
Abstract
Abstract
Introduction:
This retrospective study aims to compare open colectomy and hand-assisted laparoscopic surgery (HALS) in the management of acute obstructive right-sided colon cancer and to analyze and evaluate the feasibility and safety of HALS.
Patients and Methods:
Ten consecutive patients who underwent hand-assisted laparoscopic right hemicolectomy due to acute obstructive right-sided colon cancer were retrospectively well matched with 25 patients scheduled for a conventional laparotomy during the same time. Demographic, intraoperative, and postoperative data were assessed.
Results:
The HALS group had the advantage in the length of incision (5.8±0.7 cm) over the conventional group (16±2.3 cm) (P<.05), and the mean blood loss during the operations was significantly less in the HALS group (30±15.2 mL) than in the laparotomy group (90±29.4 mL) (P<.05). Moreover, the time of postoperative ambulation was earlier (2.5±0.8 days versus 3.2±0.9 days) (P<.05). Seven cases underwent intestinal decompression for severe intestinal dilatation and had a satisfactory result. The hand-assisted device can fairly meet the demands of a minimally invasive operation and can protect the abdominal incision and avoid infection. There was no intergroup difference in complication rate, although the conventional group had a higher rate.
Conclusions:
In this study, compared with conventional laparotomy for acute obstructive right-sided colon neoplasm, HALS is associated with less blood loss, shorter incision, and earlier ambulation. Emergency laparoscopic-assisted right hemicolectomy can be safely performed in patients with obstructing right-sided colonic carcinoma. If practiced more, it might be advocated as a bridge between the conventional open approach and traditional laparoscopic surgery.
Introduction
A
Laparoscopic colorectal surgery has been widely carried out in recent years because of the advantages of less trauma and quicker recovery, and since its first report in 1993 it has rapidly become a popular procedure worldwide. 5 Despite this, adoption has been relatively difficult for the cases of emergency patients with obstructive right colon carcinoma because the abdominal space in these patients was occupied by the proximal expansion of the intestine and the risk of injuring the distended bowel during manipulation. 6 So, the open approach is often the first choice for these subjects.
Recently, our department carried out hand-assisted laparoscopic surgery (HALS) in treating acute obstructive right colon cancer and achieved good results. HALS, another popular minimally invasive surgical technique that has been adopted by colorectal surgeons, uses a hand-access assembled device that maintains a peritoneal gas pressure while allowing the surgeon to introduce the nondominant hand into the abdominal cavity. With the use of laparoscopic visualization and instrumentation, the surgeon's hand can assist with retraction, dissection, and hemostasis. Additionally, the hand-access device incision serves as the site of specimen extraction.7,8 As a hybrid procedure of open colectomy and laparoscopic colorectal surgery, it retains many of the benefits of the standard laparoscopic approach while restoring tactile sensation to the surgeon, shortening the learning curve, and reducing the institutional costs.7,9–13 In a multicenter, prospective, randomized trial comparing HALS versus laparoscopic colorectal surgery, researchers found that HALS resulted in significantly shorter operative times while maintaining similar clinical outcomes as straight laparoscopic techniques for patients undergoing left-sided colectomy and total abdominal colectomy. 14 Moreover, we also found that the expanded small intestine can be decompressed through the small incision, which will improve the improved laparoscopic exposure space, reduce the rate of conversion to open surgery and the risk of surgery injury, and enhance the role of surgical safety.
With the above background, we set out to conduct a retrospective study that aims to compare the efficacies and short-term clinical outcomes between HALS and conventional laparotomy for acute obstructive right-sided colon cancer and to explore the feasibility and safety of HALS.
Patients and Methods
Case information
A retrospective analysis of medical record was performed for patients who presented for acute obstructive right-sided colon cancer between January and June 2013 to our department at the First Affiliated Hospital of Nanchang University in China. All the patients had undergone a preoperative computed tomography scan through which an occupying and obstructing lesion on the right colon from the cecum to the proximal transverse colon was diagnosed.
The following patients were excluded from the study: (1) patients for whom a right hemicolectomy was performed but colon cancer was not confirmed by pathology after surgery; (2) patients who had peritonitis, pericolic abscess or sepsis, etc.; (3) patients with metastatic disease on preoperative work-up; and (4) patients with synchronous tumors or polyps that necessitated multivisceral resection and those for whom only segmental resection was performed.
