
Abstract
Abstract
Purpose:
To report our technique and experiences in the laparoscopic diaphragmatic hemiplication (LDHP) in children with acquired diaphragmatic eventration after congenital heart surgery.
Subjects and Methods:
Between October 2007 to December 2013, 3498 children with congenital heart disease underwent cardiac surgery in our hospital, and 40 (1.14%) of them had unilateral diaphragmatic elevation on postoperative chest X-ray (mean elevation, 2.5 ± 0.26 intercostal spaces [ICS]) and were diagnosed as having diaphragmatic eventration due to diaphragmatic hemiparesis as a result of phrenic nerve injury. These 40 patients were followed up, and 22 of them recovered after conservative treatment; the other 18 needed surgical intervention. We conducted a retrospective study relating to surgical indications, surgical technique, complications, and outcomes.
Results:
There were 24 boys and 16 girls with a mean age of 10.0 ± 4.5 months old (range, 2 months–4 years). Twenty-two patients did not require surgical intervention. Eighteen patients underwent LDHP (12 cases left-sided and 6 cases right-sided); 2 of them had emergency LDHP with a history of ventilator dependency after cardiac surgery, and 16 of them had planned LDHP with a history of recurrent pneumonia and dyspnea. The operative time was 60 ± 7.9 minutes (range, 45–105 minutes), with minimal blood loss (3 ± 1.5 mL [range, 1–9 mL]), no intra- or postoperative complications, and postoperative hospital stay of 7 ± 1.3 days (range, 5–10 days). The diaphragmatic drop was 2.4 ± 0.2 (range, 2–4 ICS) without recurrence, and the follow-up time for all 40 patients was 14.8 ± 1.6 months (range, 11–36 months).
Conclusions:
Our study further shows that LDHP is feasible and effective in selected patients after congenital heart surgery. Our technique is convenient and provides excellent clinical and radiological results.
Introduction
P
In the past, diaphragmatic plication was performed by thoracotomy or laparotomy. Nowadays, the advancements in minimally invasive techniques have allowed us to perform diaphragmatic plication effectively and safely by laparoscopic or thoracoscopic techniques, with the well-known benefits such as minimal surgical trauma, short operative time, minimal blood loss, and less postoperative pain, which leads to fast recovery and shorter hospital stay. In this study we describe our technique and experiences with 18 pediatric patients with acquired diaphragmatic eventration operated on by laparoscopic diaphragmatic hemiplication (LDHP).
Subjects and Methods
Between October 2007 to December 2013, 3498 children with congenital heart disease underwent cardiac surgery in our hospital. Forty (1.14%) of them had unilateral diaphragmatic elevation (2.5 ± 0.26 intercostal spaces [ICS]) on postoperative chest X-ray (Fig. 1) compared with the preoperative chest X-ray (Fig. 2) and were diagnosed as having diaphragmatic eventration due to diaphragmatic hemiparesis as a result of phrenic nerve injury.

Chest X-ray showing the elevated diaphragm after cardiac surgery.

