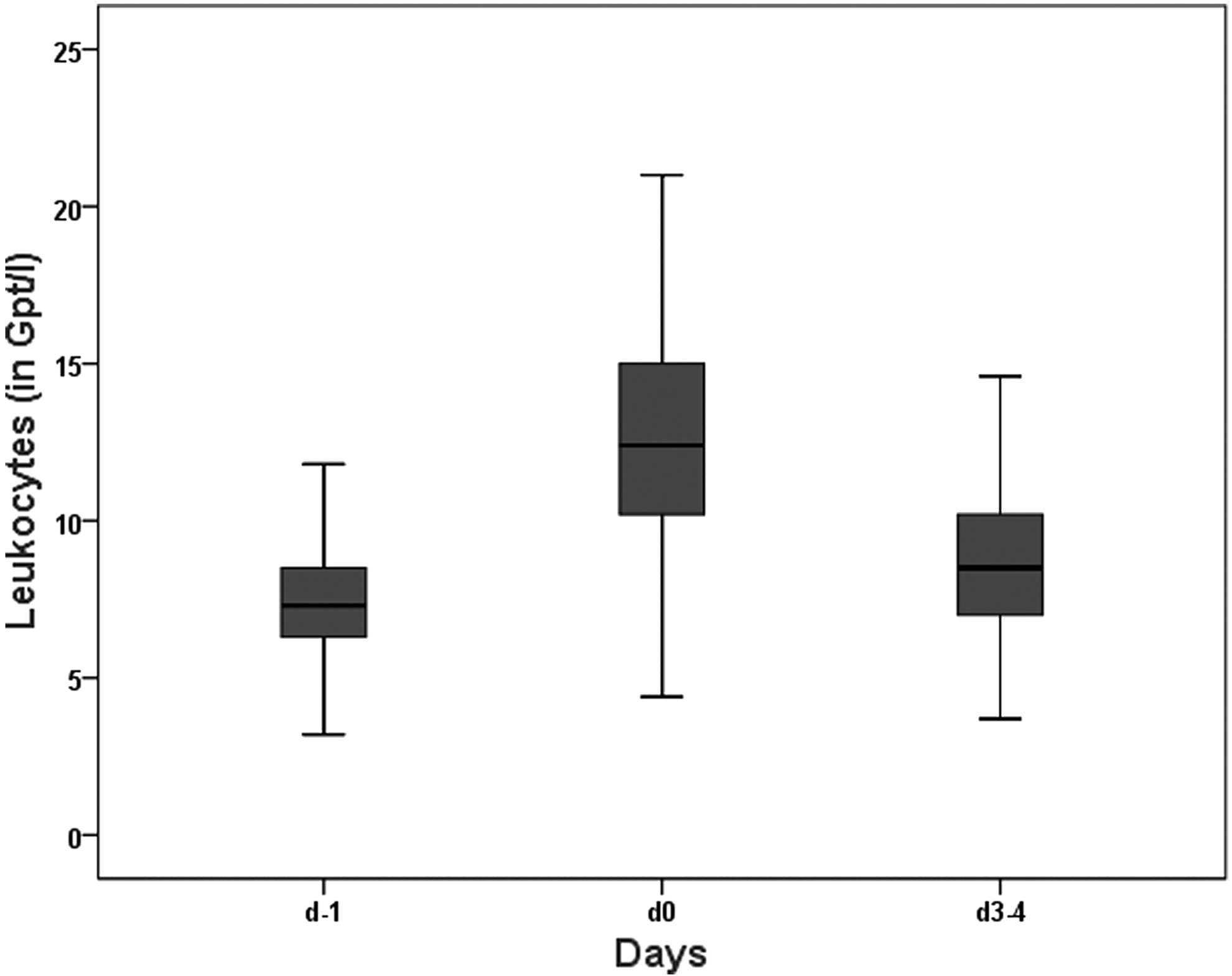
Boxplot of white blood cell count in venous blood at three time points: (1) 1 day before robotic-assisted radical prostatectomy (d–1), (2) on the day of robotic-assisted radical prostatectomy immediately after surgery (d0), and (3) on Day 3 or 4 after robotic-assisted radical prostatectomy (d3–4). Median (interquartile range) values are as follows: d–1, 7.3 (6.3–8.6) × 109/L; d0, 12.5 (10.2–15) × 109/L; and d3–4, 8.5 (7–10.3) × 109/L. Gpt, × 109.
