
Abstract
Abstract
Purpose:
This study presents a technical report of a standardized approach to the perinephric area in a series of pediatric patients, demonstrating that whatever renal or suprarenal surgery is planned, this can be approached and accomplished laparoscopically with an identical or very similar port triangulation, thus facilitating the learning curve within the same surgical team.
Patients and Methods:
All patients undergoing renal and adrenal gland surgery with a minimally invasive approach in the period from October 2008 to November 2013 were retrospectively reviewed and included in the study. Technical details and clinical outcomes are described.
Results:
In total, 68 patients matched the inclusion criteria and were therefore retrospectively examined. No major intraoperative complication occurred. Two patients developed recurrent pelvic–ureteric junction obstruction and were managed with double J stent positioning and laparoscopic dismembered pyeloplasty, respectively. Two patients presenting with adrenal mass experienced a moderate bleeding that could be treated conservatively.
Conclusions:
Thanks to the reproducibility of the procedure and on the grounds of the presented experience, we support the proposal that the transperitoneal laparoscopic approach to the kidney and the adrenal gland could represent a relatively easy and safe way to quickly achieve confidence and skill in the management of related diseases.
Introduction
T
Pediatric kidney surgery indications include nephrectomy or partial nephrectomy, stone removal, kidney biopsy, and pyeloplasty. On the other hand, adrenalectomy is usually the procedure performed whenever an adrenal mass such as a benign cyst, a pheochromocytoma, an adenoma, or, most importantly, a neuroblastic tumor is present.4,8
This study provides specific technical issues aiming to demonstrate that whatever renal or suprarenal surgery is planned, this can be approached and accomplished laparoscopically with an identical or very similar port triangulation, thus facilitating the learning curve within the same surgical team. The aim of this study is to present a technical report of a standardized approach to the perinephric area in a series of pediatric patients.
Patients and Methods
All patients undergoing renal and adrenal gland surgery with a minimally invasive approach in the period from October 2008 to November 2013 were retrospectively reviewed and included in the study.
Surgery is always preceded by a disease-specific imaging work-up (ultrasound scan, computed tomography scan, and/or magnetic resonance imaging). The surgical indication is established by a disease management team during a multidisciplinary discussion meeting on a weekly basis.