Chest X-ray showing symmetry of the two hemidiaphragms before cardiac surgery.
All the parents were fully educated about the acquired diaphragmatic eventration as one of the complications of open cardiac surgery. The management, follow-up, and indication for diaphragmatic plication were also explained. The patients' age, gender, location of the diaphragmatic eventration, underlying cardiac surgeries, the chest X-rays, and indication of surgery are given in Table 1.
ASD, atrial septal defect; AVSD, atrioventricular septal defect; CoA, coarctation of the aorta; DE, diaphragmatic eventration; ICS, intercostal spaces; LDHP, laparoscopic diaphragmatic hemiplication; LVOTO, left ventricular outflow tract obstruction; PAB, pulmonary artery banding; PDA, patent ductus arteriosus; TAPVR, total anomalous pulmonary venous return; TCPC, total cavopulmonary connection; VSD, ventral septal defect.
These 40 patients were followed up, and 22 of them recovered after conservative treatment; the other 18 needed surgical intervention. The surgical technique, operative data, and outcomes were analyzed. Before parents signed the consent form for surgery, they were informed about the laparoscopic procedure as well as the possibility of using additional trocars and conversion to the open technique. Advantages and disadvantages were reviewed.
Surgical procedures
After induction of general anesthesia, a nasogastric tube was inserted to decompress the stomach. The patient was placed in the 15° lateral position opposite to the operating side and positioned with the head raised to displace the intraabdominal organs downward. The operating surgeon was positioned between the legs of the patient.
The first trocar was placed at the umbilicus as the laparoscope port. After CO2 insufflation of the abdomen, two other trocars were placed, one in the right upper abdomen and the other one in the left middle abdomen, as working ports (Fig. 3). Usually we used three ports during the operation, but sometimes (in 6 cases) an additional 3-mm port was inserted in the upper left quadrant of the abdomen for additional assistance. The pneumoperitoneum pressure was 6–12 mm Hg, based on the patient's age. During the operation, assistants helped to drag the diaphragm to the abdominal cavity.

Position of the trocars: three 5-mm working ports and one optional 3-mm working port.
After an assessment of the abdomen, the viscous organs were mobilized, and the slack diaphragm was exposed and assessed. Then, 2-0 nonabsorbable suture was introduced into the peritoneal cavity through the anterior abdominal wall near the costal arch with the suture tail left outside the abdominal wall. Then, both sides of the weak areas and the top of the diaphragm were pleated little by little, like an accordion (Figs. 4–6). We performed intraperitoneal knot-tying with the grasping forceps holding the suture inside the abdominal cavity while an operating assistant pulling the end of the suture outside the abdominal cavity helped us to tie the knot intracorporeally with adequate tension on the suture and to drag the diaphragm down. When suturing it for plication, the intensity should be kept moderate until the lax diaphragm became taut and moved to a lower position. Usually we made two or three pleats, but sometimes (in 3 cases) we stitched an additional pleat when the tautness was unsatisfactory, which made the diaphragm straight and dropped to the normal level.
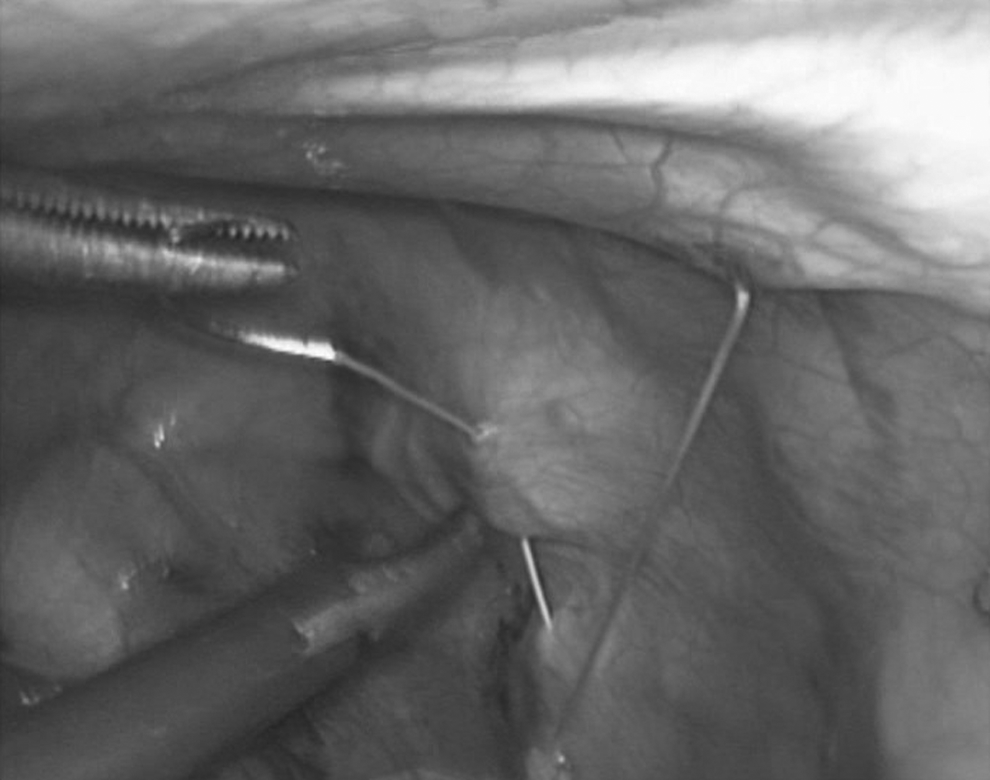
Alignment of the suture.

