
Abstract
Abstract
Background:
Morcellation of a bulky uterus after total laparoscopic hysterectomy (TLH) is a challenge for those dealing with advanced laparoscopic surgery. However, there are no laparoscopic standardized procedures available to date. We developed a laparoscopic cold knife technique with the aim of demonstrating a simple and reproducible method of sectioning and vaginal retrieval of the bulky uterus.
Materials and Methods:
From June 2012 to June 2014, patients who underwent TLH for benign indication, with a uterus size over 12 gestational weeks, were prospectively admitted into the clinical study. Before specimen vaginal retrieval, uterine section was achieved by Chardonnens' cold knife with the aim of obtaining two uterus halves sectioned longitudinally and held together only by the posterior cervical wall. We performed the procedure in a containment system to avoid myometrial spillage into the abdomen.
Results:
Twenty-nine women with a bulky uterus were treated by TLH and the cold knife section technique. The uterine size ranged from 240 to 850 g (median, 460 g), and the average morcellation operative time was 11.3 minutes. All procedures were completed successfully without complications.
Conclusions:
Our data suggest that the cold knife uterine section technique after TLH is a feasible, simple, and reproducible method of bulky uterus morcellation, even if further research is advisable to fully evaluate the advantages of this procedure.
Introduction
T
Several tips and tricks have been reported in the literature to achieve TLH in the presence of an enlarged uterus, but few studies have described standardized morcellation steps. Then available options for bulky uterus morcellation and retrieval during laparoscopy may include a vaginal or an abdominal approach.
In order to extract the bulky uterus through the vagina, it usually has to be reduced in size, especially in nulliparous patients or those with a narrow vagina. The literature reports several vaginal morcellation techniques, including uterine bisection, cervical amputation with bivalve rotation, intramyometrial coring, wedge resection, “helical” incision, or the “paper roll” technique.1–3
However, abdominal morcellation has rarely been described and it includes manual minilaparotomy, power, or cold knife laparoscopic morcellation.4–8
The topic of morcellation has recently assumed greater relevance after the U.S. Food and Drug Administration's (FDA's) statement discouraging the use of power morcellation for hysterectomy and myomectomy. 9
The aim of this report is to describe our laparoscopic cold knife section technique to reduce the uterine size in patients undergoing TLH for a bulky uterus.
Materials and Methods
From June 2012 to June 2014, patients who underwent TLH for benign indication at the Department of Gynecology and Obstetrics (Alessandria, Italy), with a uterus size larger than 12 gestational weeks at clinical examination, were prospectively admitted to the clinical study, after written informed consent (Canadian Task Force Classification III) was obtained. The inclusion criterion was a bulky uterus larger than 12 gestational weeks with myomas at the clinical examination, which was performed by the same senior gynecologist. Exclusion criteria were cervical, endometrial, and ovarian cancer or a suspicion of a malignant myometrial tumor at preoperative assessment, any systemic infections, contraindications for general anesthesia and/or a prolonged Trendelenburg position, and a patient who did not require uterus morcellation at clinical examination.
The patients' characteristics were reviewed, and intraoperative, postoperative, and follow-up data were collected, including patient age at diagnosis, parity, body mass index, surgery procedure time, uterine weight, decreasing hemoglobin level, and complications. The preoperative assessment included a physical examination, Pap test, transvaginal ultrasound scan, and office hysteroscopy with endometrial biopsy. The patients received prophylactic antibiotic administration 1 hour preoperatively.
Our technique for TLH in the presence of a bulky uterus followed the usual procedure for a standard TLH. After the colpotomy, a cylindrical sterile wrapping bag (50 × 27 cm) with a drawstring thread, forming a running noose, placed around the two open ends of the pouch, was inserted through the umbilical trocar and stretched to envelope the uterus (Fig. 1). The drawstring thread of the cranial “V-shape” end of the bag was left outside the pelvis along the umbilical trocar, and the drawstring thread of the caudal circular end was pulled through the vaginal canal, closing the caudal end of the pouch around the cervix. The anterior wall opening was obtained by pulling out the two threads connected to the bag through the ancillary trocars, allowing the uterus to be sectioned by the laparoscopic knife.
