
Abstract
Abstract
Background:
Although endoscopic thoracic sympathectomy (ETS) offers permanent cure of palmar hyperhidrosis (PH), compensatory hyperhidrosis (CH) often complicates the procedure. We analyzed the outcomes of a 2-month interval for unilateral sequential ETS (S-ETS) in comparison with simultaneous bilateral ETS (B-ETS), notably regarding CH and associated plantar hyperhidrosis, in treating patients with PH.
Patients and Methods:
Four hundred seven patients with intractable PH were randomly assigned into two groups: the B-ETS group (204 patients) and the S-ETS group (203 patients).
Results:
Three hundred sixty-four patients completed the study. Complication rates were comparable for both groups. No patient died perioperatively, and no conversion was necessary. Treatment success on follow-up was 97.2% for S-ETS and 96.7% for B-ETS. The incidence of CH was decreased substantially from 131 (71.1%) patients in the B-ETS group to 22 (12.2%) patients in the S-ETS group (P<.001), with no patient suffering severe CH in the S-ETS group compared with 33 (25.5%) patients in the B-ETS group. Eighty-four (58.3%) patients in the S-ETS group had simultaneous disappearance or decreased perspiration on the soles. All patients in the S-ETS group were satisfied, whereas 37.9% of B-ETS patients were unsatisfied with their operation, mostly because of CH and recurrences.
Conclusions:
Although both sympathectomies were effective, safe, and minimally invasive methods for treatment of PH, unilateral sequential ETS appeared to be a more optimal technique in terms of reduction of CH to a minimum and improvement of associated plantar hyperhidrosis.
Introduction
S
Since its first introduction by Kux, 3 endoscopic thoracic sympathectomy (ETS) has been considered a safe, simple, and effective method for treatment of PH. Although ETS offers permanent cure of hyperhidrosis, compensatory hyperhidrosis (CH) often complicates the procedure. CH occurs in 59.8%–90% of patients after sympathetic surgery4–6 and is manifested by increased sweating in parts of the body other than the hands, such as the back, abdomen, groin, and thighs. CH may make the patient regret having had the procedure. The mechanism of CH is not clear, but it seems to be associated with compensation for thermoregulatory function.7,8 Generally, the more sympathetic segments that are excised, the greater the incidence of severe compensatory symptoms.9,10 Some authors limited the extent of the resection for hyperhidrosis to reduce the incidence of severe CH.9,11,12 Many treatment methods, such as different levels of sympathectomy or sympathicotomy, ramicotomy, and clipping, have been attempted to reduce the extent of resection, although the effects of these methods remain controversial.1,13,14
The aim of this prospective randomized study was to compare the effect of unilateral sequential ETS (S-ETS) versus simultaneous bilateral ETS (B-ETS) on patient outcomes, notably CH and plantar hyperhidrosis, in treating patients with PH.
Patients and Methods
This prospective randomized study included 407 patients suffering intractable PH who underwent ETS at the Surgery Department of Mansoura University Hospital, Mansoura, Egypt, during the period from June 2010 to June 2013. All patients were unresponsive to medical treatment for at least 6 months. Three hundred one (73.6%) patients had experienced excessive sweating since childhood, and the remaining since their adolescence. Three hundred twenty (78.2%) patients complained of plantar hyperhidrosis associated with PH. Patients with pleural adhesions, bleeding diathesis, local infection, or previous operation for hyperhidrosis were excluded from the study. Patients' age, sex, and family history were recorded preoperatively. The patients were randomly assigned into two groups according to the surgical technique used: (1) the B-ETS group, which included 204 patients who underwent bilateral simultaneous T2–T3 ganglionectomy and (2) the S-ETS group, which included 203 patients who underwent unilateral T2–T3 ganglionectomy of the dominant side followed by T2–T3 ganglionectomy of the other side after a 2-month interval. The group selection was done using computer-generated series of consecutively numbered sealed envelopes. A detailed informed consent was obtained from all patients after explanation of the clinical condition and the options for treatment. Approval of the local ethics committee was obtained.
