
Abstract
Abstract
Background:
High-quality images can be readily captured during laparoscopic colon surgery, but there are no guidelines for documentation of these video data or how to best measure surgical quality from an operative video. This study evaluates the feasibility and compliance in documenting key steps during laparoscopic right hemicolectomy and sigmoid colectomy.
Materials and Methods:
A retrospective review of previously recorded videos of patients undergoing laparoscopic right hemicolectomy or sigmoid colectomy from September to December 2011 in a single institution was performed. Patients' demographics, intraoperative features, postoperative complications, and variables for video recording and editing were collected. Compliance of key surgical steps was assessed using a checklist by two independent surgeons.
Results:
Sixteen laparoscopic operations (seven right hemicolectomies and nine sigmoid colectomies) were recorded. Twelve (75%) were laparoscopic-assisted, and four (25%) were hand-assisted laparoscopic operations. Compliance with key surgical steps in laparoscopic right hemicolectomy and sigmoid colectomy was demonstrated in the majority of patients, with steps ranging in compliance from 42.9% to 100% and from 77.8% to 100%, respectively. The edited video had a median duration of 3 minutes 47 seconds (range, 1 minute 44 seconds–5 minutes 38 seconds) with a production time of nearly 1 hour and a resolution of 1440 × 1080 pixels.
Conclusions:
Key surgical steps during laparoscopic right hemicolectomy and sigmoid colectomy can be documented and edited into a short representative video. Standardization of this process should allow video documentation to improve quality in laparoscopic colon surgery.
Introduction
G
Strasberg et al. 1 initially introduced the concept of the critical view of safety as an important technique in preventing bile duct injury when performing laparoscopic cholecystectomy. To ensure quality, documentation of the critical view of safety, through either photo or video capture, has become required practice when performing laparoscopic cholecystectomy in The Netherlands since that time.2–4 A similar concept in quality control for laparoscopic colon surgery could be the formulation of a surgical “checklist” that defines critical operative steps and subsequent video documentation of these steps to ensure surgeon compliance. However, there are no established guidelines for this.
Usage of multimedia technology has become widespread in the medical community. Digital video documentation is increasingly being used to record operative procedures and has been claimed to improve intraoperative visualization as well as ensure accurate imaging and documentation.5,6 However, a typical operation includes many minutes of irrelevant (e.g., cleaning the camera lens) or tedious (e.g., lengthy dissection through thick mesentery) footage that are also recorded, and filtering out only the most critical steps can be a tiresome task.
The aim of this pilot study was to evaluate the feasibility and compliance of video documentation of the key steps in laparoscopic right hemicolectomy and sigmoid colectomy using a checklist, as well as the ability to edit the recorded footage into a brief, representative video depiction of the operation.
We submitted a video related to this manuscript to Videoscopy, which we have referred to within the body of this text. This video was accepted and can be found online at http://online.liebertpub.com/doi/full/10.1089/vor.2014.0260
Materials and Methods
This study was approved by the Institutional Review Board of Weill Cornell Medical College. All archived video recordings of patients 18 years of age or older who had undergone either laparoscopic right hemicolectomy or sigmoid colectomy performed by three surgeons on the Colorectal Service at Weill Cornell Medical College/NewYork-Presbyterian Hospital from September to December 2011 were included. Twenty-four colectomies (right hemicolectomy, sigmoid colectomy) were performed during the study period. Sixteen (67%) colectomies met inclusion criteria and were included; the remaining 8 cases were excluded because of incomplete or lack of video recording. Clinical and technical variables including patient demographics, operative features, postoperative complications, and the resolution, storage, and editing data of the operative videos were collected.
Feasibility was defined as the ability to record and accurately demonstrate key surgical steps with high-quality video. Compliance was defined as demonstration of the presence of the key surgical steps and their corresponding landmarks upon review of previously recorded colectomies that were not performed according to an operative checklist defining those key steps.
Predetermined key surgical steps and corresponding anatomical landmarks
The key surgical steps and landmarks for both laparoscopic procedures were defined by expert surgeons in our department and are listed in Table 1. These are visually demonstrated with a representative video (found online at http://online.liebertpub.com/doi/full/10.1089/vor.2014.0260) and corresponding images (Figs. 1 and 2) from the examined cohort.