Finally, of the 35 patients involved in this study, 28 patients had been diagnosed with colon cancer by routine colonoscopy and pathology, and the other 7 patients had very clear computed tomography diagnosis signs that were confirmed by pathology after surgery. Ten patients underwent a hand-assisted laparoscopic right hemicolectomy (HALS group), and 25 patients underwent a conventional open right hemicolectomy (open group). There were 20 males and 15 females. The mean duration of obstruction was 3 days (range, 1–10 days). The open group was selected so as to be case-matched with the HALS group in the aspects of age, sex, medical history, tumor size, and tumor-node-metastasis (TNM) stage during the same period (Table 1). All patients underwent a curative R0 resection in our department by one experienced member of the surgeon team. The inclusion criterion for who underwent HALS was by each surgeon on a case-by-case basis. Each surgeon chose the procedure on the basis of individual preference, and each surgeon can practice both techniques. In comparison of open colectomy and HALS, there was no significant difference between the two techniques that would have made the surgeon chooses the one technique over the other.
Data are mean±standard deviation (range) values or number of patients, as indicated.
BMI, body mass index; HALS, hand-assisted laparoscopic surgery; NS, not significant; OC, open colectomy; TNM, tumor-node-metastasis.
Surgical methods
All patients underwent preoperative gastrointestinal decompression by using a nasogastric tube and prophylactic use of antibiotics, and the balance disorders of water and electrolytes were corrected as far as possible.
For conventional open surgery, the patient is placed in the supine position, and a median or right transrectus incision is performed. If the intestinal obstruction is serious, intraoperative intestine decompression should be performed first. Then the right colon is dissociated and resected according to the principle of free radical resection of the tumor, and interrupted suture mesocolon hiatus is performed after the ileotransversostomy.
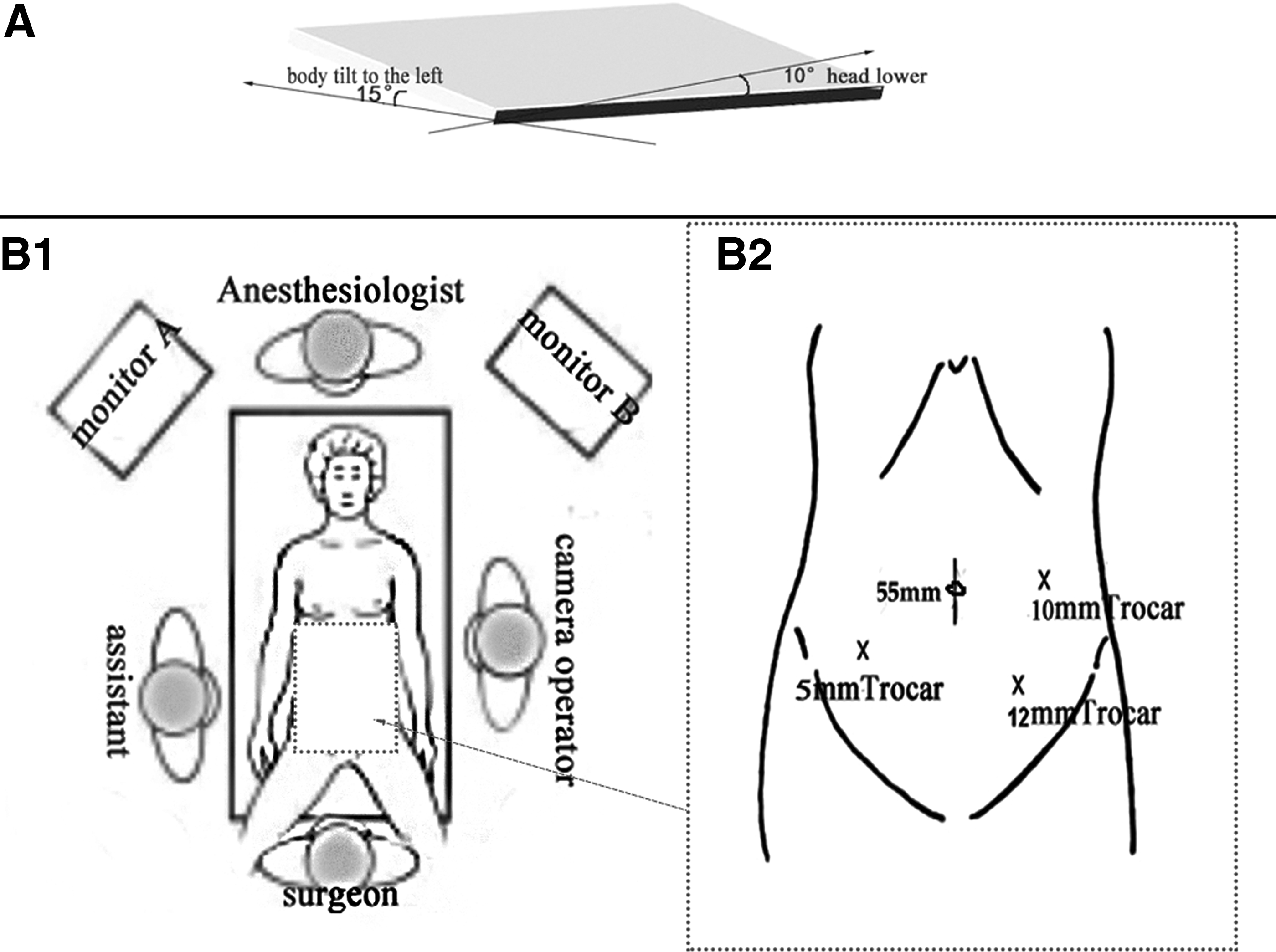