Surgical technique
The conventional ETS method by the two-port approach was the operative procedure performed. 2 Under general anesthesia with single-lumen endotracheal intubation, the patient was placed in the semi-Fowler's position with arms abducted. A 5-mm incision at the third intercostal space in the anterior axillary line was made through which a Veress needle was inserted, and the lung was collapsed by CO2 insufflation into the pleural cavity. Thereafter the Veress needle was then replaced by a 5-mm trocar through which a 0° endoscope was introduced into the pleural cavity. A second 5-mm trocar at the fifth intercostal space in the midaxillary line (at the level of the nipple) was inserted under vision for insertion of the diathermy probe. Because the first rib is usually difficult to visualize through thoracoscopy, the second and the third ribs were identified according to the anatomical landmark of the first rib by an area of bright yellow fat at the costovertebral junction. The sympathetic trunk and any Kuntz fibers were then transected at the bed of the second and third ribs using the conventional diathermy probe. The CO2 gas was then expelled from the chest cavity, the lung was expanded, and the port skin incisions were closed with single stitches. For the B-ETS group, the same procedure was then repeated on the other side at the same sitting. For the S-ETS group, the same procedure was repeated at another session scheduled 2 months later for the other side. Postoperative chest X-ray was performed routinely to rule out hemopneumothorax or incomplete lung expansion.
Patients were followed up for about 1 year postoperatively. The first follow-up assessment was performed by examining the patient in the outpatient clinic, and data were collected during an interview by an independent observer unaware of the surgical details. Follow-up was completed later by telephone interviews at 3, 6, and 12 months. Patients were asked to complete a questionnaire evaluating the results of sweating, CH, improvement of plantar sweating, degree of satisfaction, complications, and recurrence. The results of the intervention were evaluated by patients as follows: “dry” when the patient was not aware of sweat on the palms, “mild” when the patient had marked improvement whereby minimal sweat sometimes occurred under stressful conditions, and “no change” when the patient had limited improvement and was very aware of sweating (recurrence). Additionally, patients were asked whether plantar sweating was reduced. CH was graded as “severe” when the patient mentioned that sweating interfered with his or her normal activity, “moderate” when the patient indicated that his or her sweating was not bothersome, and “mild” when the patient did not mention dampness or made only a brief reference. Patient satisfaction regarding operative outcome was assessed by asking the patients to rate their level of satisfaction as very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied. Patients were considered satisfied if they reported being very satisfied or somewhat satisfied.
Results
Three hundred sixty-four patients completed the study. Regarding the B-ETS group, 184 patients completed the follow-up, whereas 12 patients had incorrect phone numbers, and 8 patients moved. In the S-ETS groups, 180 patients completed the study, whereas 7 patients did not attend for the second stage of the procedure, and 16 patients were lost during follow-up (10 had incorrect phone numbers, and 6 gone abroad). Demographic data are shown in Table 1. The age, sex, and family history were comparable between the two groups. All patients who completed the study had a follow-up period of more than 6 months in both groups. Complication rates were comparable for both groups. No patient died perioperatively, and no conversion was necessary. Residual pneuomothorax occurred in 8 patients; it subsided without intervention in 7 patients and with tube thoracotomy drainage in 1 patient. Pleural effusion and segmental lung atelectasis occurred in 2 patients and required tube thoracotomy drainage. One patient developed severe bradycardia during inflation of the pleural cavity, mostly because of inadvertent elevation of pressure, and was improved once pressure was released. No permanent Horner's syndrome occurred in any patient, and only 1 patient exhibited a mild miosis. Eleven patients suffered postoperative neuralgia, manifested by numbness along the inner side of the upper arm, and were treated by nonsteroidal analgesics, and neuralgia subsided within 2 weeks.
Data are mean±standard deviation values or percentages, as indicated.
B-ETS, simultaneous bilateral endoscopic thoracic sympathectomy; NS, not significant; S-ETS, unilateral sequential endoscopic thoracic sympathectomy.
Treatment success (lack of PH) on follow-up was 97.2% for S-ETS and 96.7% for B-ETS. Six (3.3%) patients had persistently wet hands in the B-ETS group, and 5 (2.8%) patients did so in the S-ETS group (Table 2).
B-ETS, simultaneous bilateral endoscopic thoracic sympathectomy; NS, not significant; S-ETS, unilateral sequential endoscopic thoracic sympathectomy.
The incidence of CH was decreased substantially from 131 (71.1%) patients in the B-ETS group to 22 (12.2%) patients in the S-ETS group (P<.001), with no patient suffering severe CH in the S-ETS group compared with 33 (25.5%) patients in the B-ETS group (Fig. 1). Eighty-four (58.3%) patients in the S-ETS group had simultaneous disappearance or decreased perspiration on the soles, with no patient in the B-ETS group reporting improvement in plantar hyperhidrosis. The degree of patient satisfaction is presented in Figure 2. All patients in the S-ETS group were satisfied, with no patient reporting being somewhat dissatisfied and very dissatisfied. About 37.9% of the B-ETS patients were unsatisfied with their operation, mostly because of CH and recurrences.
