
Abstract
Abstract
The incidence of rectal cancer in India is on the rise, and unlike in the West, predominantly younger individuals are affected. Surgery for rectal cancer has evolved over the years with the ultimate goals of sphincter preservation and better quality of life, besides oncological safety. With the routine use of magnetic resonance imaging for local staging, intersphincteric resection has become a viable alternative to abdominoperineal resection. Similarly, there is enough evidence to consider laparoscopic surgery as feasible and oncologically safe for rectal cancer. Thus laparoscopic intersphincteric resection fulfills all the objectives of modern-day rectal cancer surgery. Here we describe the technical points while performing the surgery as well as short-term results of our own series.
Introduction
T
Technique
Abdominal part
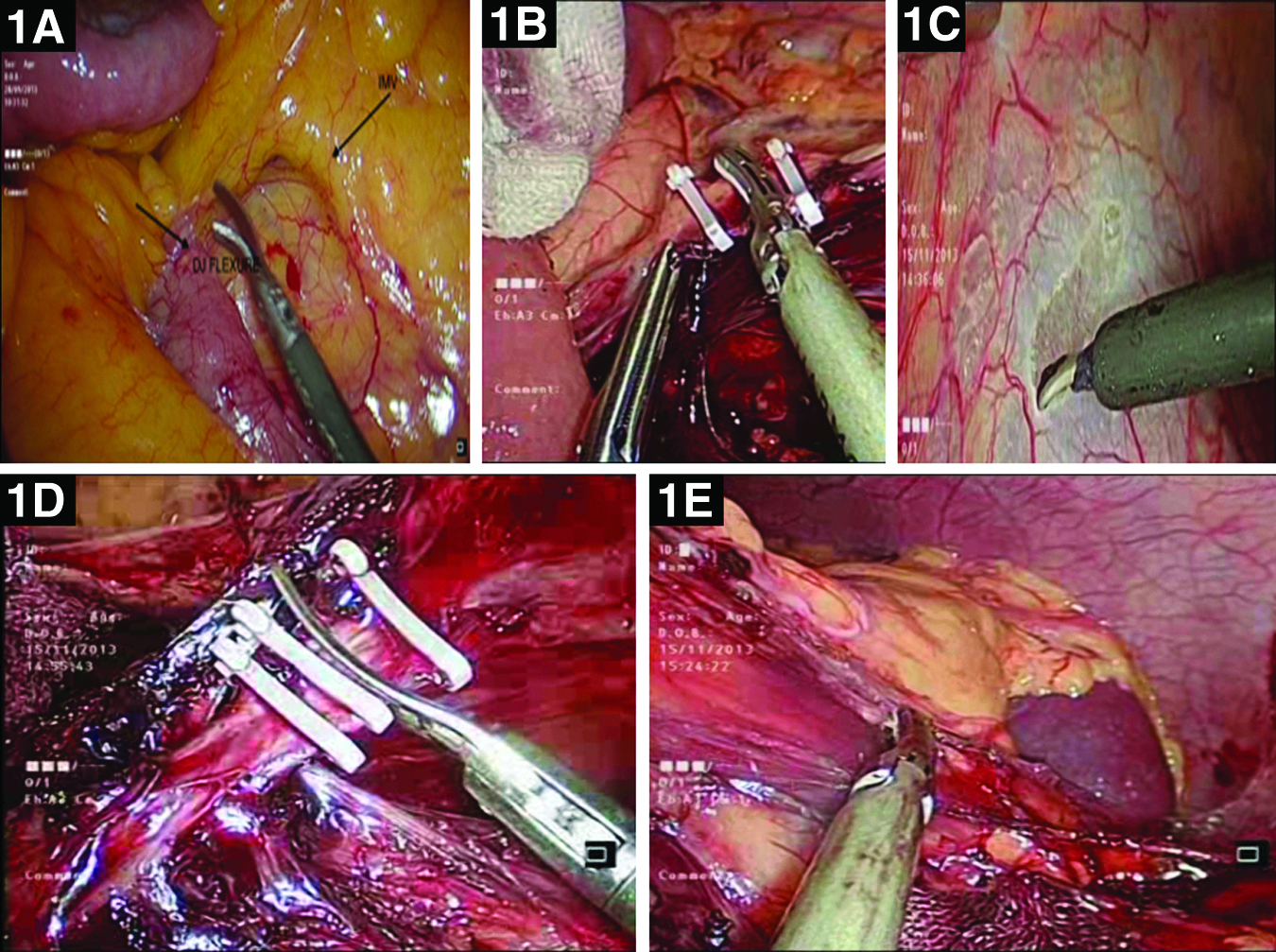
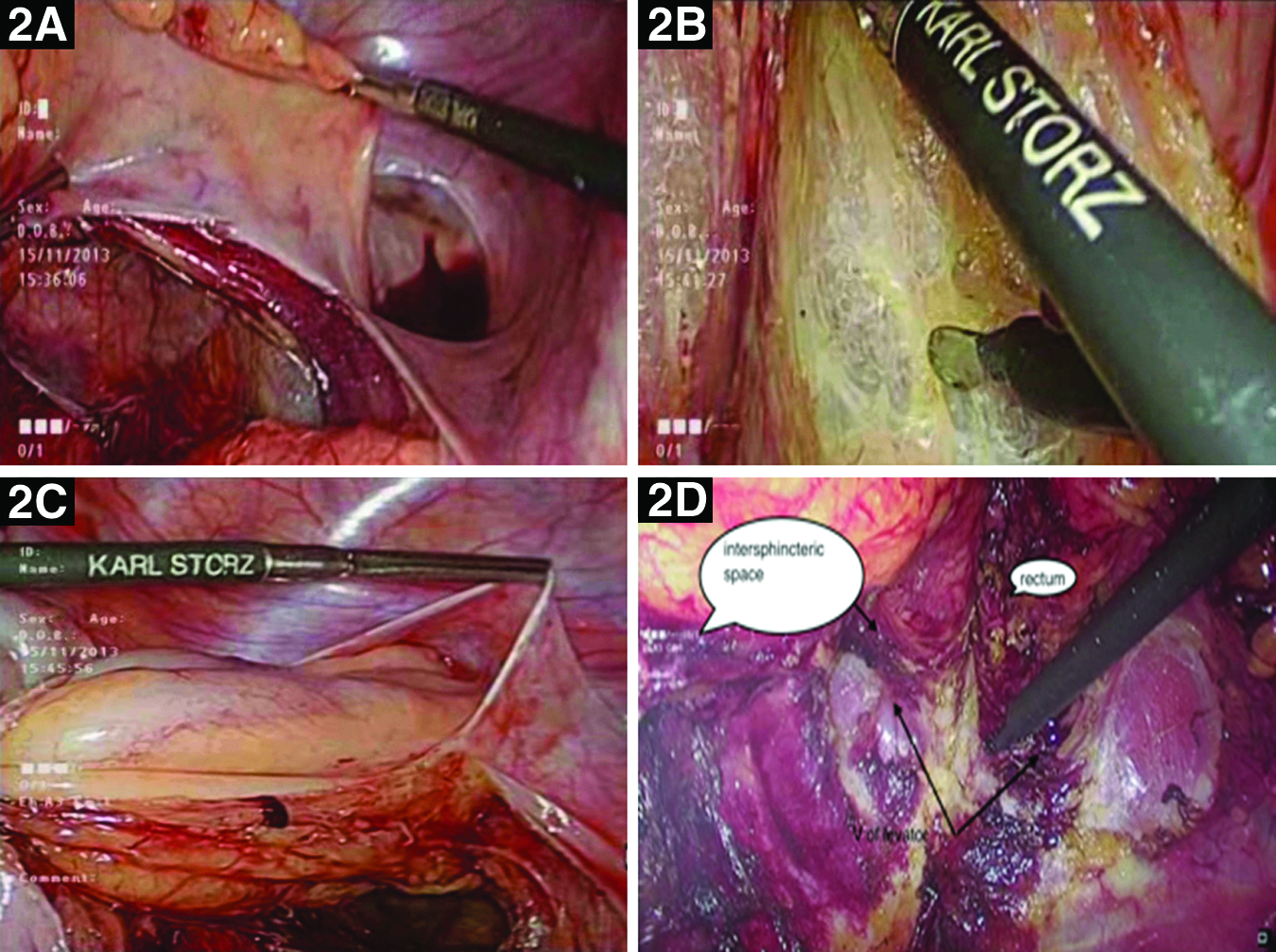
After an initial exploration of the abdomen and pelvis to ensure the absence of liver and peritoneal metastasis, standard total mesorectal excision is performed with high ligation of the inferior mesenteric artery, complete splenic flexure mobilization, and high ligation of the inferior mesenteric vein (if required for adequate colonic length) (Fig. 1). Total mesorectal excision is continued just outside the mesorectal fascia until the levator muscle is exposed circumferentially around the rectum (Fig. 2). The endopelvic fascia is then incised at the anorectal junction to open the superior aspect of the intersphincteric plane (Fig. 2D).
