
Abstract
Abstract
Background:
A prospective randomized comparison of three-dimensional (3D) versus two-dimensional (2D) imaging during elective laparoscopic cholecystectomy (LC), both performed separately by an advanced laparoscopic surgeon and by a surgeon experienced in open surgical procedures but a novice at laparoscopic procedures, was designed to address the issue of whether 3D systems offer real operative time advantages to this laparoscopic procedure.
Patients and Methods:
Eighty patients were randomized the day of surgery by random computer-generated allocation list to receive either a 3D or 2D high-definition imaging system LC by two surgeons with differing experience. After the insertion of the access ports the surgical procedure was divided in two component tasks. Operative times of the two component tasks and the entire procedure were recorded.
Results:
The execution times for the two component tasks and the entire procedure were not significantly different between the 2D and 3D groups for the experienced laparoscopic surgeon. However, the execution times for the two component tasks and the entire procedure were significantly faster during 3D compared with 2D for the novice surgeon. Both surgeons experienced better depth perception with the 3D system and subjectively reported less strain using 3D rather than 2D vision.
Conclusions:
3D imaging seems not to influence the performance time of LC by an experienced laparoscopic surgeon. Less experienced laparoscopic surgeons could benefit from shorter performance time with 3D imaging due to no need to adapt to 2D vision. Further comparative studies are necessary to verify on great numbers of cases whether 3D can reduce intraoperative complications such as biliary lesions.
Introduction
Background
D
Open questions
Some experimental studies have reported that the 3D systems improve task efficiency in laparoscopic manipulations, whereas other reports found no significant difference between 3D and 2D systems. The synthetic phantom task setup used and the involvement of medical students during experimental studies simulate only partial surgical procedures, do not reflect the complexity of clinical conditions, and could lead to unreal results. Moreover, clinical comparative studies are lacking in the literature. Laparoscopic cholecystectomy (LC) is the preferred and more accepted method of cholecystectomy for gallbladder disease. The real advantages of 3D versus 2D imaging for LC are still not known. 2 Only one prospective randomized study, conducted by Hanna et al., 3 exists in the literature and shows no statistically meaningful differences between the two imaging systems.
Aims
To address the issue of whether 3D offers real operative time advantages to the laparoscopic surgical procedure, we have designed a prospective randomized comparison of 3D versus 2D imaging during elective LC, performed both by an advanced laparoscopic surgeon (S1) and by a surgeon experienced in open surgical procedures but a novice in laparoscopy (S2).
Patients and Methods
Study design and patients
The patients recruited for the study had uncomplicated symptomatic gallstone disease and were admitted to the University Hospital of Messina, Messina, Italy, to undergo elective LC. Patients with a history of cholecystitis or previous surgery were excluded from the study. A senior laparoscopic surgeon (S1), who had performed more than 500 LCs, and a surgeon experienced in open surgical procedures but a novice in laparoscopy (S2), who had performed fewer than 40 LCs, carried out all surgical procedures. They were assisted by two other consultant surgeons, who acted as the camera operators. The novice surgeon had performed during the last 2 years around 200 laparoscopic surgical procedures as the assistant or camera operator and around 40 laparoscopic procedures as the first operator (around 20 LCs). As part of laparoscopic training he had acquired laparoscopic skills using also a training box, and he was assisted during his first 10 laparoscopic procedures by a senior laparoscopic surgeon. Both surgeons underwent examination for visual acuity, color vision, stereopsis, and accommodation. All surgical procedures were performed over a period of 24 months. Before starting the study both surgeons performed five LCs each with the 3D system for learning and training. Patients were randomized the day of surgery by a random computer-generated allocation list. Eighty operations were performed with either a 3D HD display or a 2D HD imaging system (40 by each method and each surgeon). All patients were informed and gave their full consent.