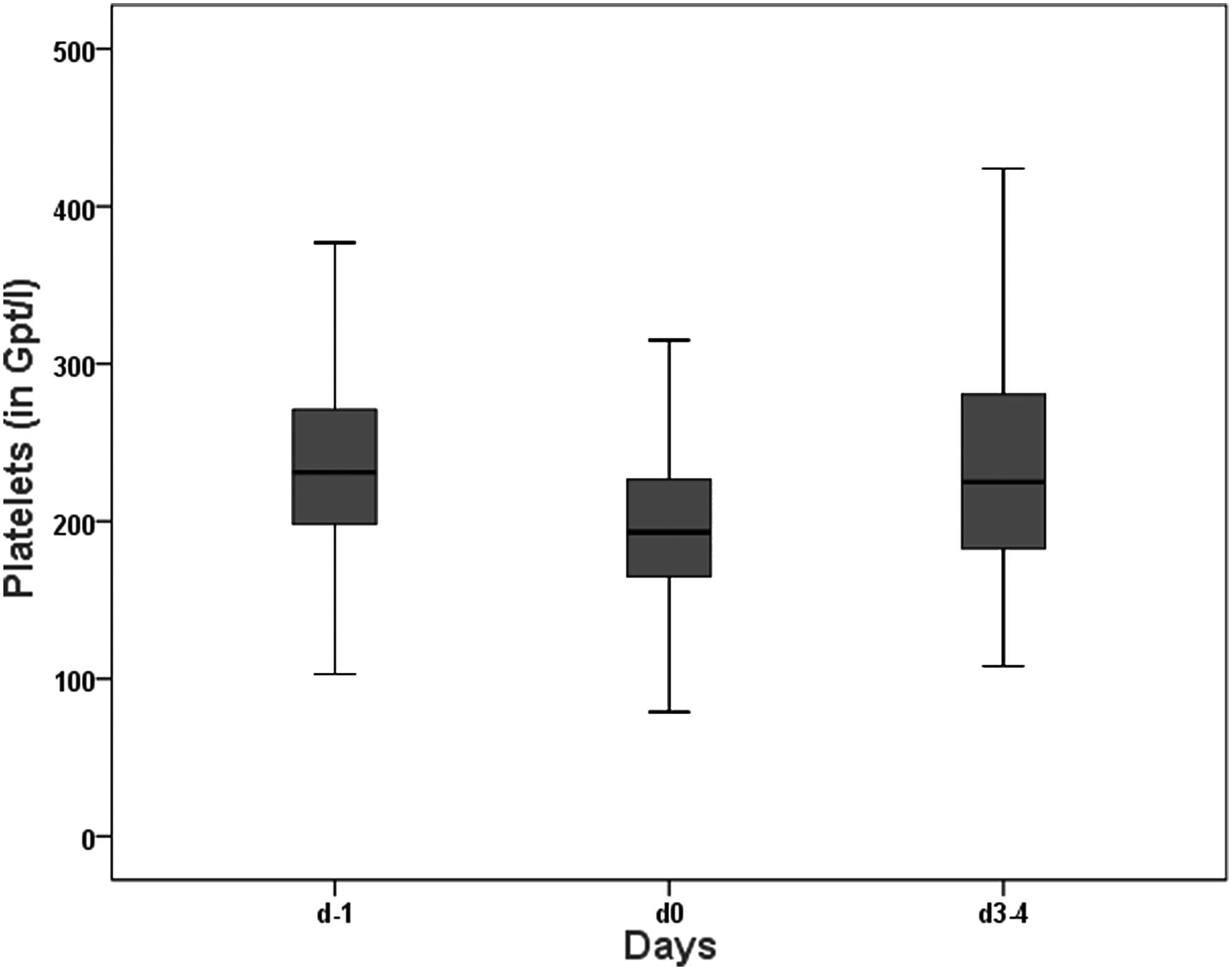
Boxplot of platelet count in venous blood at three time points: (1) 1 day before robotic-assisted radical prostatectomy (d–1), (2) on the day of robotic-assisted radical prostatectomy immediately after surgery (d0), and (3) on Day 3 or 4 after robotic-assisted radical prostatectomy (d3–4). Median (interquartile range) values are as follows: d–1, 231 (198–271) × 109/L; d0, 195 (165–227) × 109/L; and d3–4, 230 (185–294) × 109/L. Gpt, × 109.