Perineal part
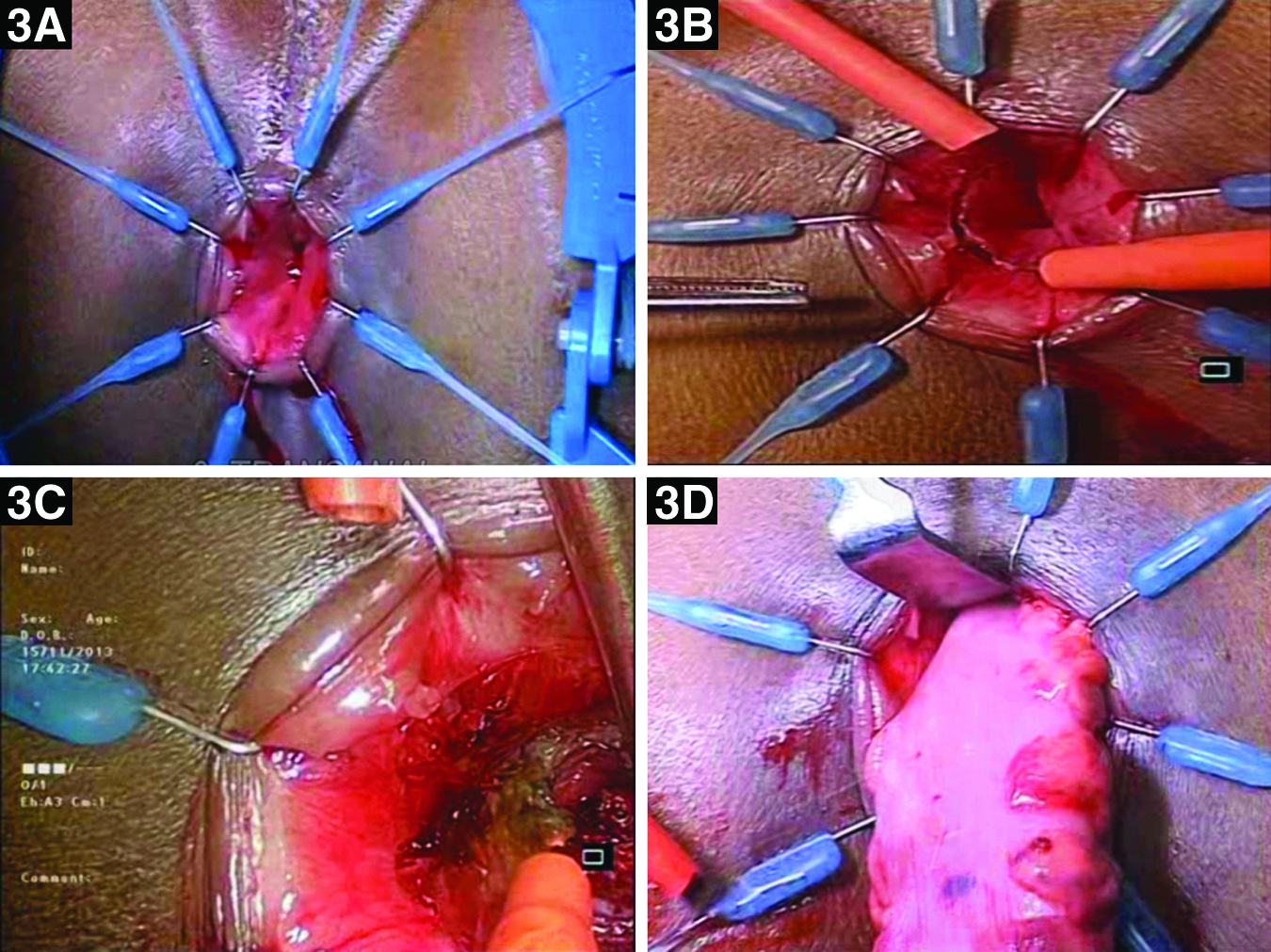
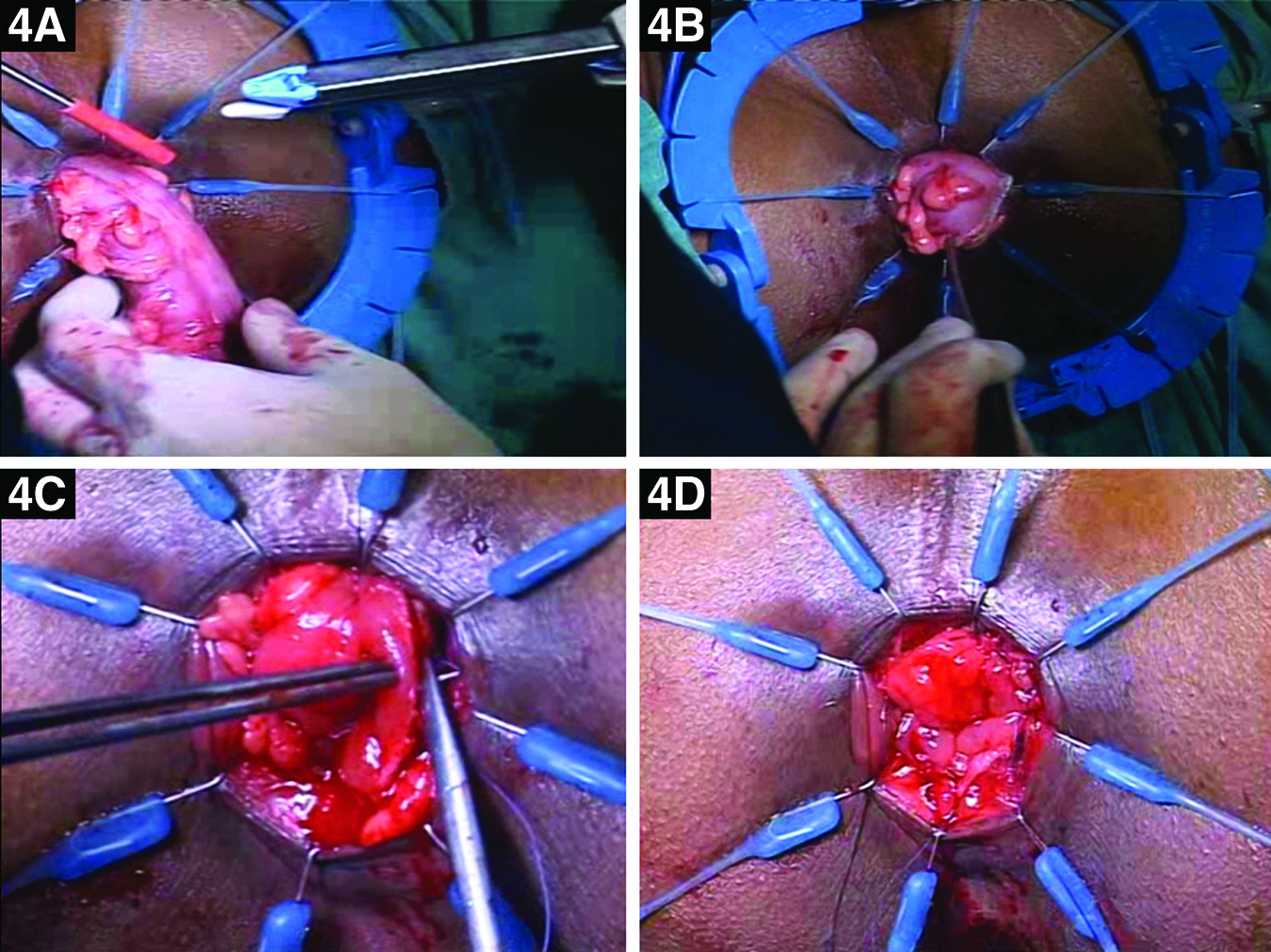
Transanal dissection is begun using the Lone Star® retractor system (CooperSurgical Inc., Trumbull, CT) (Fig. 3A). Dilute adrenaline saline solution is injected in the submucosal plane, and a mucosal incision is made about 1 cm distal to the lower end of the tumor (Fig. 3B) and deepened through the submucosa and internal anal sphincter. Dissection is then continued between the internal and external sphincters in the intersphincteric plane until the abdominal plane of dissection is met (Fig. 3C). The specimen is then delivered through the anal canal (Fig. 3D) and transected just proximal to the divided inferior mesenteric artery pedicle (Fig. 4A). An intraoperative frozen section is used to confirm a free distal resection margin, and a hand-sewn coloanal anastomosis is performed with interrupted absorbable sutures (Fig. 4B–D). A diversion loop ileostomy is done at the end of the procedure.