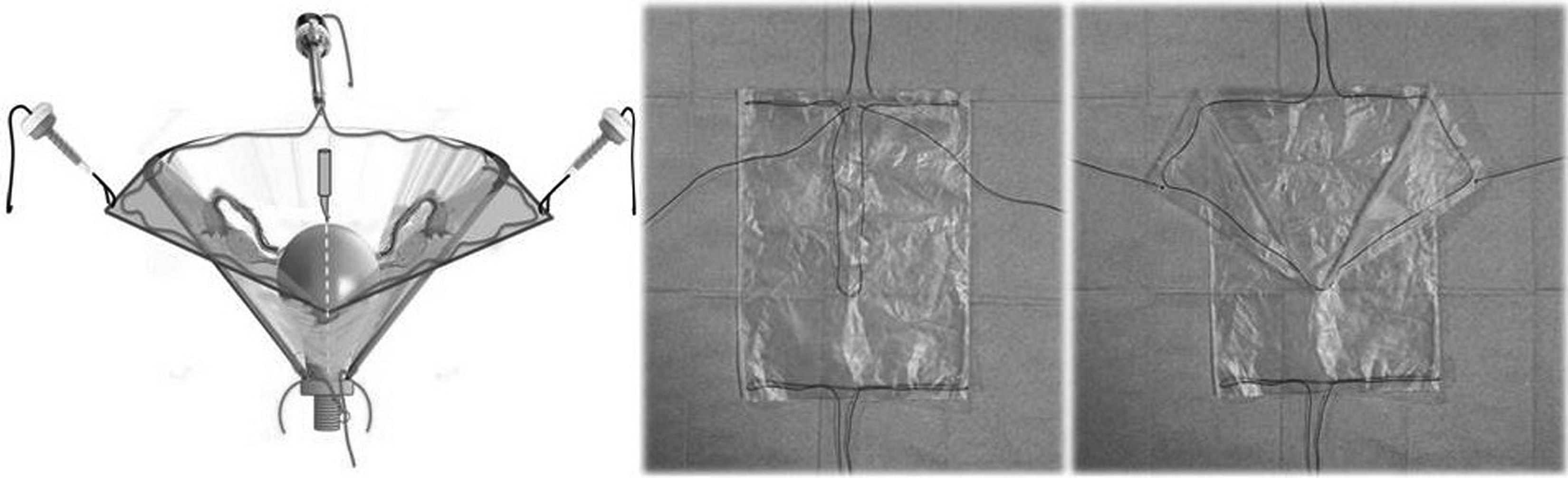
Our developed containment system that we adopted to improve the safety of the technique.
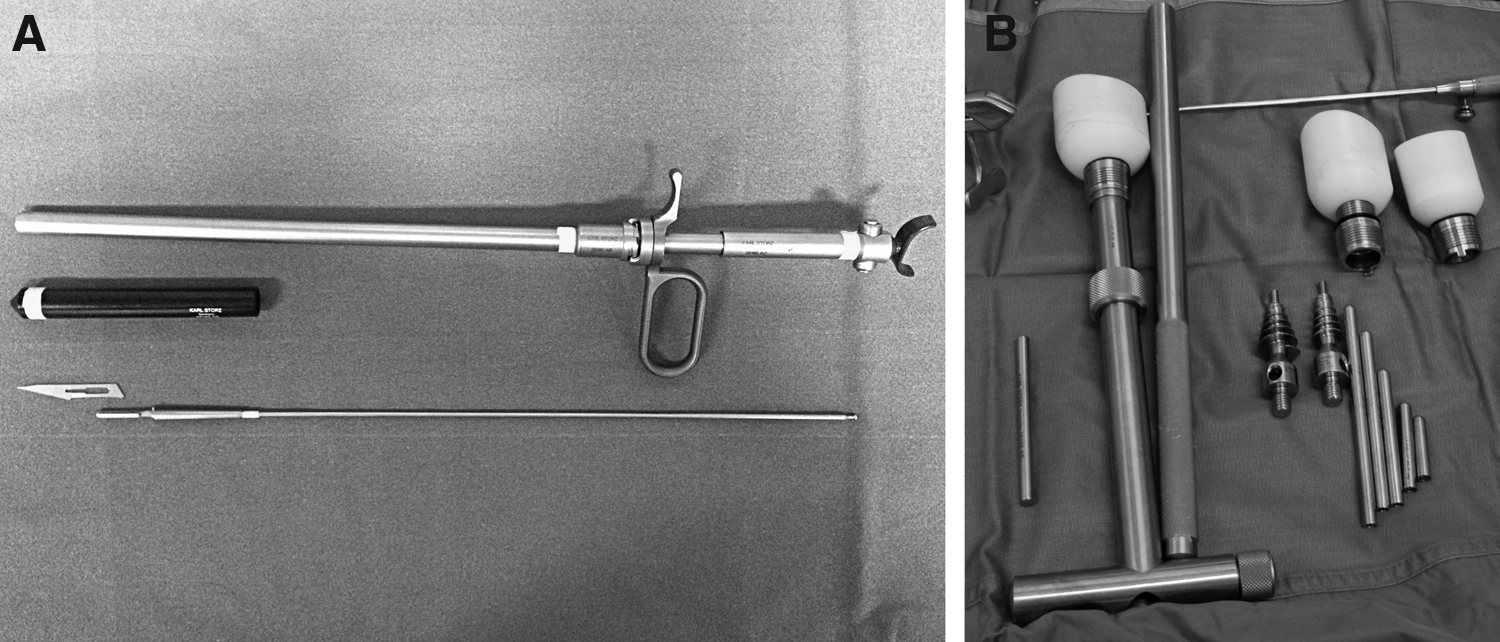
The Chardonnens' cold knife (Karl Storz, Tuttlingen, Germany) was introduced through the 10-mm-diameter soprapubic trocar (Fig. 2A). A standard number 15 blade was fastened to the scalpel and then inserted into the outer tube; then the protective cap was fixed to avoid any injury during the assembly. The uterine size reduction technique was done by holding the uterus firmly anchored onto the manipulator axis (HOHL uterine manipulator; Karl Storz) to obtain a longitudinal direction during incision, and the cup was left in the vagina to maintain the pneumoperitoneum (Fig. 2B).
The cutting movements were always made along the sagittal plane, starting from the fundus to the cervix, along the uterine anterior wall in a cranial–caudal cutting direction, to avoid damaging the bowel or blood vessels (Fig. 3A). Once the blade had reached the uterine cavity, the posterior uterine wall was divided up to the cervix. Two 5-mm-diameter grasping forceps held the edges of the uterine breach, and the tension between the two forceps was kept constant during the incision to increase the cutting efficiency (Fig. 3B).
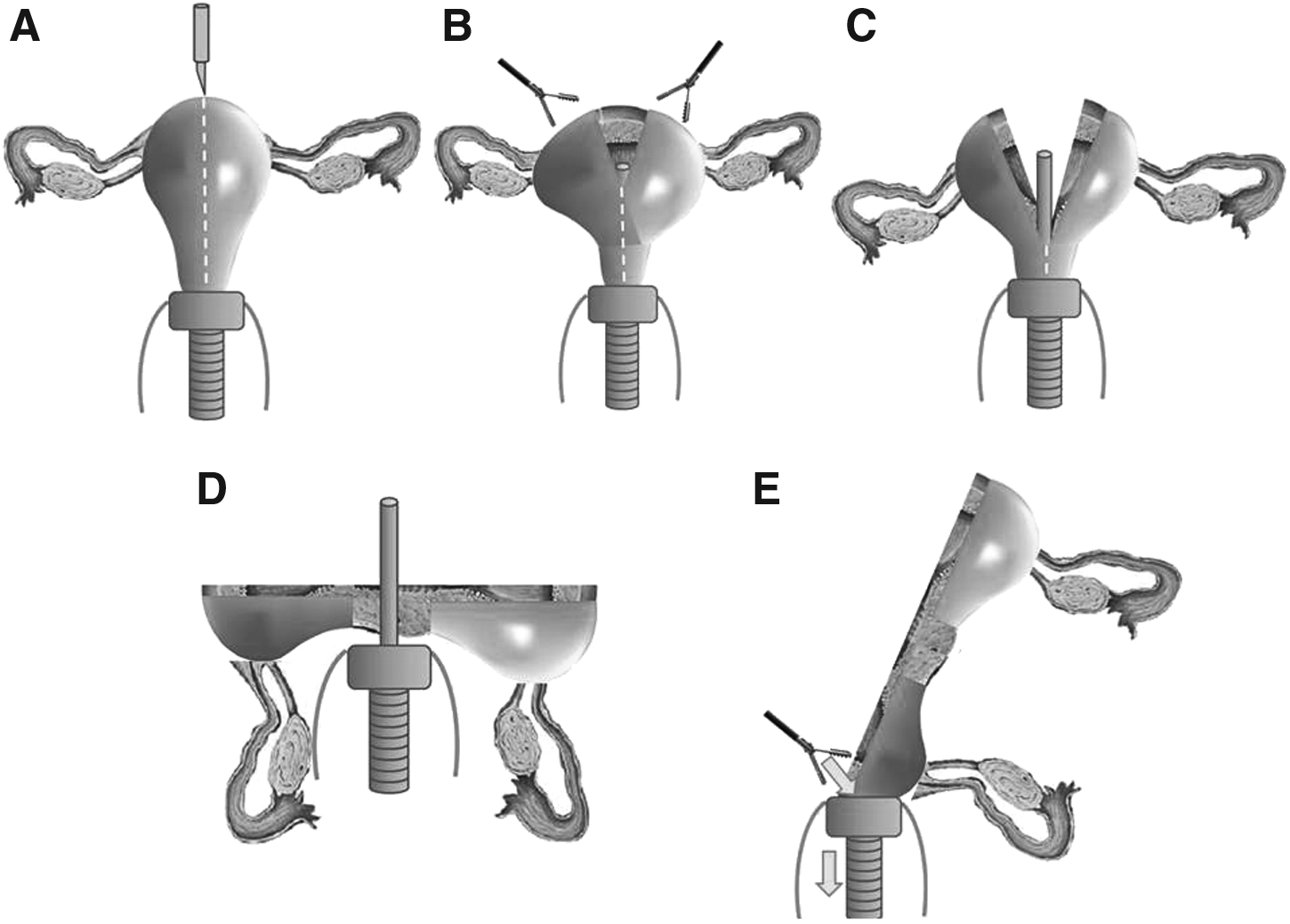
Once the anterior portion of the cervix had also been incised, the uterus was freed from the manipulator axis and rolled along in a laterolateral direction (Fig. 3C and D). This allowed us to obtain two uterus halves along the longitudinal axis held together only by the posterior cervical wall. The last step was to push down one side of the surgical specimen into the circular manipulator cup with a grasper and then into the vaginal canal for retrieval (Fig. 3E), after which the drawstring thread of the cranial end was pulled, and the cranial part of the pouch was closed.
