
Abstract
Abstract
Background:
Epidemiological studies have shown an equal gender distribution of obesity in the United States; however, literature suggests approximately 80% of patients undergoing bariatric surgery are female. The aim of this study is to identify factors that contribute to this gender disparity.
Study Design:
A retrospective analysis of the Nationwide Inpatient Sample was performed. Obese patients who underwent open or laparoscopic gastric bypass or sleeve gastrectomy were identified using International Classification of Diseases, 9th edition codes. Patients <18 years of age were excluded. Female gender was used as a dependent variable to determine factors that influence gender distribution. Multivariate analyses adjusted for age, race, state within the United States, Charlson Comorbidity Index, income level, and insurance status.
Results:
From 1998 to 2010, 190,705 patients underwent bariatric surgery (93% gastric bypass, 7% sleeve gastrectomy). Females made up 81.36% of the population. An 80% to 20% female to male distribution was maintained for every year (1998–2010) and was unchanged within individual states. Patients were more likely to be female if from a lower-income neighborhood or if African American or Hispanic (P<.05). Patients were less likely to be female with increasing age, more comorbidities, or private insurance (P<.05).
Conclusions:
The unequal gender distribution in bariatric surgery patients is influenced by demographic and socioeconomic factors. This disparity is narrowed in patients who are older and have more comorbidities, whereas the disparity is widened for certain races and lower incomes. Given the equal distribution of obesity in the United States, the widespread gender gap in bariatric surgery may suggest an underuse in obese men.
Introduction
T
Epidemiological studies have shown that the gender distribution of obesity approaches 50%/50% men/women.4–8 However, the gender distribution among patients undergoing bariatric surgery is approximately 20%/80% men/women.9,10 Unfortunately, many patients who could clearly benefit from a bariatric procedure face barriers to access.9,11 Preoperative disparities in eligibility have been reported previously.9,12 Specifically, socioeconomic and demographic factors have been shown to be significant barriers to bariatric surgical interventions.9,11
The purpose of this study is to examine prehospital nonbiological factors that may be associated with this skewed gender distribution. Therefore, we hypothesize that nonbiological factors contribute to the gender disparity of bariatric surgery in the United States and that patients who undergo bariatric surgery are not representative of the total eligible bariatric population. Important socioeconomic variables, such as urbanization, ethnic background, and poverty levels, differ significantly among regions within the United States, and surgeons' decision-making process for bariatric surgery may be influenced by these variables.
Materials and Methods
We performed a retrospective analysis of the Nationwide Inpatient Sample (NIS), a nationwide database sponsored by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project, which provides a representative 20% sample of hospital discharge records from 37 states. 13 The NIS provides information for each hospital admission, including age, gender, race, income, insurance status, comorbidities (listed as secondary diagnoses), hospital location (rural or urban), and hospital type (teaching or nonteaching). The data were enriched by calculating the comorbidities of patients using the Charlson Comorbidity Index as per the adaptation for administrative datasets of Deyo et al. 14 This study was deemed exempt by the University of California, San Diego Institutional Review Board.
Case selection
We searched the period 1998–2010 using the International Classification of Diseases, 9th edition (ICD-9) procedure codes including all subcategories of procedures and identified obese patients who underwent inpatient bariatric surgery, either open or laparoscopic gastric bypass or open or laparoscopic sleeve gastrectomy (ICD-9 procedure codes 44.31, 44.38, 44.39, 43.82, 43.89; diagnosis codes 278.0, 278.00, 278.01, and 278.02). For laparoscopic bariatric procedures without defined ICD-9 procedure codes and for data collected prior to the existence of defined laparoscopic categories, we used the generic laparoscopic code (54.21) in addition to the specific open procedure code. We excluded patients younger than 18 years of age, patients who underwent emergency operations or multiple bariatric operations during the same hospital admission, and operations performed for charity (defined as total hospital charges <$1,000).
Dependent variable
An interesting aspect of our study is the designation of female gender as the primary outcome. Although dependent variables are typically factors that can change based on the influence of several patient- and hospital-level factors, gender is obviously distinct in this regard. In order to find prehospital nonbiological factors that contribute to the gender disparity in bariatric surgery and thereby identify potential target populations for narrowing the gender gap, female gender was used as the outcome for statistical analysis. Using gender as a dependent variable, contributing factors to the skewed gender distribution can be identified and further analyzed in multivariate analyses.
