
Abstract
Abstract
Introduction:
Laparoscopic distal pancreatectomy (LDP) is replacing open surgery as the technique of choice for benign and premalignant lesions of the left pancreas. In most laparoscopic series, the supine decubitus or semilateral position is preferred. A posterior approach with the patient in full right lateral decubitus (PA-FRLD) has been proposed as an alternative.
Patients and Methods:
From July 2012 to November 2014 we performed 14 LDPs. PA-FRLD was chosen in 8 patients; in 6 patients splenectomy was also performed.
Results:
Definitive diagnoses were 3 cases of pancreatic ductal adenocarcinoma, 2 cases of nonfunctioning neuroendocrine tumors, 1 case of bulky serous cystic neoplasm, 1 case of inflammatory chronic pancreatitis, and 1 case of pancreatic trauma (duct disruption). No conversions were required. No postoperative pancreatic fistula was detected. No patient required transfusion. Two patients had Clavien II and IIIb postoperative complications. In both cases in which preservation of the splenic vessels was attempted, it was successfully achieved.
Conclusions:
The PA-FRLD position is a valid alternative to the supine or semilateral position for LDP. This approach is especially beneficial for resection of complex and bulky lesions of the tail of the pancreas and those in close contact with retroperitoneal organs and can also facilitate spleen-preserving LDP.
Introduction
C
In most series of laparoscopic DP (LDP), with or without preservation of the spleen, the anterior approach is preferred with the patient in the supine position1,7,11,12 because it allows good control of the main vessels in case of injury and rapid conversion to laparotomy if required. Some authors have also proposed the use of this approach but with the patient in the semilateral position13–15 in order to facilitate the mobilization of the spleen.
In 2007, Honore et al. 16 described the posterior approach with the patient in full right lateral decubitus (PA-FRLD), on the grounds that it simplified the procedure, achieved better preservation of the anterior abdominal cavity, the great omentum, and the splenic vessels, and left the short gastric vessels untouched. The main advantage of PA-FRLD is that it facilitates the mobilization and exposure of the posterior face of the tail of the pancreas, which is the deepest retroperitoneal part of the gland and tends to be difficult to access via the anterior approach. Since then, other authors have reported their experience with this position for selected cases. 17
We describe our experience with the use of the PA-FRLD in LDP and discuss the technique's advantages and disadvantages.
Patients and Methods
From July 2012 to November 2014 we performed DP in 19 patients. The most common diagnosis was pancreatic ductal adenocarcinoma, recorded in 12 patients. Fourteen patients (73%) were operated on laparoscopically. Open surgery was preferred in the other 5 patients: 4 with pancreatic carcinoma infiltrating the splenoportomesenteric venous system and requiring vascular resection and reconstruction (2 with previous neoadjuvant chemoradiotherapy) and 1 who presented with sepsis due to a pancreatic fistula caused by main duct syndrome disruption after retroperitoneal necrosectomy for necrotizing pancreatitis 6 months previously. Of the 14 patients operated on via laparoscopy, the PA-FRLD was used in 8. In 6 patients we chose an anterior approach: in 4 in order to perform a radical resection using the RAMPS technique, 12 in 1 because a combination of DP and enucleation of a tumor in the head of the pancreas was planned due to multiple metastasis of a kidney clear cell carcinoma, and in 1 who had a multifocal intraductal mucinous neoplasm because the pancreas was divided at the union between the head and the neck to the left of the portal vein.
The surgical technique used for the PA-FRLD was the one previously described by Honore et al. 16 with the patient in full right lateral decubitus and the trocars inserted in the left subcostal area (Fig. 1). In all the procedures, four trocars (two 12 mm and two 5 mm) and a 30° telescope were used. The dissection began by descending the splenic flexure of the colon and then opening the lesser sac via the greater gastric curvature to expose the tail of the pancreas. If an en bloc splenopancreatectomy was planned, all the short gastric vessels were ligated and divided as far as the angle of His, and the left crus of the diaphragm was identified. The splenic artery was dissected at the upper edge of the pancreas and the splenic vein at the lower edge. The decision to divide these vessels depended on whether the spleen was to be preserved. In both cases in which the splenic vessels were preserved, they were also dissected at the level of the splenic hilum. Once the distal pancreas was surrounded, it was divided. In cases in which splenectomy was indicated, the sectioning of the splenic ligaments was left until the end. The incision of assistance for the removal of the surgical specimen was a transverse suprapubic incision made without changing the patient's position (Fig. 1).