The specimen, anchored with Pozzi graspers, was removed through the vagina by rotational and circular movements, without the application of valves and after having deflated the Foley catheter to avoid transient hematuria. The colpotomy was closed transvaginally with a synthetic medium-term reabsorbable suture followed by a laparoscopic McCall colposuspension.
All specimens were sent for pathologic examination in two divided halves without fragmentation of the myometrium.
Approval for the study was obtained from the Institutional Review Board. Descriptive statistics were used to analyze our data.
Results
During the study period, in total, 32 women were scheduled for TLH because of a bulky uterus with the cold knife section technique, and only 3 patients (9.3%) were excluded because of not requiring uterus morcellation at the conclusion of the surgical procedure. Thus the number of patients enrolled for the study was 29. We adopted a containment system for the last 4 patients. The mean age of the patients was 50.1 ± 4.8 years, with a body mass index of 25.8 ± 6.3 kg/m2 and a median parity of 1 (range, 0–4). Four women were nulliparous (13.8%), and the 34.4% of women had a previous abdominal surgery. Uterine size ranged from 240 to 850 g (median, 460 g).
Intraoperative and early postoperative data are reported in Table 1. No surgeries required conversions to open surgery, and no intraoperative or postoperative complications were recorded.
SD, standard deviation.
Discussion