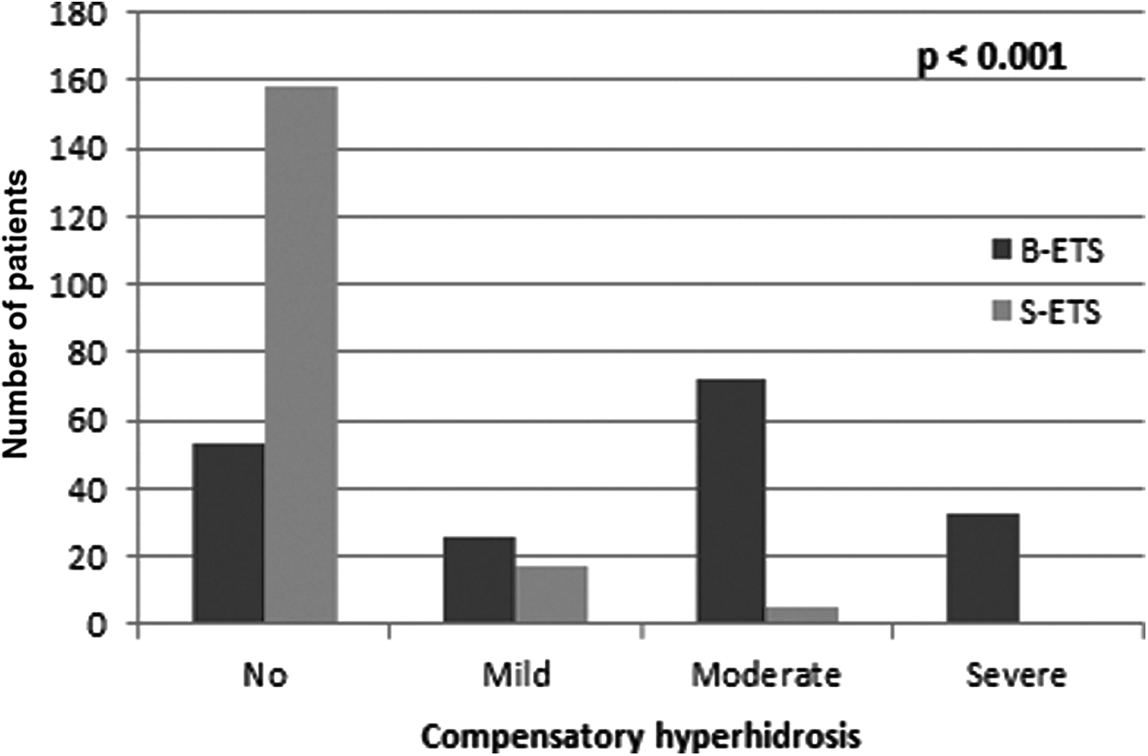
Compensatory hyperhidrosis among patient groups. B-ETS, simultaneous bilateral endoscopic thoracic sympathectomy; S-ETS, unilateral sequential endoscopic thoracic sympathectomy.
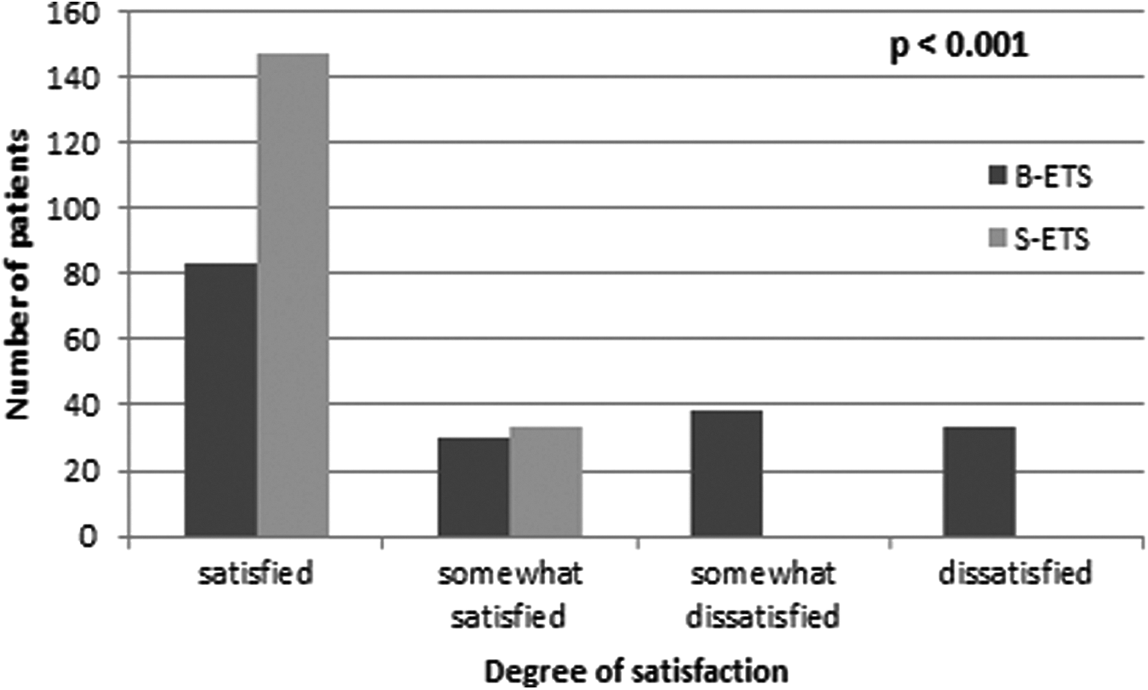
Patients' satisfaction. B-ETS, simultaneous bilateral endoscopic thoracic sympathectomy; S-ETS, unilateral sequential endoscopic thoracic sympathectomy.