Winding of the suture, folding of the diaphragm, and the pleat (like the closing of an accordion).

Appearance of the diaphragm with two pleats.
The threads were cut, and the needles were removed through the anterior abdominal wall transparietally. The peritoneum at the umbilicus was closed with 2-0 polyglactin 910 (Vicryl®; Ethicon, Somerville, NJ) suture. The skin of the umbilicus and the 3-mm stab incisions were closed by skin glue without stitches (Fig. 7).

Appearance of the abdomen after wound closure.
By this LDHP procedure, the eventration of the diaphragm is evenly reduced, the chest cavity is enlarged, and the lung expands and functions better. No special instrument or procedure is used during the operation.
Statistical analysis
All the 40 patients were followed up after cardiac surgery at regular monthly intervals for 6 months and then at 3-month interval. Descriptive statistics are reported as mean ± standard deviation values and ranges. Statistical analysis was performed using SPSS version 18.0 software (SPSS, Inc., Chicago, IL). Student's t tests, the Mann–Whitney U test, and the chi-squared test were used to calculate the P value between the LDHP and non-LDHP groups. A P value of < .05 was considered statistically significant.
Results
The differences in mean age, male:female ratio, localization of the diaphragmatic eventration, underlying cardiac surgery with cardiopulmonary bypass or hypothermia, and follow-up were insignificant between the LDHP and non-LDHP groups. The diagnosis of diaphragmatic eventration was established after cardiac surgery on the postoperative chest X-ray (Fig. 1). The elevation in the LDHP group was 2.51 ± 0.24 ICS, and that in the non-LDHP group was 2.52 ± 0.23 ICS, which was not statistically significant between the two groups (P > .05).
Due to the inability to wean from mechanical ventilation and severe dyspnea, 2 patients underwent emergency LDHP (one on Day 7 and the other one on Day 8 after cardiac surgery), and these 2 patients had a longer hospital stay of 10 days post-LDHP but recovered well. The other 38 patients were under careful monitoring for the indications of surgery (Table 1).
The operative data and outcomes were analyzed, and the results are given in Table 2. Sixteen patients were extubated immediately after diaphragmatic plication, and 2 patients who had emergency diaphragmatic plication were extubated uneventfully after 48 hours. Mean diaphragmatic decrease was 2.4 ± 0.2 ICS (range, 2–4 ICS) after 1 week of LDHP (Fig. 8). The follow-up was 14.2 ± 1.7 months (range, 11–36 months), without recurrence of diaphragmatic eventration.