A major hurdle to the development of laparoscopic surgery is the volume of tissue that must be removed from the abdomen and the availability of extraction techniques.10,11 As demonstrated by Condous et al., 12 the probability of morcellation is close to 1 (about 99.5%) for both parous and nulliparous women with a uterine weight of >350 g.
The use of morcellators has acquired more importance since advances in laparoscopic surgery and various morcellation techniques for the bulky uterus by the vaginal approach and/or abdominal laparotomic or laparoscopic approach have been reported. Indeed, the literature describes numerous vaginal techniques for the reduction of uterine size before extraction through the vagina. The vaginal route is one of the most accessible ways to enter into the pelvic cavity with no need to enlarge abdominal ports, with less postoperative pain and no negative effect on sexual function. 13 During the vaginal “uterine bisection,” the uterus is sagitally sectioned, and each hemi-uterus is extracted after morcellation and large myoma enucleation. In the “intramyometrial coring morcellation,” the deep myometrium is separated from the superficial layers and serosa by an isthmic circular incision 1 ; the mechanics involved in the “helical incision” and “paper roll” techniques are similar to those used with the electrical morcellator, which peels off the superficial part of the specimen while rotating. The “wedge morcellation” is done by removing wedges of myoma and myometrium from the anterior and posterior uterine wall.2,3
The change from the laparoscopic to the vaginal route and the time required for the vaginal morcellation techniques make the vaginal morcellation a time-consuming technique. 14 Moreover, although effective and fairly safe, the vaginal route may present more difficulties, especially in the presence of a narrow vagina.
