
Abstract
Abstract
Background:
A novel technique using a single-incision laparoscopic approach has been described for several laparoscopic procedures. The aim of this article is to describe our experience with an alternative technique for laparoscopic distal pancreatectomies using a single-port platform.
Materials and Methods:
We have performed this procedure on 20 patients with pancreatic tumors in the pancreatic body or tail. A transumbilical incision is performed, and a single-incision platform is introduced. The stomach is sutured to the abdominal wall to expose the pancreas. This technique uses an additional 5-mm trocar in the left quadrant, ultimately used for drainage after the end of the procedure.
Results:
The median operative time was 176 minutes, and the hospital stay was 2 days. Mortality was 0%, and morbidity was 20%; 4 patients developed grade A pancreatic fistula. During follow-up (median, 11 months), no patient developed an incisional hernia. The cosmetic appearance of the incision was excellent in all cases.
Conclusions:
Laparoscopic distal pancreatectomy using a single-port platform is feasible and can be successfully performed by surgeons with experience in pancreatic and advanced laparoscopic surgery.
Introduction
I
We found few reports in the literature describing single-port distal pancreatectomy.5–10 The aim of this article is to report an alternative technique for laparoscopic distal pancreatectomy using a single-port platform, as well as the preliminary results of our initial experience with 20 cases.
Materials and Methods
From November 2012 to June 2014, 20 patients with pancreatic tumors in the pancreatic body or tail underwent laparoscopic distal pancreatectomy using a single-port platform at our center. Computed tomography, magnetic resonance imaging, or both were performed in all cases. Endoscopic ultrasound-guided fine-needle aspiration biopsy was performed in selected cases for diagnostic purposes. Intraductal papillary mucinous neoplasms and mucinous cystic neoplasms were handled according to the international consensus guidelines. 11
The advantages, disadvantages, and possible risks of the surgical procedure were explained to each patient, and informed consent was obtained. Data were collected prospectively.
Surgical technique
The patient is placed under general anesthesia and positioned in a supine and reverse Trendelenburg position. The surgeon is positioned between the patient's legs, while the assistant is on the right side, and the monitor is on the patient's cranial side. A transumbilical 3-cm skin incision is performed (Fig. 1a), and a single-incision advanced access platform with a gelatin cap, self-retaining sleeve, and wound protector (GelPOINT®; Applied Medical, Rancho Santa Margarita, CA) is introduced (Fig. 1b). One 5–12-mm and two 5–11-mm working ports are introduced through the single-port device (Fig. 1c). By using the gel cap and sleeves, no articulated instruments are necessary. CO2 pneumoperitoneum is established at 12 mm Hg. A rigid 30° 10-mm laparoscope is introduced. The single port is able to accommodate, at the same time and without triangulation prejudice, a 10-mm laparoscope, a 12-mm flexible stapler, and a 5-mm instrument such as a Harmonic® scalpel (Ethicon Endo Surgery, Cincinnati, OH), grasper, scissors, or dissector (Fig. 1d). The main modification of the original technique is the insertion of an additional 5-mm trocar in the left quadrant. This small opening is subsequently used for drainage. This additional trocar is used by the surgeon's right hand.