Procedures
All LCs were performed using a standard four-trocar technique. After the insertion of the access ports the surgical procedure was divided into two component tasks. The first task was dissection of the cystic duct and artery in Calot's triangle (time from grasping the fundus of the gallbladder to clipping and dividing the cystic artery and duct), and the second task was separation of the gallbladder from the liver bed (time from dividing the clipped cystic duct to complete separation of the gallbladder from its bed). The time of complete procedure has been considered since the insertion of the first trocar to removal of the gallbladder and drainage positioning under the liver bed. Operative times of the two component tasks and of the entire procedure have been recordedfor both surgeons by a fifth observer surgeon who did not take part in any of the procedures included in the study. Laparoscopic procedures were graded by the observer surgeon as “easy” or “difficult” depending on the presence or absence of adhesions, stone impacted in the neck, and anatomical abnormalities. Intra- and postoperative complications were recorded but were not the end points of the study due to the size of the sample. The 2D imaging system consisted of the Olympus 2D/HD system (Olympus Corp., Tokyo, Japan), and the 3D imaging system was the KARL STORZ 3D camera system (Karl Storz, Tuttlingen, Germany). The3D system was equipped with a 30° direction of view, 10-mm-diameter laparoscope and a 3D camera control unit for the transmission of 3D signals to a 32-inch HD 3D monitor. The cost of this system has been around 80,000 euros.
Results
Patients' characteristics
The two surgical groups were similar for age (mean, 50 years [range, 28–70 years] in the 2D group versus 56 years [range, 32–71 years] in the 3D group), gender (9 men and 26 women versus 7 men and 28 women, respectively), and body mass index (mean, 30 kg/m2 [range, 25–32 kg/m2] versus 31 kg/m2 [range, 24–34 kg/m2], respectively). Surgical procedures reported as “difficult” due to adhesions or stone impacted in the neck by the observer surgeon were similar in the 2D and 3D groups and for the experienced and novice surgeons (10 and 12 for the experienced surgeon versus 9 and 10 for the novice surgeon in 2D and 3D surgery, respectively).
Operative parameters
The execution times for the two component tasks and the entire procedure were not significantly different between the 2D and 3D groups for the experienced surgeon (Table 1). Conversely, the execution times for the two component tasks and the entire procedure were significantly faster during 3D compared with 2D surgery for the novice surgeon (Table 2 and Figs. 1 and 2). The performance time (single tasks and entire procedure) was faster for S1 compared with S2 during 2D and 3D vision. No conversion to an open procedure was recorded for either groups or surgeons. The gallbladder was injured twice in 2D and once in 3D by S1, versus five times in 2D and twice in 3D by S2. No postoperative complications were reported in either group for both surgeons. Surgeons experienced better depth perception with the 3D system and subjectively reported less strain using the 3D vision system rather than the 2D system, particularly during longer procedures and by S2.
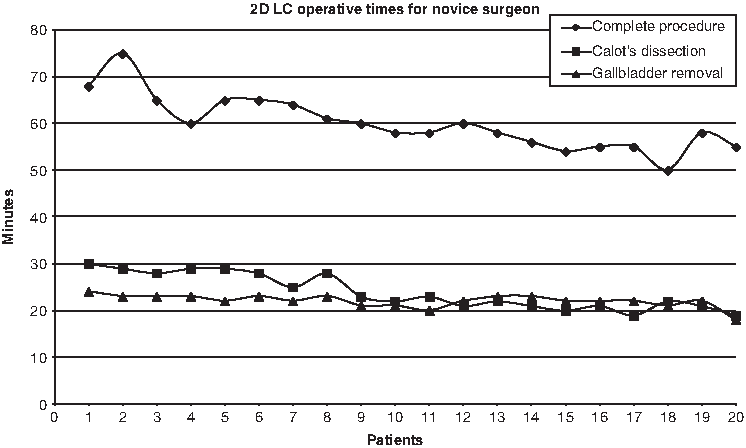
Execution times of two-dimensional (2D) laparoscopic cholecystectomy (LC) by a novice surgeon (S2).
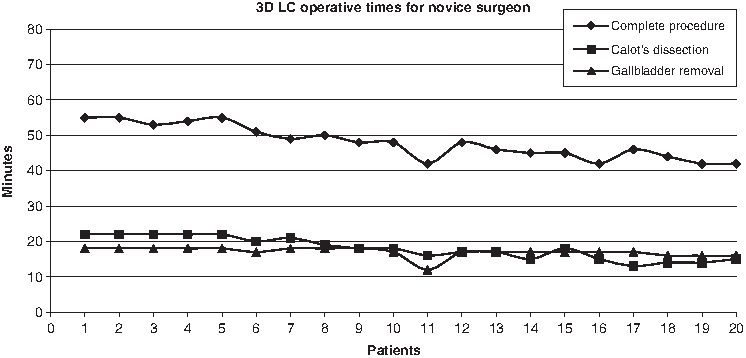
Execution times of three-dimensional (3D) laparoscopic cholecystectomy (LC) by a novice surgeon (S2).