Bowel preparation is not requested. Intraoperative antibiotic prophylaxis is usually administered 30 minutes before surgery and during the first 24 hours postoperatively.
After induction of general anesthesia, the patient is positioned in a 60°–90° lateral decubitus, elevated on a soft roll, as in open surgery (Fig. 1).

Preoperative patient preparation and positioning for left pelvic–ureteric junction obstruction: the patient is positioned in a 60° right decubitus, elevated on a soft roll, with the left flank exposed.
Transperitoneal laparoscopy is performed by initially placing a 10–12-mm umbilical camera port, followed by two 3–5-mm working ports placed in the epigastrium and in the ipsilateral lower quadrant, respectively. Operating on the right side may generally require a fourth 3-mm port to retract the liver (Fig. 2).
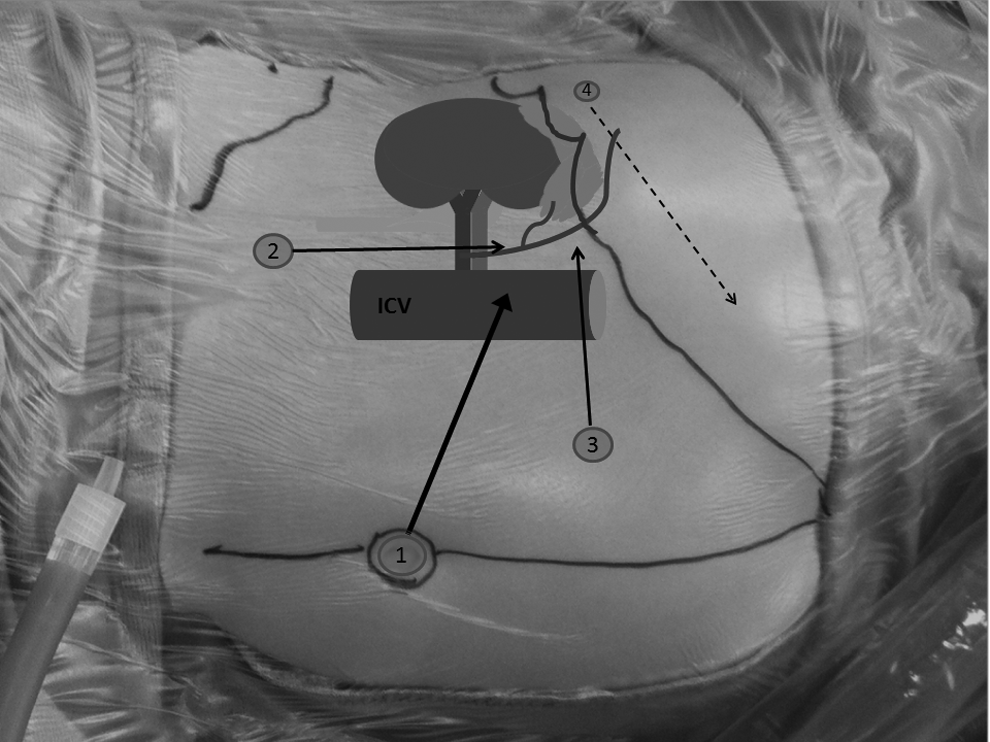
The geometry of laparoscopy, right side. A 10–12-mm umbilical camera port is initially placed (1), followed by two 3–5-mm working ports placed in the epigastrium and in the ipsilateral lower quadrant (2 and 3). The left hand (2) is ideally directed parallel to the inferior cava vein (ICV) to safely manage the adrenal gland venous drainage. Depending on liver anatomy, an additional fourth intercostal or epigastric port is helpful in liver retraction (4).
Access to the renal pelvis and ureter (nephrectomy, partial nephrectomy, stone removal, or pyeloplasty) is achieved by gentle displacement of the colon, with minimal opening of the parietocolic peritoneum. The perinephric area is approached anteriorly to safely manage the vessels and the pelvis. The ureter is identified and dissected free toward the pelvis. If a dismembered pyeloplasty according to the Anderson–Hynes technique is planned, the renal pelvis is mobilized to obtain enough freedom for a tension-free anastomosis. Stay sutures are inserted through the abdominal wall and placed across the ureter and the renal pelvis to expose the pelvic–ureteric junction (PUJ). The pelvis is divided 1 cm proximally to the PUJ. The ureter is spatulated below the stenosis by introducing scissors parallel to the ureter through an ancillary intercostal port (Fig. 3).
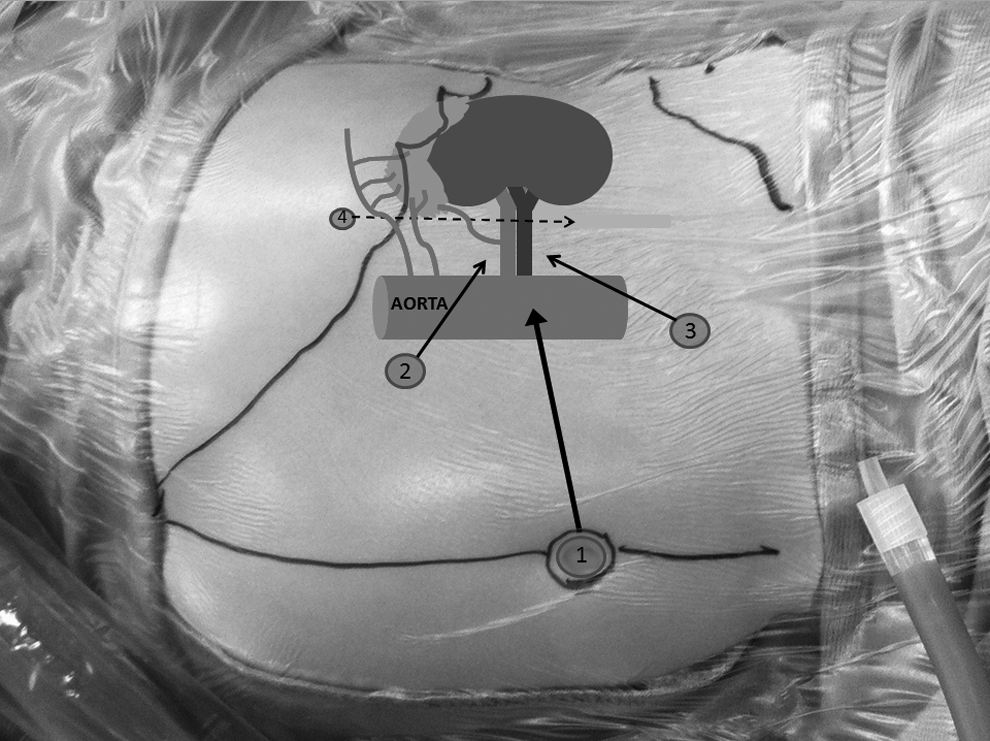
The geometry of laparoscopy, left side. A 10–12-mm umbilical camera port is initially placed (1), followed by two 3–5-mm working ports placed in the epigastrium and in the ipsilateral lower quadrant (2 and 3). The angle between the instruments for suturing should be ideally between 45° and 90°. An additional fourth intercostal port may be necessary if ureter spatulation is necessary during pyeloplasty (4).