Discussion
Although PH is a benign disorder and does not affect health, daily and social activities are affected. Therefore, a cure is usually desired. ETS has become established as a safe and effective treatment modality. Its success rate is greater than 95% in most series. 15 However, this less invasive approach has had no effect on the sequelae of the sympathetic denervation such as CS, phantom sweating, and cardiovascular reactions. 16 By far the most common complication after ETS is compensatory sweating, which occurs in 59.8%–90% of patients according to previous reports.4–6 In most patients, a mild variation of increased sweating is an unavoidable consequence of surgical sympathectomy to ensure the ablation of abnormal sweating of the palms. Nevertheless, severe reflex sweating may occur postoperatively in 10%–40% of patients. Instead of the palms, these patients start sweating in other areas, such as the lower back, buttocks, groin, and thighs, to such a voluminous degree that they are unhappy with the results of the surgery. Few treatment options exist for patients with this complication.11,12
It was proposed that sweating of innervated skin in the trunk and thighs increased to compensate for the abolished thermoregulatory function of denervated palms. Several efforts have been made to avoid the morbidity of CH following ETS. It is well known that T2 is the key ganglion responsible for the palmar sweating. Ablation of the T2 ganglion results in dryness of the palms. Many authors17,18 have concluded that the incidence of CH was correlated with the extensiveness of the sympathectomy. O'Riordain et al. 19 postulated that the low incidence of compensatory sweating might be explained by the limited extent of the sympathectomy and advocated that limited sympathectomy might minimize the incidence of CH. However, Lai et al. 20 did not show a significant difference in the incidence of CH between T2 and T2–T3 sympathectomy groups.
In the present study, CH occurred in 71.1% of patients in the B-ETS group with an incidence of 25.2% severe, 54.9% moderate, and 19.9 mild. The incidence of CH was decreased substantially to 12.2% of patients in the S-ETS group (P<.001), with no patient suffering severe CH. Moreover, 58.3% of patients in the S-ETS group had simultaneous disappearance or decreased perspiration on the soles. Therefore, unilateral sequential sympathectomy resulted in control of CH and improvement of associated plantar hyperhidrosis. This can be explained by the alteration of the quantitative distribution of thermoregulatory sweating in response to external heat following removal of T2–T3 ganglia. In other words, unilateral sympathectomy results in switch of the thermoregulatory sweating to the contralateral hyperhidrotic upper limb being flooded with the most ready sweat glands that can accommodate this extra sweating. Meanwhile, down-regulation of sweating in the trunk and lower limbs will be the counterpart of extra sweating in the hyperhidrotic upper limb. Two months later, when the contralateral limb is denervated, the end result will be dryness of both upper limbs and down-regulation of sweating in the innervated trunk and lower limbs. It is noteworthy that up-regulation of sweating in the deferred limb may pass unnoticed by the patient, as we usually start with the dominant hand so upgrading from mild to moderate or severe hyperhidrosis in the nondominant hand did not attract the patients' attention.
Conclusions
Although both sympathectomies were effective, safe, and minimally invasive methods for treatment of PH, S-ETS appeared to be a more optimal technique in terms of reduction of CH to a minimum and improvement of associated plantar hyperhidrosis.
Footnotes
Disclosure Statement
No competing financial interests exist.