Results
The results shown below are derived from the retrospective review of a prospectively maintained database in the Division of Colorectal Surgery at Tata Memorial Centre, Mumbai, India, between July 2013 and December 2014. Following a detailed history and physical examination, all patients underwent a complete colonoscopy with biopsy and determination of serum carcinoembryonic antigen levels. Locoregional staging was achieved with a baseline magnetic resonance imaging scan of the pelvis. Contrast-enhanced computed tomography of the thorax and abdomen was performed to rule out metastatic disease. Neoadjuvant chemoradiotherapy was administered to all patients with a threatened circumferential resection margin and/or enlarged mesorectal nodes. All treatment decisions were taken by a multidisciplinary team comprising a colorectal surgeon, a radiation oncologist, a gastroenterologist, and a radiologist. Patients who were incontinent preoperatively or with infiltration of external sphincter on preoperative magnetic resonance imaging were offered abdominoperineal resection. All other patients with low rectal cancers were offered intersphincteric resection. The choice of a laparoscopic or open approach was based purely on the availability of facilities for laparoscopic surgery on that day.
Nineteen patients who underwent LISR during the study period were included. Demographic features are mentioned in Table 1. Fourteen patients (74%) had received neoadjuvant chemoradiotherapy, whereas the rest had undergone upfront surgery. None of the patients required conversion to the open procedure. The inferior mesenteric pedicle was ligated at the root in 13 patients, whereas in the rest it was ligated after the origin of the left colic artery. Two patients (10%) had postoperative complications. One patient had pelvic collection with a gape in the anastomotic suture line. The collection was drained via the transanal route, and subsequent resuturing was done. The other patient had a chyle leak, which was managed conservatively. The circumferential resection margin was positive in 1 patient, whereas it was free in the remaining 18 patients. The patient who had a positive circumferential resection margin underwent abdominoperineal resection in the second surgery.
CRM, circumferential resection margin; NACT/RT, neoadjuvant chemotherapy/radiotherapy; TME, total mesorectal excision.
Among the 19 patients, ileostomy closure had been done in 8 patients. Among these 8 patients, 6 patients had completed at least a 6-month follow-up after ileostomy closure. Hence, continence status was available for 6 patients. Continence was assessed based on symptoms and anal manometry (basal and squeeze pressure). Three patients were fully continent, whereas in the remaining 3 there was increased nocturnal frequency. However, true continence status cannot be known until at least 1 year after the ileostomy closure.
Discussion
Laparoscopic rectal surgery is regarded as complex because of the technical difficulties in pelvic exposure, dissection, and sphincter preservation. Experience of the surgical team is the most significant factor influencing the outcome, with studies showing shorter operative time and fewer postoperative complications with increasing experience. 2 Watanabe et al. 3 first described LISR in 2000. In published LISR series, the rates of conversion to open intersphincteric resection range from 0% to 5.2%.4,5 Risk factors for conversion include high body mass index, 6 bulky tumor, and narrow pelvis. It has been found that conversion to open surgery is associated with an increase in local recurrence. 7 Postoperative complications vary from 5.4% to 24.1%,8,9 with no postoperative mortality reported.
Fujii et al. 5 studied short-term outcomes of LISR from a Phase 2 trial to evaluate laparoscopic surgery for stage 0/1 rectal cancer in Japan and found that LISR is safe and feasible with a favorable short-term outcome. Oncological safety of LISR has been tested in several retrospective studies, although long-term results are not available. The local recurrence rate after LISR has varied between 2.6% and 7.4%,8,10 and the reported 3-year disease-free survival is 73%–93%.11,12 Functional outcomes following LISR have been reported to be satisfactory in the majority of studies, although very few of them have objectively documented the functional outcome. One of them had a mean Wexner continence score of 7.5±2.7. 11
At present there are no randomized trials comparing LISR with intersphincteric resection. Available evidence is based on retrospective comparative studies. Laurent et al. 13 compared the results of LISR done in 110 patients with intersphincteric resection done in 65 patients and found that the two procedures were comparable in terms of 5-year disease-free survival and local recurrence rate. Similarly, Park et al. 8 compared the results of 130 LISR patients with those of 80 intersphincteric resection patients and found that LISR is associated with significantly less blood loss and shorter hospital stay, although it is associated with a similar postoperative complication rate and a similar intermediate oncological outcome.
Conclusions
LISR is technically feasible and oncologically safe and in the future may replace abdominoperineal resection as the standard of care for a selected group of patients with low rectal cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.