The posterior wall is anastomosed first using a 5/0 monofilament absorbable interrupted suture. Once the posterior wall is completed, a double J stent is placed percutaneously. The anterior wall is then anastomosed in a similar fashion. The double J stent is generally removed 4–6 weeks after surgery. Alternatively, a percutaneous transnephrostomic drainage may be inserted and removed during the third or fourth postoperative day.
When a crossing vessel is found being causative of PUJ obstruction, the technique consists in transposing the vessel in a higher position, well away from the PUJ. The vessel is therefore pexed by suturing the pelvis on either side of the vessel with three nonabsorbable interrupted sutures without tension (the so-called Hellstrom vascular hitch).
In case a nephrectomy or a partial nephrectomy is planned, renal vessels are approached anteriorly once the pelvis and ureter are divided distally or proximally, according to the presence or absence of vesicoureteric reflux, respectively.
A large stone entrapped in the pelvis, unresponsive to medical treatment, can be approached by opening the renal pelvis with scissors, extraction of the stone, and suturing the pelvis with a 5/0 monofilament absorbable interrupted suture. A ureteral stent is usually placed via cystoscopy preoperatively.
Access to the adrenal gland follows the same principles and steps described above (Fig. 2). The adrenal mass is gently dissected from the aorta or the vena cava depending on the side of the operation. Right-sided adrenal masses may contact the duodenum, which should be carefully identified and dissected. Vessels heading to or coming from the adrenal gland may originate directly from the aorta or vena cava, from the renal vessels, or from the diaphragm. Therefore, great care is taken in the dissection of the mass from these structures. The mass usually contacts the psoas muscle posteriorly, without being infiltrated in most cases. Loose adhesions are encountered laterally (toward the abdominal wall) and inferiorly (toward the kidney) and are separated with ease. According to clinical suspicion and/or histological nature, normal adrenal tissue that is often found surrounding the mass can be removed with the mass itself or left in situ, to prevent adrenal gland insufficiency. Once completely freed, the mass is usually placed in a plastic bag and extracted through the enlarged umbilical access.
Results
In the period between October 2008 and November 2013, in total, 68 patients (42 males and 26 females; median age, 3 years; age range, 50 days–20 years) matched the inclusion criteria and were therefore retrospectively examined (Fig. 4).

Disease-specific distribution of patients.
Forty-three of the 68 patients (27 males and 16 females; median age, 3.5 years; range, 7 months–20 years) underwent renal surgery with a transperitoneal laparoscopic approach. Thirty-six of these 43 patients presented with a persistent/progressive degree of PUJ obstruction. Procedures performed were dismembered pyeloplasty in 21 patients, vascular hitch in 8 patients, and adhesiolysis in the remaining 7 patients. Five of these 43 patients underwent laparoscopic lithotomy due to pelvic urolithiasis, whereas the remaining 2 patients presented with renal duplication and underwent laparoscopic heminephrectomy. Median operative time was 105 minutes (range, 40–220 minutes). A ureteral double J stent was positioned in 25 of the 28 patients whose pelvis was opened. The remaining 3 patients received an external ureteral stent as the double J stent could not be passed in the bladder.
No major intraoperative complication occurred. Intraoperative estimated blood losses were calculated to be within the acceptable threshold. No patient required red blood cell transfusion. Median hospital stay was 3 days (range, 1–14 days). One month postoperatively, 2 patients previously treated with adhesiolysis developed recurrent PUJ obstruction. This was demonstrated by ultrasonography scan and magnetic resonance imaging. A cystoscopy with double J stent positioning was performed in both patients and then removed after 2 months, with complete resolution documented by ultrasonography scan in the first patient. Unfortunately, the second patient showed persistent PUJ dilatation and therefore underwent successful laparoscopic dismembered pyeloplasty 6 months postoperatively.