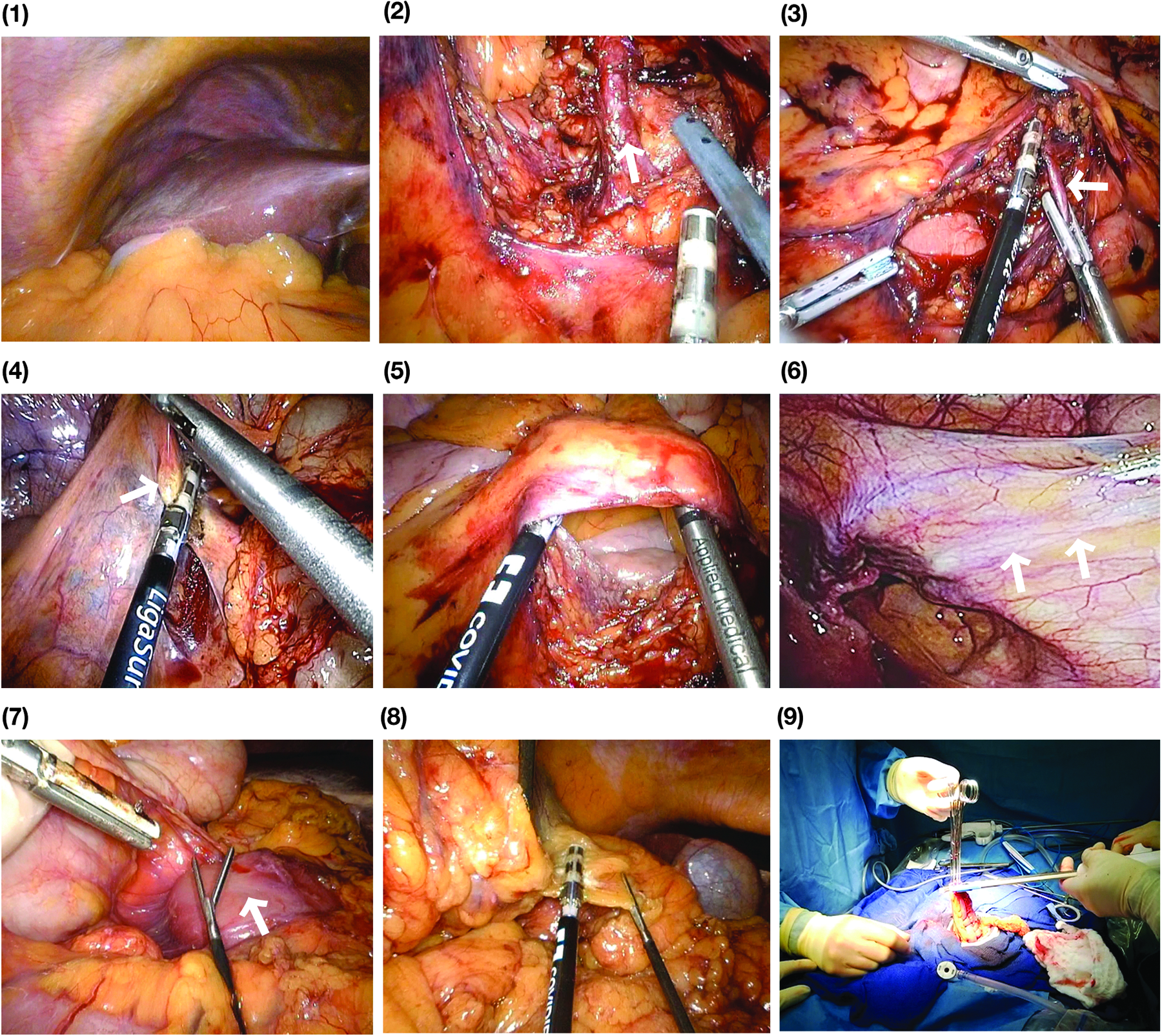
Documentation of key surgical steps in right hemicolectomy. Shown are visual representations of surgical steps for right hemicolectomy:
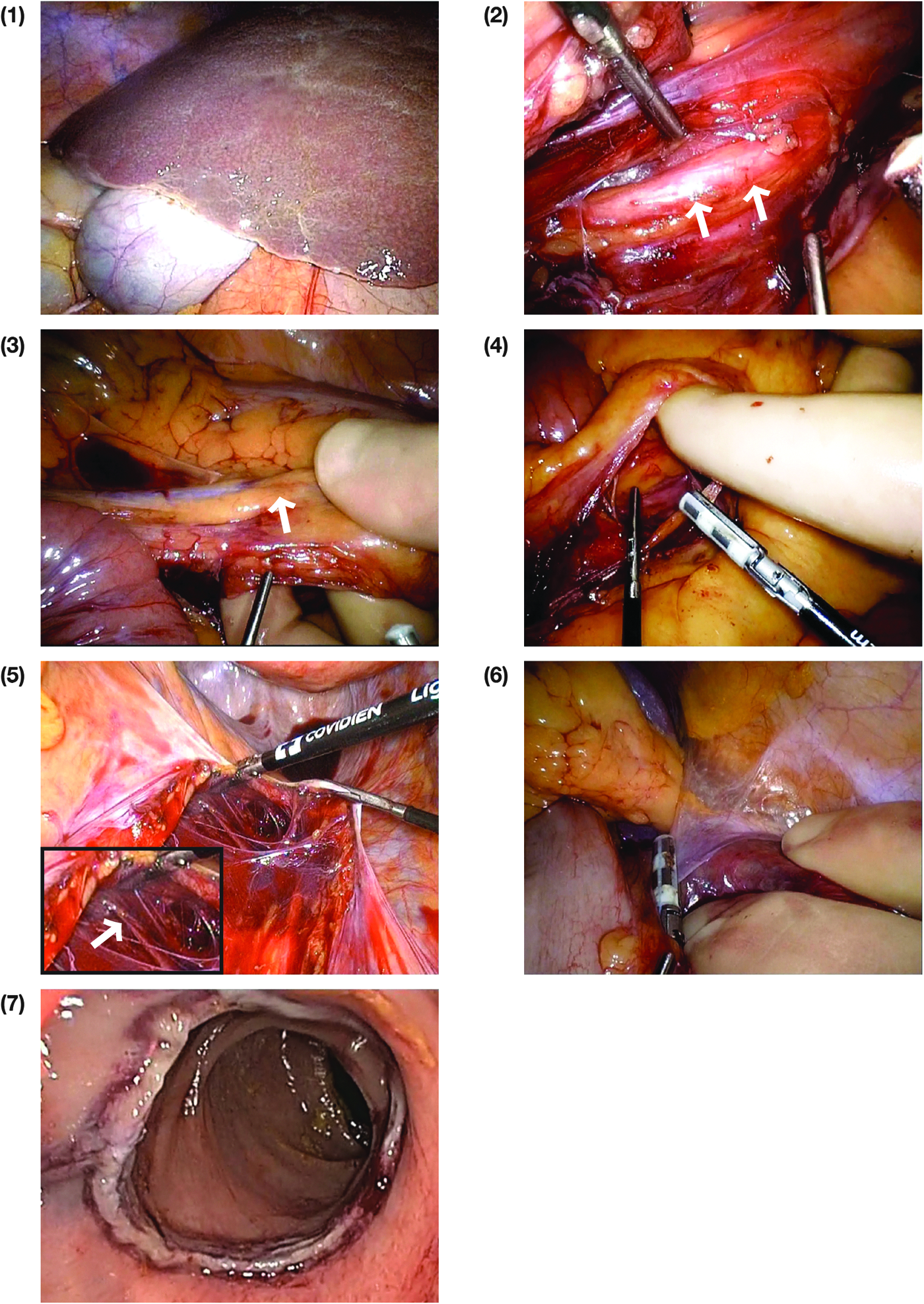
Documentation of key surgical steps in sigmoidectomy. Shown are visual representations of surgical steps for sigmoidectomy:
IMA, inferior mesenteric artery; SMV, superior mesenteric vein.