For HALS, first, pneumoperitoneum is established before exploration. The patient is in the supine position, with the legs horizontally split and fixed, the head lowered by 10°, and the body tilted 15° to the left by rotating the operating table. Pneumoperitoneum pressure is maintained at 12–15 mm Hg.
The position of the surgeon is shown in Figure 1. An approximately 5.5-cm-long longitudinal incision is made with the umbilicus as the center, and the minimally invasive access system (ENDOPATH DEXTRUS®; Ethicon Endo-Surgery, LLC, a Johnson & Johnson Company, Cincinnati, OH) is inserted as the hand-assisted device. A 12-mm trocar for the 30° telescope (Karl Storz, Tuttlingen, Germany) is inserted at the midclavicular line at the level of the left lower quadrant, and after pneumoperitoneum is established, other trocars are inserted under direct vision: the 10–12-mm trocar at slightly lateral to the left midclavicular line is inserted as the main operating hole (mainly for the use of an ultrasound knife and a hemostatic clamp), and the lower abdominal 5-mm trocar is the right lower quadrant near the midclavicular line. This port may be used as the vice operating hole to facilitate mobilization of the intestine. The surgeon and camera operator may switch trocar ports during the procedure to provide better visualization and operating angles. Under special circumstances (such as patient size), an alternative port placement should be adopted (Fig. 1).
When the exposure space is seriously occupied by the obstruction, enteral decompression would be performed first that carefully puts the obstructive intestine out through the small ENDOPATH DEXTRUS incision. A small incision is made in the lower segment, the contents of the distal and proximal intestine are aspirated with the help of the aspirator, and then continuous double suture intestinal decompression is cut (Fig. 2). After decompression, the left hand is inserted through the ENDOPATH DEXTRUS incision, the establishment of pneumoperitoneum is finished, and the pelvic and abdominal cavities and tumor diseases are explored, to understand the relation of the tumor and adjacent organs.