Boxplot of C-reactive protein (CRP) level in venous blood at three time points: (1) 1 day before robotic-assisted radical prostatectomy (d–1), (2) on the day of robotic-assisted radical prostatectomy immediately after surgery (d0), and (3) on Day 3 or 4 after robotic-assisted radical prostatectomy (d3–4). Median (interquartile range) values are as follows: d–1, 0.1 (0.1–0.3) mg/L; d0, 2.2 (0.6–6.0) mg/L; and d3–4, 5 (2.3–8) mg/L.
Parameters were correlated with the metric white blood cell count at time point d0 (on the day of robotic-assisted radical prostatectomy [RARP] immediately after surgery) and the categorized white blood cell count at point d0 (no immediate postoperative leukocytosis versus immediate postoperative leukocytosis ≤2× normal values versus immediate postoperative leukocytosis >2× normal values).
No Grade 4 and 5 complications according to Clavien–Dindo classification were recorded.
ASA, American Society of Anesthesiologists; BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range; PSA, prostate-specific antigen.
There were no significant correlations between LBC, platelet count, or C-reactive protein values and one of the clinical or histopathological parameters at any time point. In particular, no significant correlation was found between LBC (d0) and biopsy Gleason score (for metric, ρ = −0.044, P = .419; for categorical, ρ = −0.088, P = .103) or pGS (for metric, ρ = −0.016, P = .773; for categorical, ρ = −0.039, P = .467) (Table 1). Correlations of further study parameters and LBC (d0) are also displayed in Table 1. Metric LBC did not differ by means of pGS at any time point (p > 0.05) (Fig. 4).
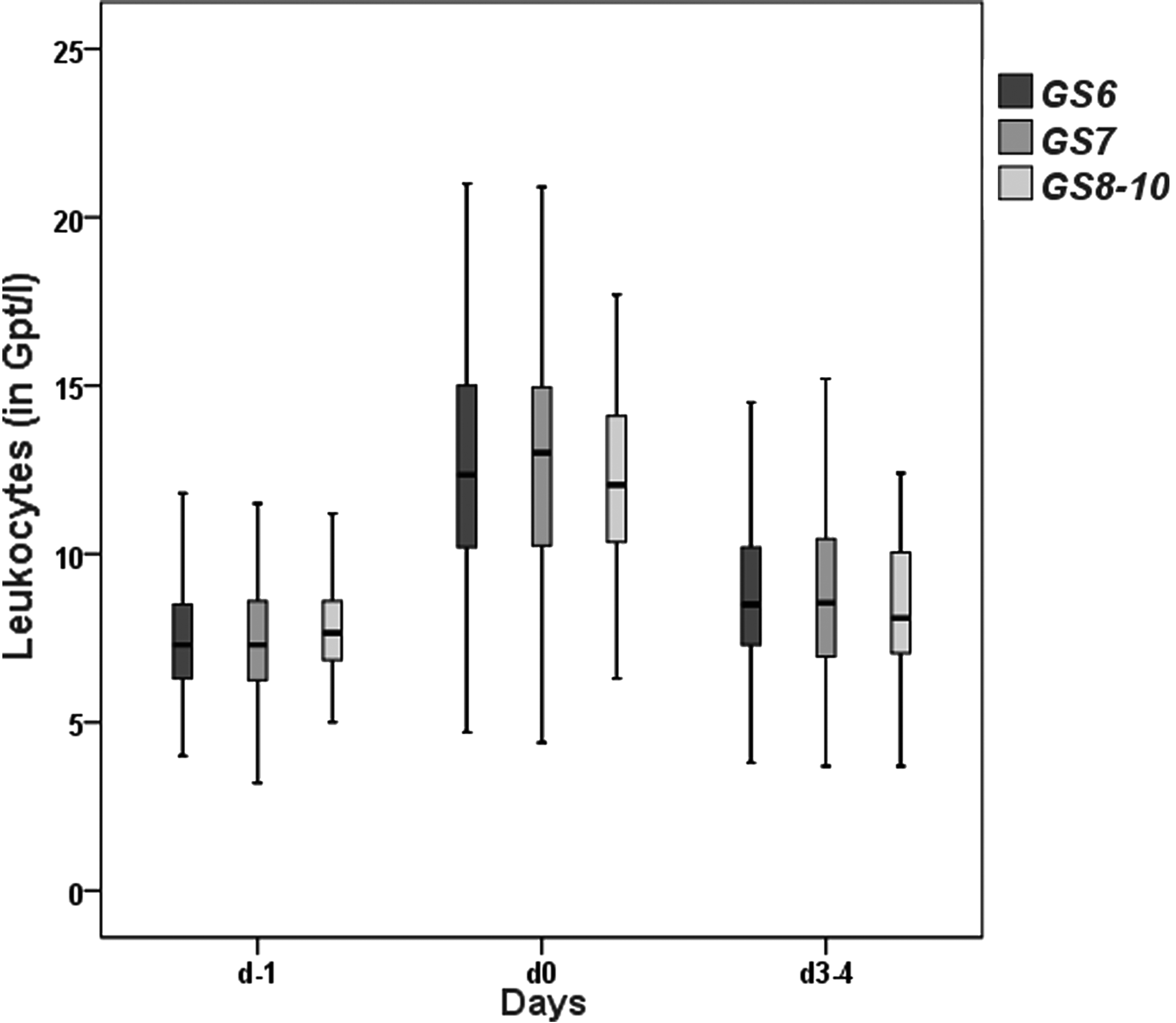