Video capturing and recording
A high-definition (HD) laparoscopic camera (light source, EVIS EXERA II Xenon CLV-180; rigid laparoscopes, 5-mm or 10-mm scopes with 0° or 30° directional view [Olympus America, Melville, NY]) was used to record the intracorporeal component of the operation, and an endoscopic camera (light source, VISERA ELITE Xenon CLV-S190; flexible video sigmoidoscope [EVIS PCF-240; Olympus America]) was used for intraoperative colonoscopic recording. Institution standard, operating room rack-mounted video equipment (nStream + HD; Olympus America) was used to record the HD video data. Prior to the operation, the video recording system was turned on, and the patient and surgeon data were entered. Actual recording was initiated either by surgeon control using buttons in the laparoscope/colonoscope handle or by an assistant using the control panel on the rack-mounted video system. Recording was started prior to the initiation of the case and stopped at its conclusion. Finally, photographic documentation of the surgical specimen was obtained using a hand-held digital camera (Lumix® DMC-LX3; Panasonic North American, Secaucus, NJ). Upon completion of the operation, all photo and video data were exported, labeled with a unique number, and archived to a password-protected computer with a 2.8-GHz Duo processor, 4 GB RAM, 500 GB SATA II hard drive, and a Windows® 7 Professional 64-bit operating system (Microsoft, Redmond, WA).
Video editing and evaluation
Commercial video-editing software (Adobe Premiere Pro CS 5.5; Adobe Systems Inc., San Jose, CA) was used to edit the full-length archived recordings into several short segments representing the key surgical steps by a surgical research fellow. The videos were then independently reviewed for compliance using a checklist by two attending colorectal surgeons who were blinded to the identity of the patient and the operating surgeon. Compliance to the key surgical steps was assessed by evaluating whether (1) the key steps presented in the short edited video clips were indeed present in the unedited full-length raw video and (2) if the key steps were not presented in the short edited video clips, that they were truly absent from the unedited full-length raw video.
From these short video segments, we identified landmark anatomy and captured representative still images (Figs. 1 and 2). For the purpose of this manuscript, video was converted to AVI file format, and corresponding still images were converted to 300 DPI in TIFF format.
Statistical analysis
Categorical data were presented as numbers and percentages. Continuous data were described by median and range. Statistical analysis was performed using JMP version 9.0 statistical software (Cornell University, Ithaca, NY).
Results
In total, 16 laparoscopic operations (seven right hemicolectomies and nine sigmoid colectomies) were captured on video from September through December 2011. Patient demographics and operative features are described in detail in Table 2.
BMI, body mass index; ASA, American Society of Anesthesiologists; LOA, lysis of adhesions; LOS, length of stay.
At the conclusion of an operation, video export to an external drive was variable, depending on operation length and file size, but did not exceed 10 minutes. After the key surgical steps were identified from the original recording over approximately 15 minutes, the median time to produce an edited video clip was 29 (range, 21–42) minutes. Thus, the overall editing and video production process was performed in close to an hour. The recorded and edited video clips had a resolution of 1440 × 1080 pixels. The edited video had a median storage volume of 659 (range, 320–1010) MB with a median duration of 3 minutes 47 seconds (range, 1 minute 44 seconds–5 minutes 38 seconds). Video capturing and editing results are described in Table 3.
Full compliance to the key surgical steps in both laparoscopic procedures was achieved in the majority of patients. Laparoscopic right hemicolectomy and sigmoid colectomy compliance ranged from 42.9% to 100% and from 77.8% to 100%, respectively. The online video (http://online.liebertpub.com/doi/full/10.1089/vor.2014.0260) demonstrates representative video clips of compliant surgical steps with corresponding still images seen in Figures 1 and 2. The surgical checklist used by reviewers summarizes these results in detail in Table 4.
Recommended.
Discussion
Several international large, multicenter trials have shown outcomes following a laparoscopic approach to be technically as well as oncologically equivalent to conventional open colectomy,7–10 and adoption of laparoscopic colectomy for the treatment of various colonic diseases has increased in the past decade. In addition to the reported advantages of laparoscopy, accompanying video recording systems enable surgeons to record their operations in great detail and high resolution. However, the ability to capture intraoperative details in an era of increasing medical transparency and documentation requirements is underutilized by surgeons. In this study, we found that recording the key steps during laparoscopic colon surgery can be readily achieved in HD and edited into a brief video that highlights these important steps.
By providing high-quality imaging as well as a magnified view of the anatomical details in the operative field, video capture using a standard laparoscopic camera should be regarded as a valuable piece of documentation that can reliably record what has been performed by the surgeon during an operation.11,12 It enables surgeons to better inform their patients, to accurately share experiences with their colleagues, and to train medical students, residents, other surgeons, and the surgical team more efficiently. 2 Two groups have recently published standardized techniques for rectal surgery, concluding that operative standardization may lead to an improvement in the quality of patient care.13,14 It is equally plausible that standardized video documentation portraying the key surgical steps in laparoscopic colon surgery will also lead to an improvement in the quality of patient care along with enhancing surgical training.