Chest X-ray after surgical management (laparoscopic diaphragmatic hemiplication) showing that the diaphragm of the operative side dropped to a normal level.
Data are mean ± standard deviation (range) values.
DE, diaphragmatic eventration; ICS, intercostal spaces; LDHP, laparoscopic diaphragmatic hemiplication.
Discussion
Diaphragmatic eventration after cardiac surgery in children is caused by diaphragmatic paralysis, which is due to phrenic nerve injury.2–4 Postoperative phrenic nerve lesion can occur as a consequence of contusion, dissection, stretch, and hyperthermic or hypothermic damage. 5 The main clinical signs after cardiac surgery are significant diaphragmatic elevation on chest X-ray and difficult extubation, and sometimes failure to wean off from the ventilator leads to emergency diaphragmatic plication (2 cases from the LDPH group). It is considered that a number of these children may recover from phrenic nerve injury by themselves within 1–3 months (17 cases from the non-LDHP group in this study). 1 Therefore, the first choice treatment is the clinical monitoring of these patients over a period of time (1–6 months), related to the surgical indications for diaphragmatic plication.6–8
These indications are also related to the pathophysiology of diaphragmatic eventration, which causes problems in four ways: (1) inability to ventilate the ipsilateral lung, (2) direct compression of the ipsilateral lung, (3) pneumonia due to chronic atelectasis, and (4) paradoxical motion of the diaphragm making ventilation of the contralateral lung inefficient. In the infant, the mediastinum is very mobile, and paradoxical movement of the affected diaphragm causes a shift of the heart and mediastinum toward the contralateral thorax. This limits effective ventilation of the opposite lung and also impedes venous return to the heart. If the patients are not affected by these conditions, there is no indication for operation even if they had permanent diaphragmatic elevation (in 5 cases from the non-LDHP group).
Laparoscopic diaphragmatic plication was first described by Hüttl et al. 9 ; in their report, 3 adult patients developed eventration of the diaphragm after cardiac surgery, and laparoscopic plication resulted in significant improvements in pulmonary function tests and shortness of breath. The laparoscopic plication used for children with eventration of the diaphragm has been successfully reported in several cases.6,10,11 After accumulating some experiences in laparoscopic diaphragmatic plication to treat congenital eventration of diaphragm and laparoscopic diaphragmatic hernia repair, we started performing the plication to treat acquired diaphragmatic eventration after congenital heart defects repair in those children indicated for diaphragmatic plication using the pleating technique. Eighteen patients in this study had surgical indications, and we successfully applied the LDHP procedure. There were no intra- or postoperative complication, no re-occurrence or re-elevation, and no pneumothorax, and clinically these patients were better without related chest infections.
The advantages of laparoscopic and thoracoscopic surgery over the open technique are as follows: (1) less pain from the incisions after surgery; (2) shorter hospital stay; (3) shorter recovery time; (4) faster return to normal activity; and (5) better cosmetic healing. The advantages of laparoscopic over thoracoscopic are as follows10,12: (1) The thoracic cavity has adhesions in children after cardiac surgery, transthoracic plication may be difficult, and transabdominal plication avoids the adhesion after cardiac surgery. (2) There is lesser risk of pneumothorax. (3) It provides a better intraoperative view with greater freedom for manipulating the instruments. (4) It avoids the complication of decreased cerebral O2 saturation during thoracoscopic procedures. 13 (5) In the thoracoscopic procedure, the collapsed lung on the operating side and compression of the mediastinum could lead to hypoxia and hemodynamic changes. 14
In order to reduce the diaphragmatic tension, the use of a knotter 9 and injection of gas into the thoracic cavity 15 had been reported. We just performed intraperitoneal knot-tying with the grasping forceps holding the suture inside the abdominal cavity while an operating assistant pulling the end of the suture outside the abdominal cavity helped us to tie the knot intracorporeally with adequate tension on the suture and to drag the diaphragm down. When suturing for plication, the intensity should be kept moderate until the lax diaphragm becomes taut and moves to a lower position.
In LDHP, usually we used three ports, but in 6 cases (4 on the left and 2 on the right side) the diaphragm was tenser, and one additional 3-mm trocar was inserted in the left upper abdomen to provide additional assistance for manipulating the diaphragm and ease of suturing. The use of an endostapler device by Lao et al. 11 for laparoscopic transperitoneal repair of pediatric diaphragm eventration has also been reported; it is a very interesting method, but we simply used 2-0 nonabsorbable suture instead.
Our study described a bigger sample for acquired diaphragmatic eventration after cardiac surgery, and the management is based on the indications for diaphragmatic plication. We further showed that LDHP is feasible and effective in patients who had operative indications, and it has some more advantages compared with the open or thoracoscopic techniques. Our technique is convenient and simple with excellent clinical and radiological results.
Footnotes
Disclosure Statement
No competing financial interests exist.