Twenty-five of the 68 patients (15 males and 10 females; median age, 1.4 years; range, 50 days–13 years) underwent transperitoneal laparoscopic adrenal gland surgery. All patients presented with a localized adrenal mass clinically and radiologically suggestive for neuroblastoma, which was histologically confirmed postoperatively. Image-defined risk factors were not detected in any patient (stage L1). 9 Median size (considering the largest mass diameter) of the adrenal masses was 30 mm (range, 12–83 mm). Median operative time was 105 minutes (range, 60–240 minutes). All patients underwent successful complete tumor excision without major intraoperative complications. Two patients experienced a moderate bleeding that could be treated conservatively using an appropriate vessel sealing device without the need for red blood cell transfusion. Median hospital stay was 3 days (range, 2–10 days).
Discussion
As widely demonstrated, both retroperitoneoscopy and transperitoneal laparoscopy have been successfully considered and applied to manage renal and adrenal gland surgical indications. As no scientific evidence of one technique being better than the other one has been achieved, every surgeon dealing with such diseases should rely on his or her personal preference and experience. However, it seems that a certain propensity is recently growing among general and pediatric surgeons toward the transperitoneal laparoscopic approach.5,8,10–14 We did experience both the mentioned approaches and finally embraced the latter choice. It must be noted that the retroperitoneal approach is limited by a small working space and decreased maneuverability.
Perhaps the most important advantage of the transperitoneal laparoscopic approach is the presence of familiar anatomic landmarks, which are crucial in orienting the surgeon. Because tactile feedback is compromised during laparoscopy, the surgeon is more dependent on visual cues, such as the position of adjacent organs, to maintain orientation. Thus, the transperitoneal approach represents a more intuitive extension for most surgeons, and this favorably impacts the learning curve. In addition, the transperitoneal approach allows for simple entrapment of large specimens, easier morcellation if desired, and the crucial ability to examine and treat possible concomitant intraperitoneal and/or retroperitoneal disease.
Almost all the procedures involving the upper urinary tract and the adrenal gland can be managed with the transperitoneal approach, whereas certain scenarios such as anterior renal disease can be extremely challenging, even for skilled retroperitoneal surgeons. As such, a surgeon familiar with the retroperitoneal approach also must learn the transperitoneal approach, but the converse of this is not necessarily true. Surgeons learning the retroperitoneal approach have the added burden of learning a new anatomical layout and adjusting to a small operative field. 10
Moreover, we do support the concept that the same patient preparation and patient positioning standards should be applied to both renal and suprarenal surgeries. In fact, although different procedures may be carried out, exposure of the kidney and the adrenal gland should follow the same surgical steps.
As a consequence, surgeons involved in the training program are thus facilitated in the learning process of understanding the “triangulation” concept in laparoscopy. When starting with advanced laparoscopic surgery, such as laparoscopic pyeloplasty or adrenalectomy, one has to be aware of the geometry of laparoscopy: the angle between the instruments for suturing should be ideally between 45° and 90°, whereas vessel dissection or ureter spatulation should be accomplished through an operative access oriented parallel to these structures (Figs. 2 and 3). The angle between the instruments and the working plane should be less than 60°, and the working height of the surgeon should permit an angle of 90° of his or her elbow. Working at an inadequate height or using a suboptimal trocar arrangement can be considered a factor that could lead to a potentially serious intraoperative incident. 15 Suturing or dissecting tissues in an less-than-optimal trocar arrangement may lead in the best case to placement of additional ports and in the worst case to massive bleeding, bowel or liver injury, or ineffective suturing causing anastomotic leakage or stricture. Moreover, an optimal patient positioning is of utmost importance. The mere 60°–90° lateral decubitus of the patient during the procedure optimizes and shortens renal and adrenal gland exposure, thus often avoiding a potentially highly demanding dissection for the surgeon.