Statistical analysis
Student's t test (for continuous variables) and the chi-squared test (for nominal or categorical variables) were used for all bivariate analyses. Logistic regression analysis was performed to determine the independent predictors of female gender after bariatric surgery when adjusted for age, sex, race, state within the United States, insurance status, hospital volume, poverty level (defined as people living in various degrees of poverty within their specific county), laparoscopic approach, and comorbid disease as measured by the Charlson Comorbidity Index score. Using female gender as a dependent variable, an odds ratio of 1 would imply the skewed gender distribution, 80% female and 20% male, found in our collective. Odds ratios lower than 1 would imply factors that narrow the gender gap, and ratios higher than 1 signify factors that increase the gap. Subset analyses were repeated for each state. All tests were two-sided, with statistical significance set at P≤.05. All statistical analyses were performed with Stata MP version 11.2 software (StataCorp, College Station, TX).
Results
Study population
In total, 190,705 obese patients were identified from the NIS sample who underwent open or laparoscopic gastric bypass or sleeve gastrectomy from 1998 to 2010. The majority of patients underwent a gastric bypass and had a laparoscopic approach. The mean age was 42.8 years (range, 18–94 years), and the majority of the patients were white, with private insurance and with minimal comorbidities. The gender distribution was skewed, with greater than 80% females. This 80%/20% female/male distribution was maintained for each year of the study and was consistent within every state in the United States. Details are shown in Table 1.
Age is given as mean (minimum, maximum).
Unadjusted comparison