Boxplot of white blood cell count in venous blood at three time points: (1) 1 day before robotic-assisted radical prostatectomy (d–1), (2) on the day of robotic-assisted radical prostatectomy immediately after surgery (d0), and (3) on Day 3 or 4 after robotic-assisted radical prostatectomy (d3–4) according to pathological Gleason score (GS) of GS6, GS7, and GS8–10. Gpt, × 109.
The influence of several clinical and histopathological parameters on the different predefined EPs related to perioperative leukocytosis was examined in two independent MLRMs (Table 2). pGS did not influence either EP1 or EP2. Also, all further histopathological and intraoperative parameters did not significantly impact these two EPs. In addition, for both EP1 and EP2 no independent correlation between perioperative leukocytosis and postoperative complication rate (defined by dichotomized Clavien–Dindo classification, Grade 0–2 versus 3a/b) was observed (Table 2). Odds ratios calculated in the two independent MLRMs are bootstrap corrected and thereby confirmed to be internally valid with slope indices exceeding 0.93.
End points were as follows: (1) EP1, leukocytosis at time d0 (on the day of robotic-assisted radical prostatectomy [RARP] immediately after surgery) versus any other option (AOO); and (2) EP2, leukocytosis at d0 and d3–4 (on Day 3 or 4 after RARP) versus AOO. For EP1, 267 events were recorded, hence, all 18 parameters were included in this model (R2 = 0.403). For EP2, only 92 events were recorded; therefore the number of variables was reduced to 9 (R2 = 0.374).
Due to high collinearity between the biopsy Gleason score and the pathological Gleason-Score (pGS), only pGS was included in this model.
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; OR, odds ratio; PSA, prostate-specific antigen.