The success rates of dismembered pyeloplasty have been reported to exceed 95% in long-term studies. 16 Although this technique has become a well-accepted gold standard treatment modality for PUJ obstruction, the question of whether postoperative urinary diversion after pyeloplasty is beneficial has been debated for decades, particularly in infants and smaller children who have narrow ureters. Some surgeons prefer to just simply leave a perinephric drain without urinary diversion. On the other hand, there are many ways to divert urine, and different types of drainage methods have been described in the literature, including nephrostomy tube drainage, internal ureteral stents such as the double J stent, external stent, or a combination of these modalities.
The advantages of a double J stent compared with a nephrostomy tube include a shorter hospital stay and a lower morbidity rate. 17 Furthermore, a double J stent prevents adhesion to the suture site, helps to maintain an appropriate diameter and alignment of the ureter, and limits ureter kinking. On the other hand, disadvantages of such a stent include that it can cause stent-related complications such as urinary tract infection and provoke ureter obstruction by irritating the mucosa of the ureter or the renal pelvis. Moreover, a double J stent requires an additional general anesthesia for removal.17–19
The overall rate of urological complications in both stented and nonstented cases is similar, ranging from 12% and 15%. In both groups, recurrent PUJ obstruction occurs in 2%–4% of cases. 19 Therefore, the choice of postoperative urine drainage should be made by surgeon's preference rather than by the perceived complication rate or the duration of hospital stay.
In our series, the majority of patients whose pelvis was opened were regularly internally stented for 4–6 weeks postoperatively, and then the stent was removed with no case of recurrent PUJ obstruction. Three patients younger than 1 year of age had an external ureteral stent because the double J stent could not be passed through the vescicoureteric junction into the bladder.
Despite the high success rates in the management of PUJ obstruction, some patients may show persistency or develop recurrence of the obstruction. Various strategies have been adopted in these situation: observation, ureteral stent placement, percutaneous nephrostomy, endopyelotomy, repeated pyeloplasty (by laparoscopy or open surgery), or nephrectomy. 20 All these options provided good results in skilled hands. Although symptomatic or worsening patients should be generally approached surgically with repeated pyeloplasty or nephrectomy, conservative management may be an increasingly viable solution, especially in patients with minimal symptoms and stable renal function. 20
Two patients from our series experienced asymptomatic PUJ re-obstruction and were consequently treated by stent positioning and laparoscopic pyeloplasty, depending upon resolution or persistency of pelvic dilation following stent positioning, respectively. Although more challenging, reiterative laparoscopic access to the renal pelvis in the latter patient did not imply technical differences and, most importantly, resulted in a safe and successful procedure. These 2 patients, along with 5 other patients, had been previously treated with pelvic adhesiolysis because of PUJ obstruction due to severe reactive inflammatory tissue surrounding the pelvis. This scenario was supposed on preoperative urologic magnetic resonance imaging, and consequently a surgical procedure to free the pelvis from such tissue was planned. There are many etiologies for fibrosis and inflammation causing PUJ obstruction, such as infections, previous instrumentation including endopyelotomy, and previous abdominal surgery. 20 None of these 7 patients had previous surgery and/or endopyelotomy, and therefore the main suspicion was directed toward unrecognized recurrent urinary infections.
Due to the high failure rate of this technique (28.5%), we no longer consider this procedure applicable to patients with severe PUJ obstruction.
Bleeding is a common complication when dealing with adrenal masses. Precise evaluation and exclusion of image-defined risk factors (i.e., vessel encasement) may prevent massive bleeding, which could be difficult to manage laparoscopically. 21 Minor or low-pressure bleeding (due to multiple small vessels entering the adrenal mass) can be safely managed with simple gauze pressure, intracorporeal stitching, and/or the use of vessel sealing devices. Our preference is directed toward use of the ValleyLab (Boulder, CO) LigaSure™ vessel sealing system, which has the worldwide recognized advantage of an optimal hemostasis with minimal thermal injuries to adjacent structures.
In conclusion, whatever renal or adrenal surgery is planned, whatever approach and procedure is chosen by the surgeon, we do believe that the preparation of the patient, his or her correct positioning in order to obtain the best anatomical exposition of the operative field, an optimal predetermined trocar arrangement, and following always the same surgical steps for similar procedures represent the key factors when starting with advanced minimally invasive surgery. Thanks to the procedure's reproducibility and on the grounds of the presented experience, we support the proposal that the transperitoneal laparoscopic approach to the kidney and the adrenal gland could represent a relatively easy and safe way to quickly achieve confidence and skill in the management of related diseases.
Footnotes
Disclosure Statement
No competing financial interests exist.