The percentage of females undergoing surgery in the study population was 81.14%, whereas the gender distribution of obesity was equal according to the Centers for Disease Control and Prevention data (Fig. 1). It was highest in patients under the age of 45 years (83.85%) and was lowest (68.29%) among patients over 74 years of age, as shown in Figure 2. When analyzing the effect of race on gender, a narrowed gender gap was found in the Asian patients, whereas the gap was widened for other races (Fig. 3).
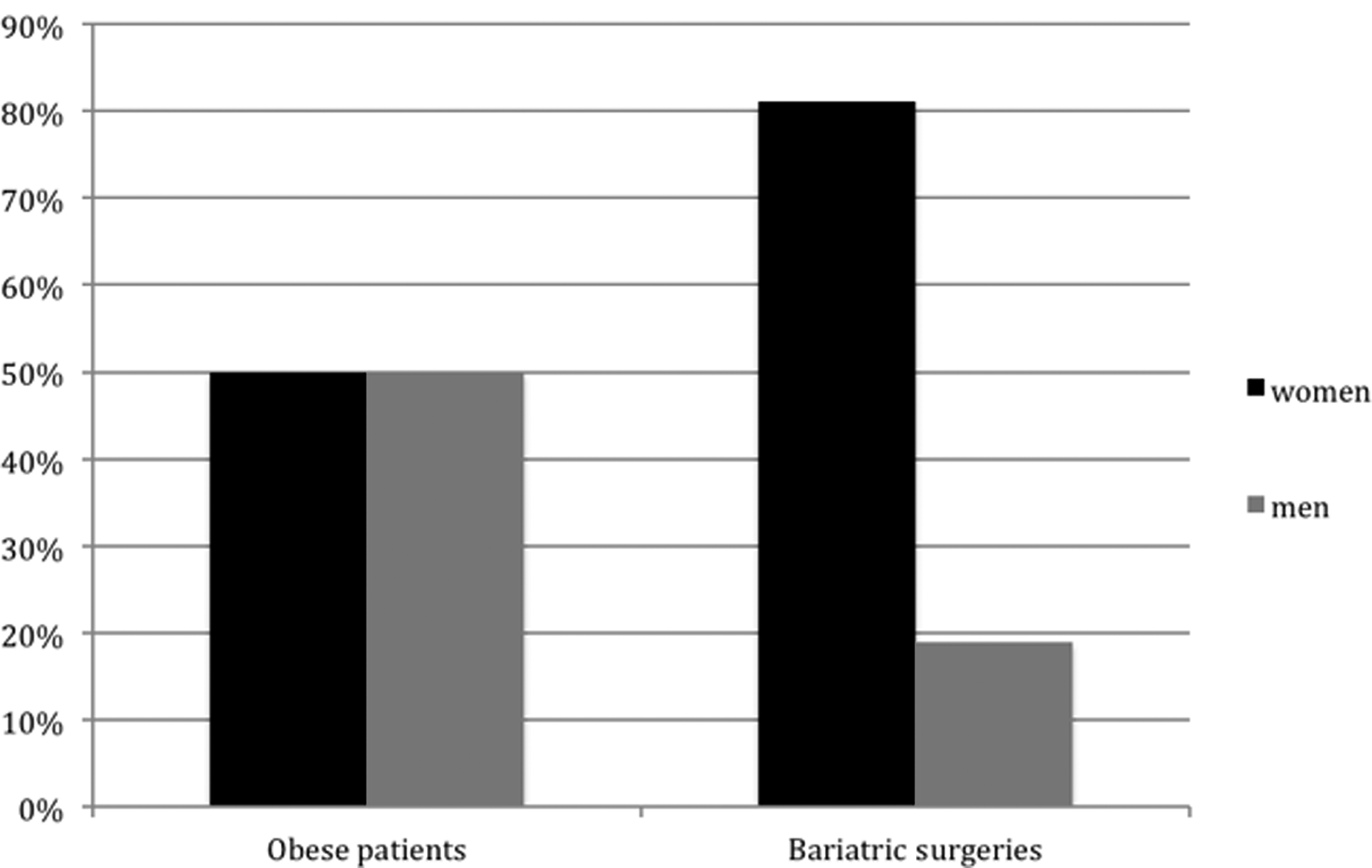
Skewed gender distribution in bariatric surgery patients in our collective (compared with equal gender distribution in obese people according to 2010 Centers for Disease Control and Prevention data 8 ).
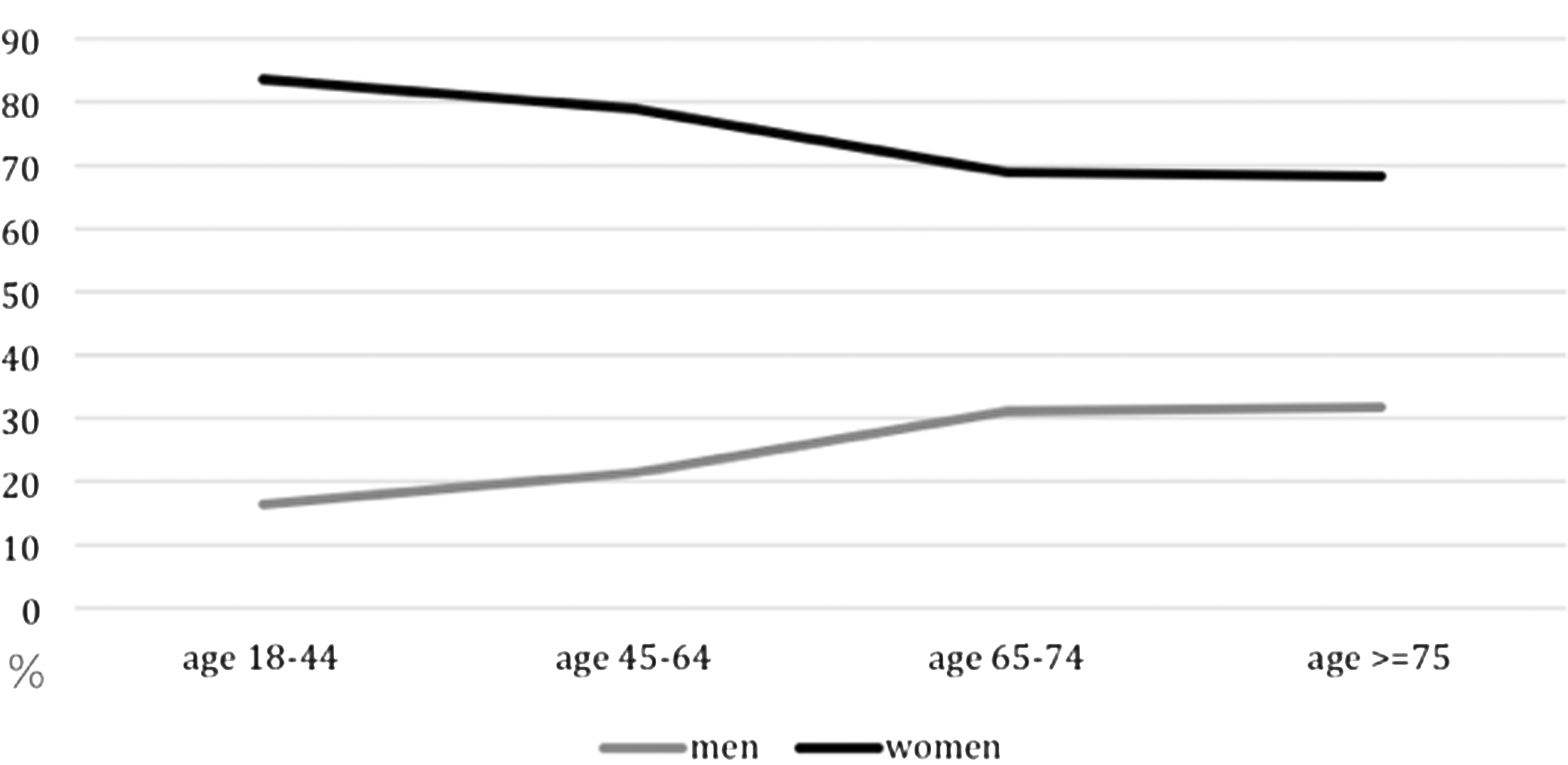
Narrowed gender gap in older patients (unadjusted data).
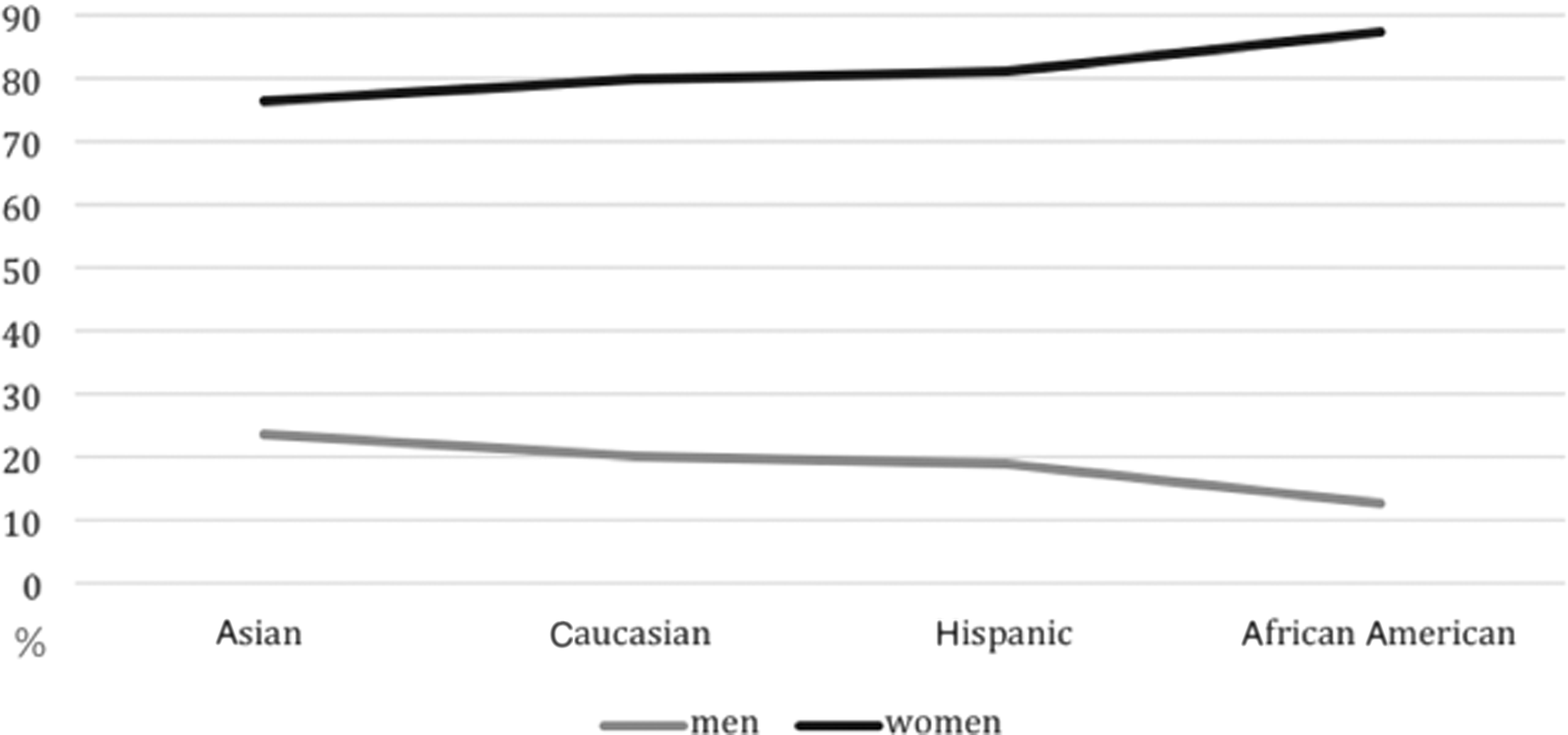
Gender gap depending on race (unadjusted data).