Discussion
The purpose of the present study was to validate recently published data suggesting a potential correlation between perioperative leukocytosis and pGS in patients undergoing RARP. Recently, Patel et al. 9 showed that the presence of IPLC correlated with pGS and race based on a retrospective dataset including 768 RARP patients. This investigators demonstrated that patients with IPLC had a lower pGS and more often belonged to the white and Hispanic race. Because patients belonging to different races did not differ with regard to pGS (P = .652), the correlation of IPLC with these two parameters was independent. 9 With the present study we aimed at proving three hypotheses based on a prospective dataset of a homogeneous group of 346 white patients undergoing RARP for biopsy-proven localized PCA. In summary, our results conclude that IPLC, which was present in 77% of the study patients, (1) was not associated with a more favorable tumor biology (pGS), (2) was not influenced by intraoperative parameters (e.g., loss of blood, surgical time, surgeon), and (3) was not an early sign indicating serious adverse events (Clavien–Dindo Grade 3a/b) (Tables 1 and 2). Therefore the clinical benefit of a routine close monitoring of LBC after RARP needs to be questioned.
Nevertheless, there is significant research activity around the possible prognostic relevance of various systemic inflammatory parameters in different tumor entities.13–17 Increased attention is given to the fraction of neutrophils, which normally represent between 50% and 70% of leukocytes.15–17 Neutrophils play a key role in the immune response (“host defense”) against invading microorganisms. Beyond this aspect there is robust evidence that tumor-associated neutrophils interfere with tumor biology in various cancer types (such as, e.g., PCA). Tumor-associated neutrophils are supposed to invade tumor tissue under the influence of chemokines, cytokines, and cell adhesion molecules and thus change the specific microenvironment. 15 However, because an exact characterization of tumor-associated neutrophils and their function is still lacking to date, it remains unclear whether tumor-associated neutrophils facilitate an antitumor effect (N1 phenotype) or whether they enhance tumor growth by suppressing the antitumor immune response (N2 phenotype) mediated by the tumor's own growth signals (e.g., transforming growth factor-β). Based on current evidence, in PCA patients a higher fraction of neutrophils (measured as neutrophil/lymphocyte ratio) seems to be associated with more aggressive tumor biology and worse tumor-specific survival independent of tumor stage.
Such tumor-induced immune mechanisms need to be distinguished from the common perioperative leukocytosis, which can be interpreted as a physiological host response mediated by cytokines.7,8,18,19 In the present cohort of patients undergoing RARP, IPLC was found in 9.5% (n = 33), 77.2% (n = 267), and 28.6% of patients (n = 99) at d–1, d0, and d3–4, respectively, without any association with a more aggressive tumor biology (Figs. 1 and 4).
Our study is not devoid of limitations, which should be taken into account for interpretation of the results. We did not address tumor-specific recurrence and mortality rates as EPs potentially better reflecting the prognostic impact of IPLC. Furthermore, no differential leukocyte counts (hemograms) were assessed, and therefore the significance of the neutrophil fraction could not be investigated. In addition to that, 29% of the patients presented with increased leukocyte counts on d3–4, but further follow-up data regarding normalization of LBC were not available, and hence we cannot estimate the time interval until normalization of this parameter in this subgroup. Moreover, because the study was European based and the study cohort comprised white patients undergoing RARP only, we cannot estimate effects of IPLC on tumor biologic and functional outcome in comparison with different ethnicities or with patients undergoing open radical prostatectomy.9,20 The strengths of the present study are its homogeneous study population in a prospectively assessed dataset. In addition to that, the impact of two surgeons with different levels of expertise in robotic surgery was evaluated.11,21
Conclusions
In patients undergoing primary RARP for PCA, IPLC was not associated with a more favorable tumor biology (lower pGS, better tumor stage), was not influenced by patient conditions (age, body mass index, American Society of Anesthesiologists score, and smoking) or intraoperative parameters (blood loss, operating time, surgeon), and did not predict the occurrence of serious complications (Clavien–Dindo Grade 3a/b) within a period of 90 days. Hence, routine assessment of LBC in the postoperative setting after RARP is not required in clinically uneventful patients. Further studies addressing this topic should integrate assessment of differential blood counts and cytokines to better understand the underlying physiological and tumor biology–dependent processes of perioperative leukocytosis after RARP.
Footnotes
Acknowledgments
We thank Mrs. Stefanie Wolf (study coordinator at the Oncology Center, St. Elisabeth Hospital, Straubing, Germany) for maintaining the prospective RARP database and Dr. Werner Mohren (Pathology Institute of St. Elisabeth Hospital) for pathological evaluation.
Disclosure Statement
No competing financial interests exist.