2D, two-dimensional; 3D, three-dimensional.
2D, two-dimensional; 3D, three-dimensional.
Discussion
Definition of novice and senior surgeon in laparoscopy
Novice surgeons are described in the literature as surgeons with less than 3 years of experience in LC or as surgeons who have performed fewer than 30–50 LCs as the first operator. 4 It is widely accepted that to become proficient in LC, the surgeon must perform 30 LCs as the first operator. 5 This study showed that no difference in performing LCs exists between using the 3D imaging rather than the 2D HD imaging system when the surgeon is highly experienced in laparoscopic procedures. Conversely, when the surgeon is a novice in laparoscopy, the 3D imaging system has a great impact on performance time compared with 2D vision.
Interpretation of results
In our opinion these results can be explained by the nature of the surgical task and by the high degree of laparoscopic experience of one surgeon. In our opinion if the surgeon is experienced in 2D laparoscopy, he or she does not require the help of a stereoscopic view to perform LC. One of the largest challenges for surgeons moving from open to laparoscopic surgery is the hand–eye coordination within a 3D scene observed on a 2D display. 6 In fact, laparoscopic surgeons require extended experience to overcome the lack of depth perception. The more experience a surgeon gets, the more he or she gets used to the 2D vision. It has been shown that 3D perception on a 2D display improves with education. Through experience a laparoscopic surgeon learns that a structure or condition is related to another structure or condition with high probability and can use shadow or movement parallax as the depth cue instead of stereovision. 7
Technology evaluation
With the use of the 3D imaging system, the limitations of 2D HD laparoscopy can be overcome. The most recent 3D imaging systems are dual-lens systems where two separate lenses are present within a single laparoscope along with two cameras. Each camera captures its respective images, which are then displayed and synchronized on a video monitor. The quality of image, superior today to that of 15 years ago, seems to be useful in performing difficult tasks as suturing or knotting, but it has not been shown to influence the performance time, as shown in our study, when tasks are easier and the surgeon is experienced. In our case series, both surgeons did not experience any of the discomforts, such as headache, dizziness, and strain, that occurred at the beginning of clinical use of 3D imaging system in laparoscopy that were correlated with the first single-lens technology. Despite the benefits claimed, 3D systems have not yet been widely used, probably due to the high expense of these systems and the lack of studies reporting a real superiority of 3D over 2D vision in laparoscopic procedure performance.
Literature analysis
Most of the studies that showed superiority of a 3D over a 2D imaging system have been conducted using an experimental surgical model. Van Bergen et al. 8 reported no significant differences in execution times between 3D and 2D vision in a model with five standardized tasks. In a experimental study performed by Storz et al., 9 it was demonstrated how both difficult and easy tasks were completed with greater precision and shorter performance time when medical students were working under 3D vision rather than 2D vision. Conversely, in the same setting, advanced laparoscopic surgeons, although faster and more accurate than medical students, did not show any significant difference in performance time and precision for an easy task under both 3D and 2D vision but were faster during difficult tasks as suturing and stitching. 9 As previously mentioned, only one prospective randomized study, by Hanna et al., 3 exists in the literature, and it showed no statistically meaningful differences between the two imaging systems. It is noteworthy that surgeons involved in this study were all novice surgeons (fewer than 20 LCs performed), but probably the use of a first-generation single-lens laparoscope, which does not project a true stereoscopic vision to the operator, may have influenced their results. A more recent study by Bilgen et al. 10 reported significant reduction in the performance time of LC performed under 3D vision. Surgeons participating in their study were all experienced in laparoscopy, but the 2D group was artificially created by computer and in our opinion negatively influenced their results.
Conclusions
On the basis of our results, 3D imaging seems not to influence the performance time of LC by an advanced laparoscopic surgeon. Less experienced laparoscopic surgeons could benefit from shorter performance time with 3D imaging due to no need to adapt to 2D vision. 11 Further comparative studies are necessary to verify on great numbers whether 3D can reduce costs and, even performed in a similar operative time, decrease intraoperative complications such as biliary lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.