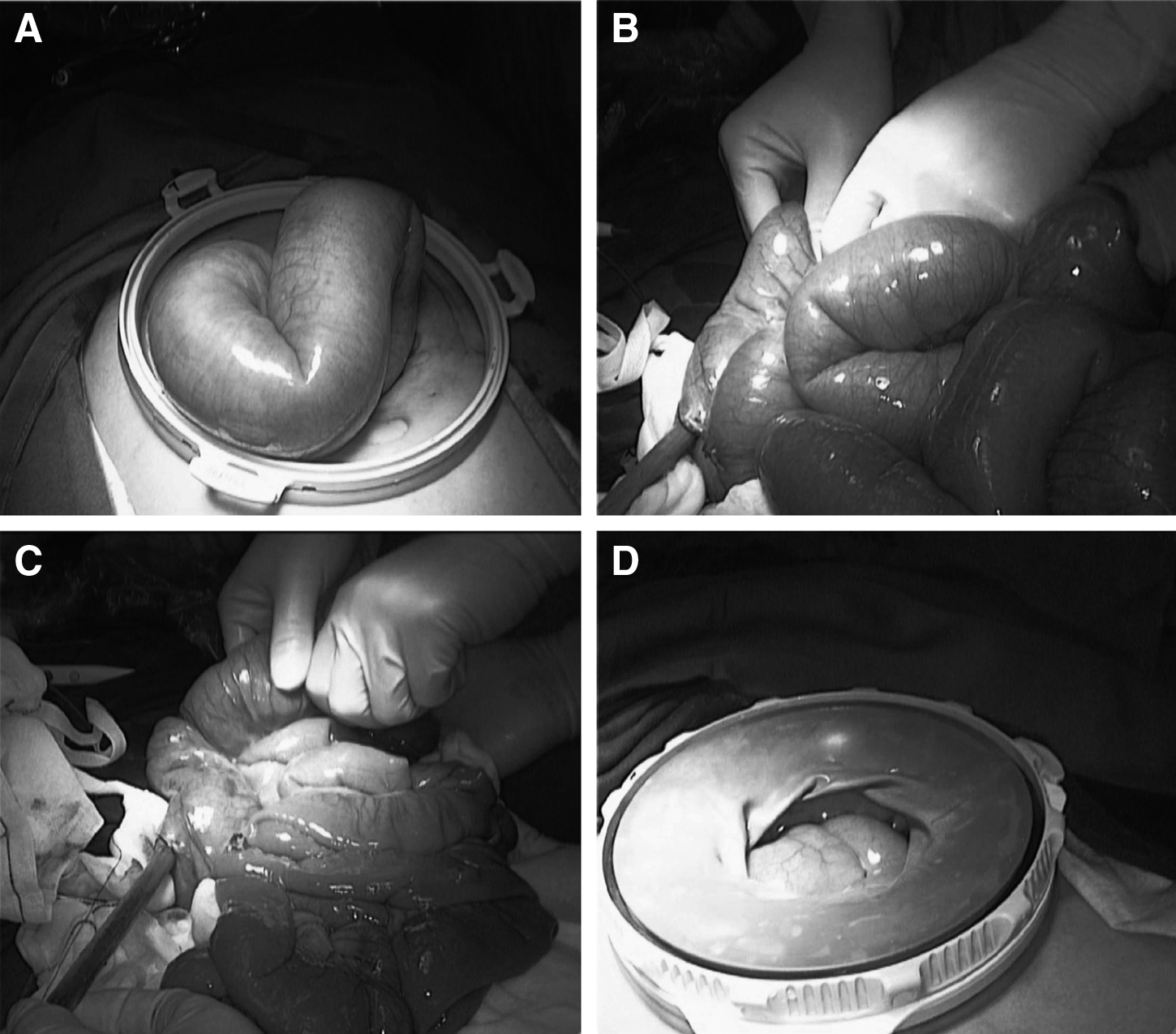
The process of intestinal decompression.
Second, for the treatment of major blood vessels, mobilization of the right colon is done by a medial approach. The posterior peritoneum is isolated along the right edge of the superior mesenteric vein from bottom to top. Lymph and adipose tissues are eliminated. The ileocolic artery and vein are dissected at the root of vessels. The surgeon lifts the right mesocolon and opens Toldt's fascia, exposing the horizontal part of the duodenum to the inferior border of the pancreas or uncinate process of the pancreas. The dissection is carried toward the hepatic flexure and up to Henle's gastrocolic truck and skeletonized. The right colic vein and right gastroepiploic vein are isolated and dissected. Along the right edge of the middle colic artery the right branch is separated and dissected.
Third, the omentum majus and right gastric colon ligament are dissociated and dissected, as well as the hepatic flexure of the colon, and the side peritoneum is separated. Then the free right colon resection lesions are extracted from the incision.