Adjusted outcomes
After adjusting for age, comorbidities, race, state where operation was performed, hospital volume, laparoscopic procedures, and insurance status, a significantly higher female percentage was observed in counties with lower median income as well as in Hispanic or African American patients. When adjusting for the same covariates as listed above, a significantly lower female percentage is found in patients who are older, are Asian, and have private insurance and with more comorbidities. A detailed overview is given in Figure 4. As previously described, odds ratios lower than 1 imply factors decreasing the gender gap, and ratios higher than 1 imply factors increasing the gap. In other words, an odds ratio lower than 1 means a gender distribution less skewed than 80/20. The gender distribution never flipped to the other side (more men undergoing surgery) in any subgroup.
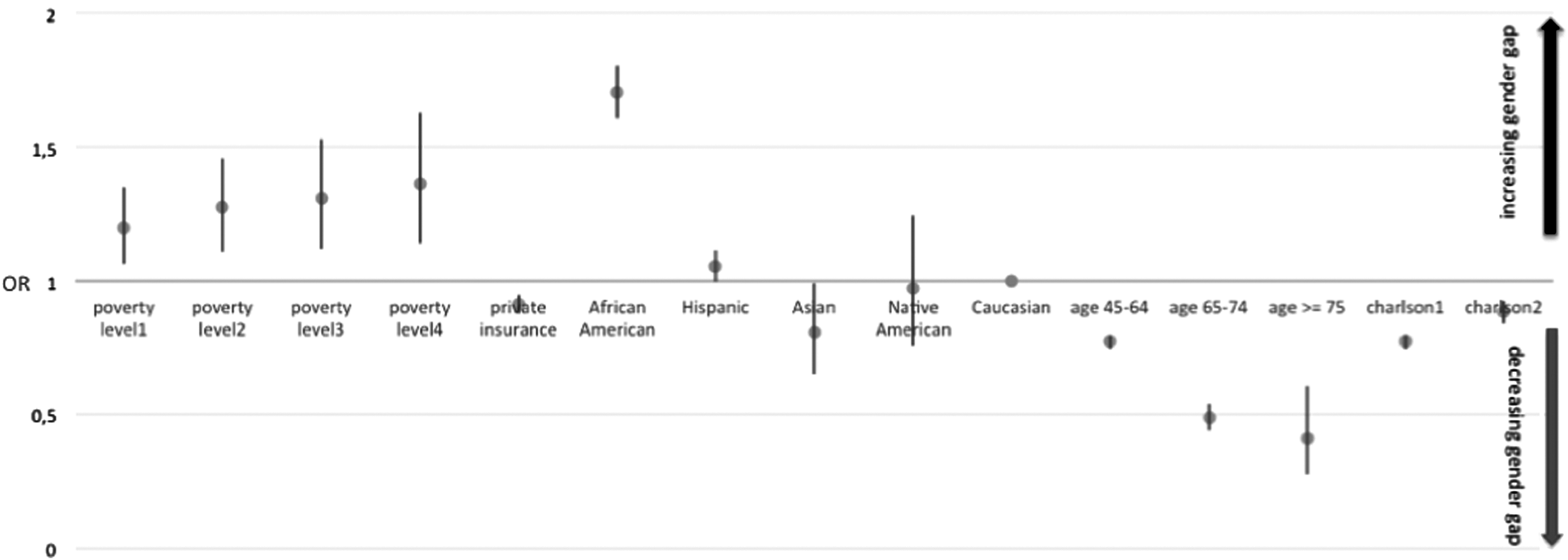
Adjusted factors contributing to gender gap. An odds ratio (OR) lower than 1 implies a factor decreases the gender gap, and an OR higher than 1 implies the factor increases the gap.