Positioning of the patient, placement of the trocars, and incision for removal of the specimen for the posterior approach with the patient in full right lateral decubitus in laparoscopic distal pancreatectomy.
Informed consent for this procedure was obtained from all patients.
Results
Table 1 displays the patients' characteristics and the results. The 3 patients who underwent LDP for pancreatic carcinoma were followed up for 30, 23, and 10 months, respectively, and are currently disease-free. In the 2 patients with nonfunctioning neuroendocrine tumors of the pancreatic tail, it was possible to preserve the spleen by preserving the splenic vessels, as had been planned. In the other 6 patients, a distal splenopancreatectomy was performed. No patient required blood transfusion during hospitalization. The 3 patients with benign disease presented particular technical difficulty: a bulky symptomatic serous cystic neoplasm, chronic pancreatitis with an inflammatory pseudotumoral mass, and emergency surgery to treat pancreatic trauma with disruption of the main pancreatic duct. Conversion to open or hand-assisted surgery was not required in any case. Two patients suffered complications.
ASA, American Society of Anesthesiologists; DSP, distal splenopancreatectomy; DSP-LN, en bloc distal splenopancreatectomy and left nephrectomy; F, female; M, male; NF-NET, nonfunctioning neuroendocrine tumor; PF, pancreatic fistula; SPDP, spleen-preserving distal pancreatectomy.
One patient required reoperation for postoperative intestinal obstruction due to adhesions resulting from multiple previous operations. This patient had been operated four times 40 years previously via a midline laparotomy for a subtotal gastrectomy due to a gastric ulcer and complications arising from leakage associated with that technique. During the approach for the LDP, only the adhesions impeding access to the surgical site (left upper quadrant of the abdomen) were released, and the incision for specimen removal was made by connecting three of the trocars inserted in the left subcostal region (Fig. 2). The patient underwent radical resection of the left pancreas with sectioning of the splenic artery and vein at their source (Fig. 3). Postoperatively, she presented a segmental intestinal ischemia due to a single long-standing adhesion requiring intestinal resection by laparotomy. Her postoperative stay was 47 days. The mean postoperative stay for the remaining 7 patients was 4.7 days.

The posterior approach with the patient in full right lateral decubitus in a patient with a previous laparotomy. The incision for removal of the specimen was performed by connecting three of the four trocars lined in the left subcostal site.
Discussion
Although the laparoscopic approach is well established and widely accepted for DP for the treatment of nonmalignant lesions, certain characteristics of the lesions and patients may complicate this approach. Among these characteristics are the size of the lesion and the invasion of adjacent retroperitoneal structures such as the kidney, adrenal gland, stomach, and spleen. The anterior laparoscopic approach is the most commonly used, with the patient in a supine or semilateral position at an angle of 30°, either with the legs spread and the surgeon located between them18,19 or with the legs closed.13,14
The steps that present the greatest technical difficulty during the anterior approach in LDP are the dissection of the splenic flexure of the colon and mesocolon, the division of the posterior splenic ligaments to complete the splenectomy after dividing the pancreas, the dissection of the splenic vein at the lower edge of the tail of the pancreas, and the dissection of the splenic vessels in the hilum if their preservation is planned. Warshaw's technique facilitates these steps as it avoids the dissection of the splenic vessels between the tail of the pancreas and the spleen. Indeed, in most published studies, conservative surgery of the spleen and its vessels is the least used technique.1,7,14 Although it has been claimed that the preservation or removal of the spleen does not affect the results, a recent comparative study showed that the risk of complications was lower and postoperative hospital stay was shorter if the splenic vessels were preserved. 20
Our experience with the laparoscopic approach in pancreatic surgery dates back to 2007. Until July 2012, we carried out 18 resections of the left pancreas, 15 of which were performed laparoscopically with an anterior approach. Of these, 1 patient had to be converted due to difficulties in the dissection of the mesocolon at the level of the pancreatic tail and the splenic flexure. We introduced the posterior approach in July 2012 in connection with an en bloc resection of the distal pancreas, left kidney, and spleen due to an infiltrating pancreatic carcinoma. The choice of this position proved to be essential for the successful completion of the laparoscopic procedure. Since then, we have regarded the posterior approach as the treatment of choice for resecting lesions of the pancreatic tail that do not require resection of the splenic vessels at their origin or radical lymphadenectomy.