Finally, to perform a side-to-side extracorporeal stapled anastomosis, the proximal ileum and distal colon are then rotated the required number of degrees in order to align the antimesenteric borders. A portion of the antimesenteric border staple line is obliquely excised from each limb so as to create an opening large enough for insertion of the forks of the cutting linear stapler instrument. The linear stapler is then introduced and closed. Once it is ensured that the posterior aspect of the bowel has been examined to be certain that no mesentery is included in the closed stapler, the stapler is discharged, and the anastomosis is created. The enterotomy is closed with a stapler. Any bleeding points after the removal of the stapling instrument are controlled with interrupted sutures. The mesenteric defect is closed, and the bowel is returned to the peritoneal cavity.
During postoperative care, the patients use patient-controlled interscalene analgesia to control pain for 1 or 2 days, according the condition of patients. The orogastric or nasogastric tube provides decompression until bowel activity returns. Intravenous fluids are administered, and vital signs and urine output are monitored every 4 hours. Antibiotic therapy is discontinued after a few days or so unless the patient has a continuing infection. The bladder catheter is removed on postoperative Day 1 or 2. Clear liquids are started on postoperative Day 2 or 3 if there is no distention or indications of complications, and this is advanced as tolerated. Early ambulation is permitted.
To determine the efficacy of HALS, the two groups were compared with respect to several perioperative factors, such as length of incision, total operative time, operative blood loss, number of resected lymph nodes, number of enteral decompressions, rate of conversion to open surgery, the recovery time of bowel function, the time of early ambulation after operation, postoperative hospital stay, and the incidence of postoperative complications, including frequency of postoperative respiratory complications, frequency of anastomotic leakage, frequency of incision infection, frequency of urinary tract infection, and retention of urine. Postoperative respiratory complications were defined as those involving major respiratory insufficiency, such as a need for re-intubation or severe pneumonia.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 software (SPSS Inc., Chicago, IL). The two-sample/group t test was used to analyze intergroup differences. Measurement data are expressed as mean±standard deviation values. Quantitative data were analyzed by chi-squared test, Fisher's exact test, or Mann–Whitney U test as appropriate. P<.05 was considered statistically significant.
Results
From January 2011 to June 2013, there were 35 cases of patients with acute obstruction of the right colon cancer included in this study. Ten patients (six males and four females) made up the HALS group, with an average age of 64.5±9.7 years (range, 42–89 years). There was 1 case of previous appendectomy. Obstruction duration averaged 3±1.2 days (range, 1–6 days). There were 2 cases of postoperative TNM stage II and 8 cases of stage III. Twenty-five patients (14 males and 11 females) made up the laparotomy group, with an average age of 62.3±10.2 years (range, 39–92 years). There were 2 cases of previous appendectomy, 1 case of tubal ligation, and 1 case of hysterectomy. Obstruction duration averaged 3±1.8 days (range, 1–10 days). There were 9 cases of postoperative TNM stage II and 16 cases of stage III.
No significant differences were found between the HALS and conventional groups in terms of sex, age, body mass index, operation history, the duration of obstruction, tumor staging (TNM), tumor diameter, number of lymph nodes dissected, recovery time of intestinal peristalsis, and hospital stay (Tables 1 and 2). The HALS group has the advantage in the length of incision (5.8±0.7 cm) over the conventional group (16±2.3 cm) (P<.05), and the mean blood loss during the operations was significantly less in the HALS group (30±15.2 mL) than in the laparotomy group (90±29.4 mL) (P<.05). Moreover, the time of postoperative ambulation was earlier (2.5±0.8 days versus 3.2±0.9 days) (P<.05). But, the duration of operation time was longer in the HALS group than in the open group (186.5±18.4 minutes versus 142±20.8 minutes) (P<.05). There were no conversions to the open procedure in the HALS group. Seven cases underwent intestinal decompression because of severe intestinal dilatation and had a satisfactory result. The average decompression time in our study was 21 minutes (Table 2). The minimally invasive access system (ENDOPATH DEXTRUS) hand-assisted device can fairly meet the demands of a minimally invasive operation and can protect the abdominal incision and avoid infection. During HALS we select the pneumoperitoneum pressure to be between 12 and 15 mm Hg; there were no complications of pneumoperitoneum such as subcutaneous emphysema and pneumothorax in the HALS group. Although the number of complications was higher in the laparotomy group, the difference in complication rate was not significant (Table 3).