When the gender gap is analyzed by state, in comparison with California, the gap is significantly narrowed in Arizona, Connecticut, Florida, Illinois, Kansas, Louisiana, Massachusetts, Missouri, New Hampshire, New Jersey, Nevada, New York, Pennsylvania, and Utah. No state has a significantly increased gender gap, when compared with California.
Discussion
To our knowledge, this is the first study that further analyzed the bariatric surgery gender disparity in sleeve gastrectomy and gastric bypass patients on a national level. We clearly identified which socioeconomic and demographic factors significantly increase or decrease the gender gap in obesity surgery. Existing studies either were single-institution case series or did not include nationwide data and were unable to determine reasons for the gender distribution observed in bariatric surgery or how certain factors influence the gender gap.15–17 In addition to gastric bypass, we included an emerging bariatric procedure, sleeve gastrectomy, which currently comprises the largest proportion of bariatric surgeries in the United States according to the American Society for Metabolic and Bariatric Surgery. 18
Recent studies examining national trends in bariatric surgery repeatedly report disproportionate and increasing use of bariatric surgery among women, without analyzing reasons for the high percentage of females.19,20 Santry et al. 19 found an astonishing rate of 84.1% females in their 2002 nationwide collective. These numbers indicate that the tremendous increase in rate of bariatric procedures in the past two decades represents bariatric procedures performed on women. 15 A large proportion of patients who underwent bariatric surgery in North Carolina in recent years had higher socioeconomic status, were younger in age, and had no comorbidities; all of these factors we also determined significantly influenced the gender gap, which corroborates our findings. 15
One possible explanation for the high rate of females undergoing bariatric surgery is greater eligibility. In a recent analysis of racial trends in bariatric surgery in the United States, Mainous et al. 20 found that overall a larger proportion of females were eligible for bariatric surgery, and according to the National Hospital Discharge Survey and National Health and Nutrition Examination Survey databases, this is consistent within each race. Additionally, a significantly higher proportion of women than men received bariatric surgery from their eligible population. Martin et al. 9 found 62% of their female population and 38% of their males eligible for bariatric surgery, which still does not explain the 80%/20% gender gap in bariatric surgery. Their study did not further comment on this mismatch.
Surgeons' preferences to operate on certain patient groups in addition to sociocultural pressure may also play a role, as we found a higher percentage of females in the younger subcategory. A national survey performed among U.S. bariatric surgeons revealed that gender was not a factor that influenced patient selection within bariatric patients who fit into National Institutes of Health clinical guidelines. However, gender was a factor for patient selection in those with a body mass index of ≤35 kg/m2 without comorbidities, with men having 67% decreased odds of selection. 21
Additionally, barriers in access to healthcare for certain subgroups have been reported. 22 Men were less likely to have health insurance coverage than women over the entire study period in the United States 23 : according to U.S. Census data, 17.7% of males were uninsured, whereas only 14.9% of females were uninsured in 2010. This fact suggests that males may be less likely to seek healthcare. Cultural differences and viewpoints also could affect willingness to seek medical care; a persistent lack of trust of physicians by African Americans has been reported previously, leading to decreased adherence to treatment recommendations. 24 Cultural influences also play a role in body image acceptance, for example, the effect of body image suspected in the racial disparity study of Mainous et al., 20 presuming that African Americans may have less motivation to get a bariatric operation because obesity is more culturally accepted among their population. 25 Our finding—that the gender gap is wider for African Americans—is supported by a recent study 27 about body satisfaction in the United States, that African American men are more satisfied with their body image than African American women (score of 3.9/5 versus 3.24/5), whereas this relation is closer for whites (men versus women, 3.44/5 versus 3.29/5). It is plausible that cultural differences and racial differences may accentuate the gender disparity.