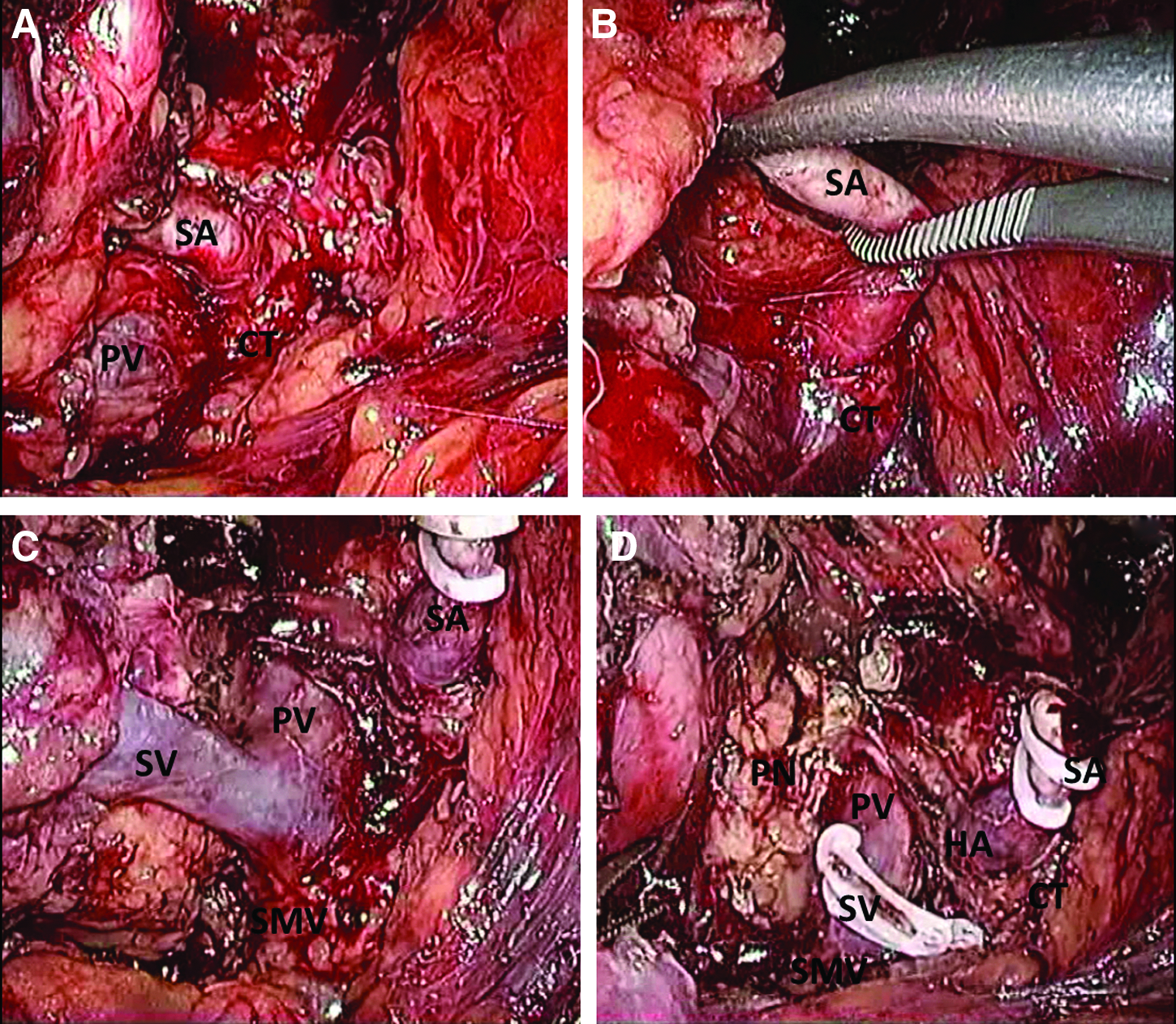
As the anterior approach was practically impossible in the patient who had undergone multiple previous laparotomies for gastrectomy (Fig. 2), we performed a radical splenopancreatectomy for the pancreatic body carcinoma but divided the splenic vessels at their origin (Fig. 3). In this case, the neck of the pancreas was sectioned after mobilization of the posterior surface of the entire left pancreas, and from this position the portal vein, inferior mesenteric vein, hepatic artery, and celiac trunk could be clearly identified (Fig. 3). In spite of this single experience and even though radical surgery is feasible via a posterior approach, we still prefer the anterior approach in cases of pancreatic ductal adenocarcinoma, for the following reasons: it allows us to perform the initial dissection of the neck of the pancreas and the splenic vessels at their origin at an early stage, it facilitates the lymphadenectomy of the common hepatic artery and celiac trunk using the RAMPS technique, and it allows the right-to-left dissection after sectioning the neck of the pancreas, leaving the mobilization of the spleen as the last step. 12
Using the posterior approach, conversion was not necessary in any of our patients, whereas among the 6 patients who underwent LDP in the same period with the anterior approach, 1 had to be converted due to bleeding in the splenic hilum in an attempt to preserve the splenic vessels. In the 2 patients in whom preservation of the spleen with its vessels was planned, this procedure was successfully completed. The only severe complication that occurred was not attributed to the approach but to the adhesions that the patient presented previously and that had not been fully released during LDP. Specifically, the posterior approach achieves better control than the anterior approach, thanks to the exposure of the splenic hilum, the posterior surface of the tail of the pancreas, and the splenic vessels coming through the inferior–posterior border of the pancreas, where the splenic vein is usually attached to the parenchyma. This facilitates the dissection of the splenic vessels and spares the parenchymal vessels. Although our sample size is small, our experience suggests that the posterior approach may favor the preservation of the splenic vessels in conservative surgery of the spleen. In a retrospective review of 359 patients undergoing LDP via a semilateral approach, Song et al. 14 reported that almost 50% of the patients underwent conservative surgery of the spleen and that in 84% of these cases the splenic vessels could be preserved.
There are two other situations in which the posterior approach facilitates the surgical resection. One is the dissection of left retroperitoneal structures (kidney, left adrenal gland) when they are attached to the pancreas; the other is the presence of bulky tumors that are difficult to handle inside the abdominal cavity (Fig. 4). In these cases, the initial approach and the division of the body of the pancreas make it possible to leave the tumor attached to the spleen and to postpone the division of the splenic ligaments until the end.