The video management system used in this study to document the operations had its own software, facilitating the video capture process, and could be readily started and stopped on the control panel. All operations were recorded for the full duration of each case, reducing potential bias by preventing the surgeon from selectively including or excluding specific operative portions. Video clips could be recorded directly into a digital format or converted easily into a different format without loss of quality. All of the recorded and edited videos in our study had a high resolution of 1440 × 1080 pixels, and with the introduction of large-capacity and high-speed hard disk and portable hard drives, video storage is no longer an impediment to documentation. 3 Fast processors and contemporary editing software allowed us to easily edit the recorded video clips. Although an optimal video management system would permit instantaneous video/audio editing to streamline synoptic surgical video production, we showed that one can document the key moments of an operation in a stepwise way.
Our study is one of the very few attempting to describe the feasibility and compliance of video documentation to capture the standardized steps of laparoscopic colon surgery. Standardization of this video documentation process using a checklist could have several important implications. The education of surgical residents and medical students could be enhanced if they are able to preoperatively review a video depicting the key operative steps and subsequently participate in the same surgical procedure. 2 The video may also help refine the surgeons' operative technique and improve performance through reflective analysis. 15 Surgical video need not only serve as objective documentation of what occurred in the operating room, in addition to the subjective, traditional operative note. 16 Video can help communicate with other physicians regarding the patients' anatomical changes and surgical outcome, thereby improving patient care and aiding in planning further intervention in the multidisciplinary setting.16–18 Increasing importance is being placed upon communication and education in the patient–physician relationship, which can be enhanced by showing the patient representative footage from his or her operation.
We believe that standardization and routine use of operative video documentation may also lead to improvements in the quality of patient care through qualitative and quantitative analyses. A recent example of this was seen in a study by Birkmeyer et al., 19 who examined the correlation between technical skill and postoperative outcomes using a representative operative videotape of surgeons performing a laparoscopic gastric bypass. A surgeon's technical skill was evaluated using this video, and the study findings suggested that greater skill was associated with decreased postoperative complications, reoperation, re-admission, and mortality. 19 It is also possible that increased attention by the surgeon at highlighted critical steps using video documentation may foster better patient care as was evidenced by Rex et al., 20 who attributed significantly improved colonoscopy performance to physician awareness of procedural video recording (the Hawthorne effect).
The primary goal of our study was to examine the feasibility of capturing the key steps in laparoscopic colectomy on video and produce a brief representative video depiction of the operation, but we would like to acknowledge several issues that may limit integration of routine video documentation into surgical practice. In our study, operating rooms were fully equipped with modern recording equipment and staffed with a surgical team familiar with operative video recording. We recognize that the costs of video equipment, operative capture, and data maintenance may be high for some hospitals and providers. This requires further careful investigation to determine expected time and resource expenditure. However, it is plausible that insurers would reimburse video capture costs if it can be demonstrated to improve surgical quality and patient outcomes. The hospital would likely then store and secure the full-length video data against alteration within the existing electronic medical record.
Video editing was performed in our study in a relatively short, although not negligible, time. Despite the ability of a short representative video to facilitate communication of operative findings, routine editing of all operations is not feasible for many practitioners as each video may require nearly an hour of production time. Thus, synoptic video editing will likely remain an adjunctive tool for surgeons and educators until live intraoperative editing programs become more available and therefore only a minor component in the drive for surgical quality in its current structure.
However, it is the standardization of an operation (e.g., through the use of stepwise checklists) not just within a hospital, but between many hospitals and surgeons, coupled with video documentation that provides the greatest opportunity to improve patient care and outcomes.
In conclusion, it appears that the majority of steps in laparoscopic right hemicolectomy and sigmoid colectomy can be documented following a checklist and using a standard video management system. These key steps may then be presented in a short representative video of an operation if desired by the surgeon or educator. The high-resolution video images obtained allowed for demonstration of the key components of an operation that may help improve the quality of care in patients undergoing laparoscopic colon surgery. Prospective studies are needed to demonstrate that standardization of the critical steps in an operation and their documentation can lead to an improvement in surgical quality.
Footnotes
Acknowledgments
We wish to thank Yuko Tonohira for her expert illustrating assistance.
Disclosure Statement
No competing financial interests exist.