Body image is different in men and women, possibly contributing to the underuse of bariatric surgery in males, as they typically are more satisfied by their body image than women. 26 Fallon et al. 27 found that 72.8%–94.0% of overweight and obese men and 56.7%–85.0% of overweight and obese women were satisfied with their health. This skewed male body perception hinders the likelihood of seeking healthcare advice. As being thin is particularly valued in women and connotes control and competence, it is logical for females to desire to reach this goal and thus seek surgical assistance if unable to do so otherwise.28,29 Although we did not directly measure body image in our study, there are some findings that suggest that this may be at play. For example, the observation that the gender gap is largest in California is consistent with the notion that body image consciousness within California's population is high. 30 The effect of ongoing underuse of bariatric surgery in men could be partially responsible for the reported plateau in procedures since 2003. 3 Consequently, there is potential for further growth of the bariatric surgery market if males become a target population.
Other findings of interest of this study include that worsening poverty level increases the gender gap. Additionally, a covariate associated with higher income—private insurance—decreases the gender gap. These findings taken together may reflect that females are poorer than males in the United States in general.31,32 Furthermore, female patients who underwent bariatric surgery are generally in better health than males as measured by the Charlson Comorbidity Index. This suggests that men may seek bariatric surgery late, as a means to achieve improvement in comorbid conditions instead of as a preventive weight loss therapy alone. This emphasizes the fact that bariatric surgery should not be promoted for body image only, but for improvement in health as well.
A strength of our study is the extensive number of patients in our analysis. The large patient population allows for accurate determination of factors that influence the gender gap in bariatric surgery. Additionally, the nationwide nature of this study makes our findings generalizable. Furthermore, inclusion of sleeve gastrectomy in addition to gastric bypass better reflects current surgical practice than if our analysis included only those who underwent gastric bypass. A limitation of our study is that large administrative claims-based databases are dependent on accurately entered codes. 33 The NIS is limited to inpatient procedures; this is the reason we did not include laparoscopic adjustable gastric banding patients, as this procedure is typically performed in an outpatient setting. Furthermore, the NIS database does not provide us with weight data necessary to assess the validity of a bariatric protocol. The detailed demographic and socioeconomic information provided by the NIS allowed us to ascertain the reasons behind the gender disparity in bariatric surgery, whereas purely descriptive studies were unable to do so.
Our study has important implications. The implication of body image in this gender disparity suggests that men may, erroneously, think that the sole aim of bariatric surgery is to improve body image, not recognizing the long-term negative health consequences of obesity. There are some findings to support this possibility in our study. For example, among patients with comorbidities, there is a smaller gender gap, suggesting that men are more likely to wait to seek care until their comorbidities develop. Therefore, a possible intervention would be a public health campaign to educate the public, specifically men, about the fact that bariatric surgery is not an operation to improve body image, but, rather, it is an important tool to treat and prevent health maladies.
Conclusions
The extensive and pervasive gender gap in bariatric surgery may suggest an underuse in obese men, given the equal gender distribution of obesity in the United States. There are multiple socioeconomic and demographic factors that contribute to the gender disparity, including poverty, insurance, race, age, and comorbid conditions. Although the obesity rate continues to increase in the United States, we now face a plateau in the number of bariatric procedures performed. To further improve the reach of bariatric surgery, our findings suggest that male patients should become the target for outreach. Bariatric surgery needs to be better promoted to eligible male patients in order to remedy the currently existing widespread gender disparity.
Footnotes
Disclosure Statement
No competing financial interests exist.
H.F.F., R.C.B., C.R.H., and D.C.C. were responsible for study concept and design. All authors were responsible for acquisition, analysis, and interpretation of data and for drafting of the manuscript. D.C.C., S.H., B.J.S., G.R.J., and H.F.F. were responsible for critical revision of the manuscript for important intellectual content. D.C.C. and H.F.F. were responsible for statistical analysis. H.F.F. was responsible for administrative, technical, or material support. S.H. was responsible for study supervision. S.H. and D.C.C. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.