The abdominal approach by “minilaparotomy” or a small abdominal incision can be used to extract the uterine tissue. 5 This can be performed by extending a trocar incision or by making an incision in another location, sometimes with the use of a self-retaining retractor. The size and location of these types of incisions may dictate different risks, such as infection and incisional hernia. Furthermore, any type of open morcellation through an abdominal incision may involve exposing the tissue to the peritoneal cavity, presenting a similar risk as that of specimen fragments remaining in the intraperitoneal cavity.
Various morcellators have been developed in the abdominal laparoscopic approach. Although monopolar electrodes are a common cutting method, they produce large amounts of smoke and carry the risk of distant electric injury. Laparoscopic power morcellators do facilitate the removal of large sections of tissue from the abdomen through existing incisions 15 ; however, related injuries to surrounding structures during laparoscopy are a frequent event.6,16 The two main complications (i.e., visceral and major vessel injuries) are often related to surgeon inexperience. Gas leakage during the extraction of pieces may pose a problem, and maintenance of pneumoperitoneum is important for a safe morcellation. 15
The laparoscopic power morcellator systems are expensive and time consuming because the specimens can be morcellated at a rate of only about 25 g/minute, and any scattered pieces in the abdomen must be removed, lengthening the procedure time. 6 Moreover, parasitic leiomyomatosis and diffuse endometriosis have been reported after accidental tissue piece leakage into the abdominal cavity. 17
The power morcellation has recently come under scrutiny after the FDA statement discouraged its use for hysterectomy and myomectomy to avoid dissemination of occult uterine cancer, significantly worsening patient prognosis with an increased risk of recurrence and shorter progression-free survival when compared with en bloc resection.18–20
Some surgeons prefer to use the cold knife morcellation, mainly to reduce costs and risks of electrical damage. 8 Morcellation with the Chardonnens' knife produces no smoke, heat, or stray electric current that might be harmful to adjacent structures. However, the safety level of this procedure depends on the ability and experience of the surgeon; no reproducible and standardized techniques have been described in the literature to date. The cold knife morcellation may be associated with the same rate of complications reported for the use of power morcellators, such as vascular and bowel injuries or spillage of specimen material into the abdomen. That is why the aim of our study was to standardize the technique to reduce both procedure time and complications.
Our data suggest that the laparoscopic cold knife technique with transvaginal specimen removal is a simple, reproducible, and quick method to reduce the volume of a bulky uterus or when there is a disproportion between the vaginal width and uterine transverse diameter.
Indeed, we reported an average uterine section operative time of 11.3 minutes for a median uterine size of 460 g, which is significantly faster than tissue removal at the rate of 25.9 g/minute for the Gynecare Morcellex (Ethicon, Somerville, NJ) device or of 28.4 g/minute for the Rotocut G1 (Karl Storz). 7
Furthermore, our standardized technique may well minimize the risk of visceral or vessel injuries and specimen fragmentation in the peritoneal cavity.
We believe that after the FDA statement, this technique has acquired more interest as it may represent a viable alternative to power morcellation because it does not create myometrial fragmentation. This is what prompted us to define our technique as “sectioning” rather than “morcellation,” which means “breaking the specimen into small pieces before removal.”
However, after the FDA statement in April 2014, we introduced a containment system to improve the safety of the technique, modifying our developed specimen retrieval bag used to remove the enlarged uterus with an endometrial cancer at laparoscopy. 21
Moreover, the longitudinal incision along the manipulator allows the surgeon to maintain correct anatomical relationships of the organ, a reconstruction of the whole uterus, and a precise histopathologic examination.
Lastly, this technique is more cost-effective than power morcellation and quicker than the vaginal approach. 14
We believe that this standardized technique may well be a viable alternative to power or vaginal morcellation in the presence of a bulky uterus, considering the low risk of injury and/or myometrial fragmentation along with the shorter operative time. However, further studies are advisable to fully assess the advantages of this procedure, and the use of specimen retrieval pouches should be investigated to further enhance safety and outcomes in a controlled setting.
Footnotes
Disclosure Statement
No competing financial interests exist.