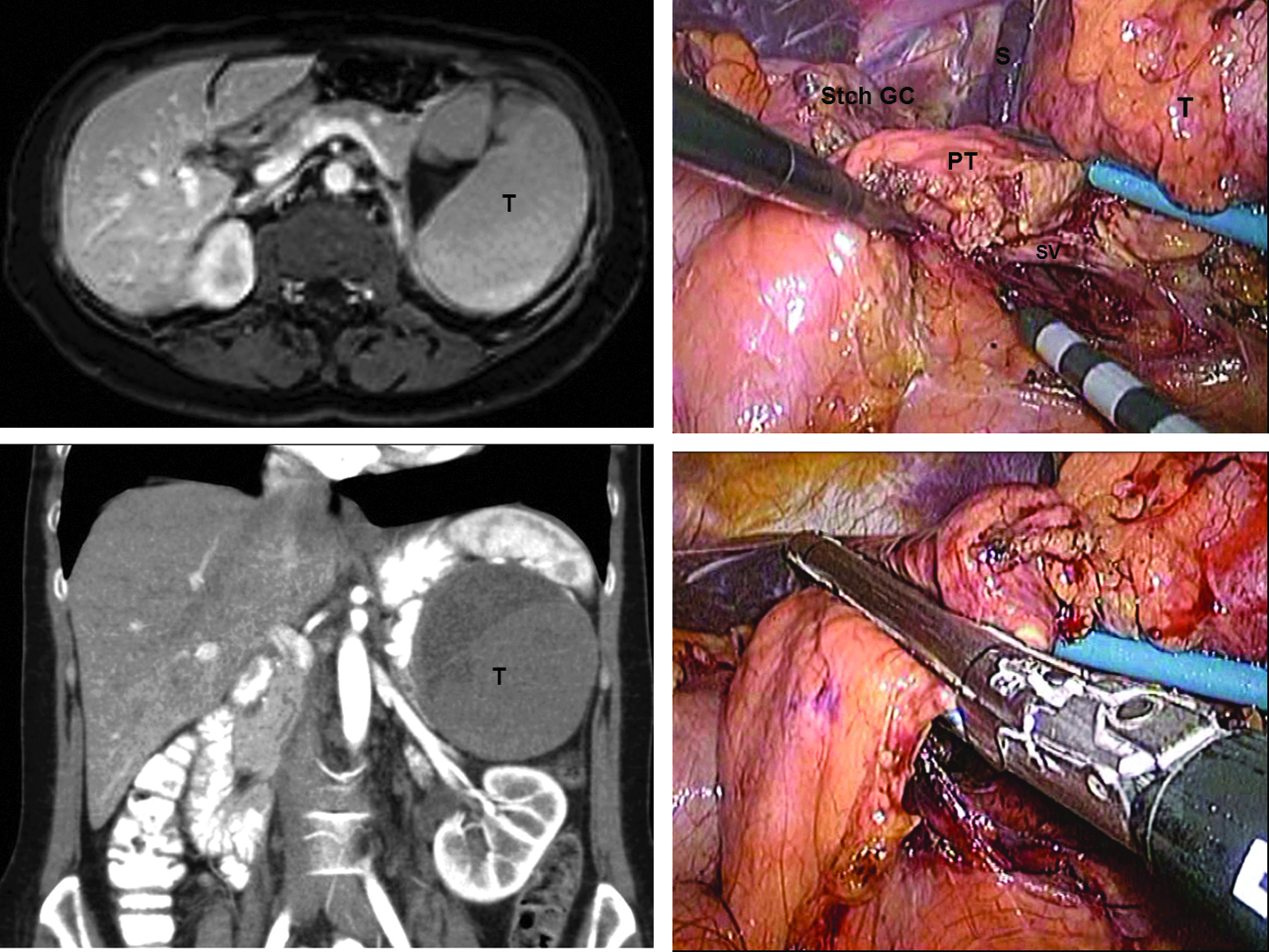
The posterior approach with the patient in full right lateral decubitus in laparoscopic distal pancreatectomy for a large tumor (T) in the tail of the pancreas. PT, pancreas tail; Stch GC, stomach greater curvature; SV, splenic vein.
In conclusion, PA-FRLD facilitates complete surgical resection in LDP for bulky and complex pancreatic lesions specifically involving the tail of the pancreas, especially those infiltrating adjacent retroperitoneal organs. It also facilitates the preservation of splenic vessels in spleen-preserving LDP when this is planned. It can therefore be considered an alternative to the anterior or semilateral approach and may even be the technique of choice in these selected cases.
Footnotes
Disclosure Statement
No competing financial interests exist.
I.P. contributed to this study in terms of conception, design, acquisition of data, drafting, analysis, revision, and final approval and wrote the manuscript. F.B. and L.G. contributed to this study in terms of analysis and interpretation of data, revision for intellectual content, and final approval.