Data are mean±standard deviation (range) values or number of patients, as indicated.
HALS, hand-assisted laparoscopic surgery; NS, not significant; OC, open colectomy.
Data are number of cases.
HALS, hand-assisted laparoscopic surgery; NS, not significant; OC, open colectomy.
Discussion
At present, laparoscopy for operations has been increasingly practiced worldwide; the technical level has been extended to all areas of surgery. Laparoscopic colectomy for colon cancer has been reported in the surgical literature since 1991. 15 The laparoscopic operation not only has obvious advantages in the treatment of colorectal cancer, but also is a relatively early operation to carry out in this field.5,16,17 But, along with the technical development, clinicians have encountered some new problems in daily work, including the longer operative time, risk of port-site cancer recurrences, the procedural complexity, the loss of tactile feedback, the lack of optimal retracting devices, and the need for more expensive instrumentation. Laparoscopic resections can be technically demanding and difficult to learn and teach.10,18–21 In addition, it is difficult for some obstructive colorectal cancer patients to accept the laparoscopic minimally invasive therapy as abdominal bowel dilatation affects the exposure space of peritoneal insufflation. 6
In recent years, many scholars carried out some exploration on laparoscopic treatment of obstructive colon cancer. Colorectal stents have been used successfully as preoperative “bridges to surgery” for patients with obstructing left-sided colorectal carcinoma. 22 Stipa et al. 23 performed endoscopic colonic decompression first with self-expanding metallic stents for 31 patients with obstructing colorectal cancer; the laparoscopic minimally invasive operation was performed about a week after the intestinal obstruction disappeared, which achieved a satisfactory effect. Chung et al. 24 and Fernández-Esparrach et al. 25 also reported the successful results in laparoscopic treatment with an endoscopic stent relieving left colonic obstruction. But, the best position of the bracket is placed in the rectum and sigmoid colon, which can result in only dealing with part of the left obstructive colon tumors. Published articles on the use of colorectal stents in treating obstructing right-sided colonic carcinoma, however, are scarce.26,27 So far, the laparoscopic treatment of obstructive right-sided colon has not been well solved. The key to successfully performing laparoscopic minimally invasive treatment for obstructive colorectal cancer patients is to provide enough space for the laparoscopic operation. Patients with seriously dilated bowel loops and a distended abdomen are generally not suitable for laparoscopic surgery because of poor visibility and a high risk of bowel injury. Patients with bulky and fixed obstructing tumors should also be excluded from laparoscopic surgery.6,22 Careful patient selection with preoperative computed tomography scanning is needed to avoid invalid operations and complications.
In 1995, Kusminsky et al. 28 completed the first HALS splenectomy, and they also later used HALS in colorectal surgery. The application of HALS in colorectal disease makes more sense because a mini-incision is needed at the end of the procedure to perform the anastomosis, and because it includes procedures in several parts of the abdominal cavity, HALS resection was associated with a significantly higher lymph node harvest than laparoscopic resection. The development of total laparoscopic surgery was delayed for these features.19,29 Its advantages include better control of hemorrhagic accidents, thereby reducing the conversion rate, metastatic lesions, small lesions, and lymph nodes, which are hard to find by laparoscopic exploration, and the local staging of tumors can be detected. Insertion of the hand restores the tactile feeling and the sensation of depth and facilitates the exposure, traction, and retraction maneuvers during the procedure. Additionally, the hand-access device incision serves as the specimen extraction site.7,9,12,15,16,30 Moreover, through clinical practice we found HALS may be an interesting alternative to conventional laparoscopic or open surgery in therapy of acute obstructive right-sided colon cancer as it incorporates elements of both the laparoscopic and the traditional open techniques. It simplifies the performance of difficult procedures for experienced surgeons and can initiate less experienced surgeons in advanced laparoscopic surgery.
Because the initial stage of operation of HALS is carried on with about a 5–6-cm small incision with the umbilicus as the center, the operation was done by placing the minimally invasive access system (ENDOPATH DEXTRUS) as the hand-assisted device.7,29,31 In those patients with severe acute obstructive symptoms, we can carry out intestine decompression through the small umbilicus incision, which will provide greater pneumoperitoneum space for surgery and the possibility for laparoscopic operation, and greatly improve the safety of the operation. In our study, intraoperative intestinal decompression was performed in 7 cases of obstructive colorectal cancer patients in the HALS group and achieved a satisfactory result. The other 3 patients did not due to the short time of obstruction and because the ileocecal valve prevents reflux of colonic contents into the small intestine; thus the small intestine expansion is not serious.
The incision infection rate of emergency intestinal surgery is higher than that of general elective surgery; surgery performed along with intestinal decompression will increase the incidence of wound infection. The minimally invasive access system (ENDOPATH DEXTRUS) hand-assisted device not only means a satisfactory sealed space of pneumoperitoneum, but also it can achieve a good protection role in that the incision is shielded from contamination by the colonic contents because the device should be also biologically resistant. 15 In our HALS group, no incision infection occurred in patients who underwent intestinal decompression, whereas in the open group, 3 cases of incision infection occurred. In addition, due to the obstruction of the right colon, cancer patients have mostly advanced disease, so the lymph node dissection plays a clinically important role in the prognosis and management of the acute obstructive right-sided colon cancer patient. We compared the HALS and laparotomy groups; there was no significant difference in the number of lymph nodes dissected. The initial studies comparing open colectomy with laparoscopic colectomy for colon cancer had the same result. 32 However, Osarogiagbon et al. 15 found that significantly more lymph nodes were present in the specimens obtained by hand-assisted laparoscopic colectomy than by open colectomy. This difference might be explained in part by the improved visualization of the operating field obtained on the monitors attached to the laparoscopic equipment. But the explanation for this discrepancy in lymph node harvest between the different groups is difficult to ascertain as, in the whole, more long-term follow-up and investigation of tumor outcome need to be done.
Although we may change the position of the trocar according to the tumor location for better visualization and mobilization, the surgical procedure discussed in this article is the standard practice in all 10 cases. According to our experience, we think patients who shared the following features were suitable for the hand-assisted laparoscopic approach: small stenotic tumors, short duration of symptoms, and mildly dilated small bowel loops (especially for the obese and elderly patients). Those cases with a grossly distended abdomen and dilated bowel loops are generally good candidates given that intestinal decompression can be well performed. Some cases with undefined bulky and fixed obstructing tumors could choose HALS first and be converted to laparotomy if patients are in special circumstances.
Although we tried to minimize bias by including consecutive patients who had had HALS, by using the case-control strategy, and because all patients are from the same department and were managed by the same team of surgeons, this study still had limitations, including the retrospective design and the possibility that the two cohorts of patients might not be directly comparable. We did not collect data on postoperative adjuvant therapy or long-term survival because we were primarily interested in the feasibility and effectiveness of the surgical technique in surgical therapy of acute obstructive right-sided colon cancer. As a possible criticism of our study, one might ask whether HALS really maintains the benefits of minimally invasive surgery with the relatively small number of subjects in each study arm. Although emergency hand-assisted laparoscopic right hemicolectomy has been shown to be feasible in our small cohort of patients, we think that prospective randomized trials and large numbers of patients are needed to further define the potential benefits of HALS over conventional open surgery for this disease, and we are also moving in this direction. But, on the whole, as patients with such disease presenting as an emergency are relatively few, as this article is concerned, we preliminarily explored the possibility, feasibility, and safety of HALS in emergency right hemicolectomy for obstructive right-sided colon carcinoma and tried to prove that HALS can become a practical and attractive alternative in laparoscopic colorectal surgery.
In summary, we think intraoperative intestinal decompression via HALS can improve the abdominal cavity, create the opportunity of minimally invasive treatment of obstructive colorectal cancer, improve the security of the operation, and provide a new direction for the development of laparoscopic operations. With less operating time, reduction in size of surgical wounds, less blood loss, potentially lower postoperative complication rate, equivalent oncologic resection, and equivalent duration of hospital admission, hand-assisted laparoscopic colectomy might be more cost-effective than open colectomy. Appropriately designed prospective clinical trials are needed to investigate this possibility.
Footnotes
Disclosure Statement
No competing financial interests exist.