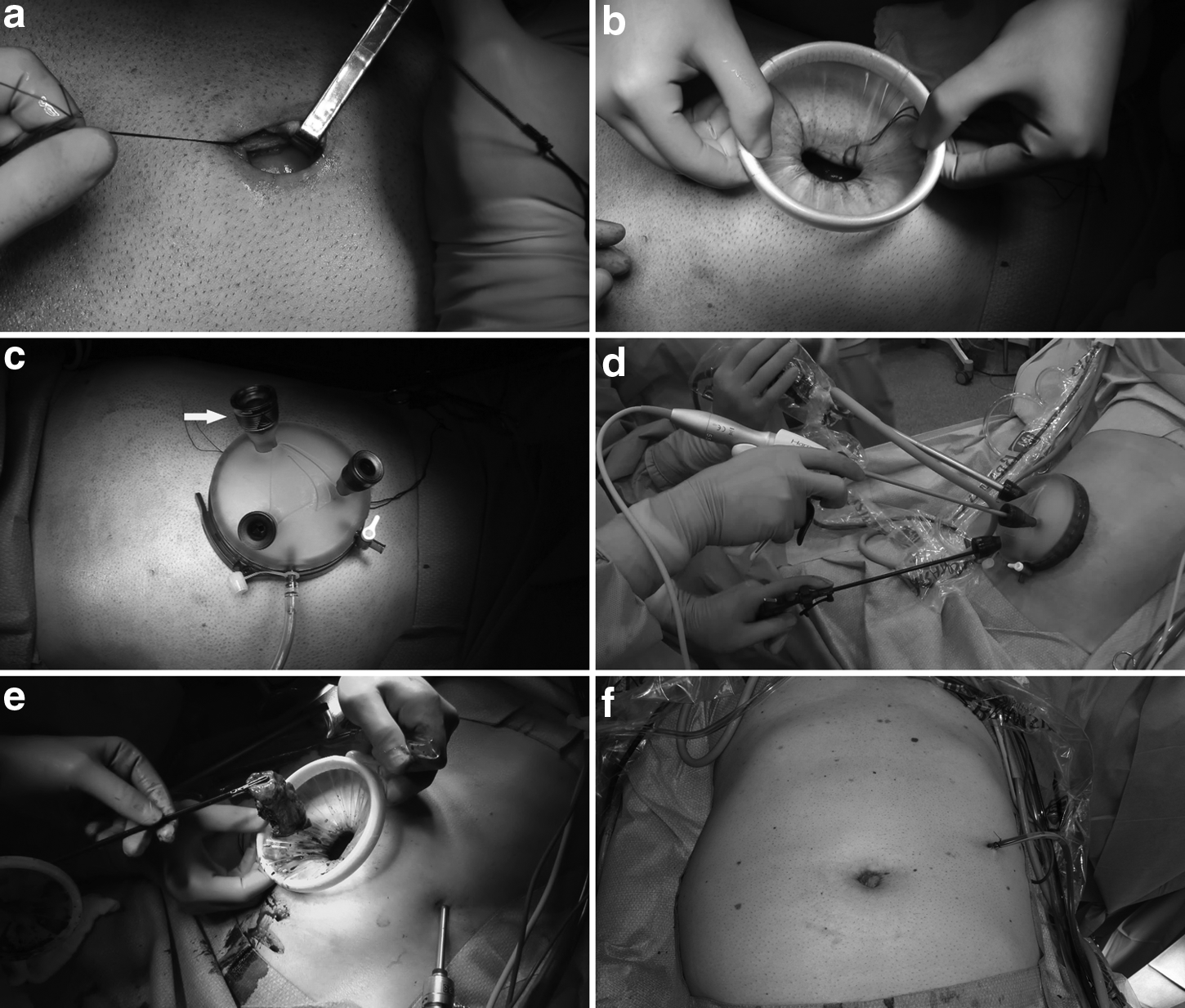
The single-port platform setup.
Access to the lesser sac is gained by opening the omentum along the greater curvature of the stomach using a Harmonic scalpel (Ultracision®; Ethicon Endo Surgery), taking care not to injure the gastroepliploic vessels. The stomach is sutured to the abdominal wall to expose the anterior face of the pancreatic body and tail (Fig. 2a). Once other lesions are discarded, intraoperative ultrasound (SonoSite, Inc., Bothell, WA) is used to ascertain the tumor's location and relationship to splenic vessels (Fig. 2b). If the splenic artery and vein are not involved by the tumor, the spleen is preserved. The ultrasound examination is useful in establishing a proximal negative margin. The peritoneum is released from the inferior border of the pancreas at the level of the tumor, exposing the splenic vein. A tunnel is opened behind the body or tail of the pancreas between the gland and the splenic vein by blunt dissection, and a cotton tape is placed around the pancreas. The tape is pulled upward, and the pancreas is dissected proximally, about 2–3 cm, to allow easy insertion of the stapler (Fig. 2c). The splenic artery is dissected, encircled, and kept away from the area to be divided. The pancreas is then divided with a flexible endostapler (Echelon Flex™ Endopath 60; Ethicon Endo Surgery) (Fig. 2d).

Laparoscopic spleen-preserving distal pancreatectomy using the single-port platform.
In 2 cases, splenectomies were performed. In these 2 cases, after division of the pancreas, the splenic vein was divided with a stapler, and the splenic artery was ligated with synthetic nonabsorbable suture (polyethylene terephthalate [Mersilene®] 2/0; Ethicon Endo Surgery) and divided between metallic clips. In the other cases, where the spleen was preserved, small venous and arterial branches from the pancreas were clipped or divided with a Harmonic scalpel along the body and tail of the pancreas (Fig. 2e). Distal pancreatectomy was then completed (Fig. 2f). The surgical specimen was removed through the single port (Fig. 1e). The raw surface of the pancreas was checked for bleeding, and hemostatic tissue was inserted into the dissected area. A closed suction drain was placed near the pancreatic stump and exteriorized through the 5-mm trocar in the left quadrant, after which the umbilical incision was closed (Fig. 1f).
In all cases, cefazolin was given prophylactically. The nasogastric tube was removed at the end of the procedure, and clear liquids were initiated on the first postoperative day. Drain fluid amylase was checked on postoperative Day 1 and before discharge. If the level was less than 300 U/L, the drain was removed on postoperative Day 7. If the drain fluid amylase level was higher than 300 U/L, it was checked again on postoperative Day 7, and if it remained high, a late removal of the drain was advised.
Results
The demographics and clinical characteristics of the patients are summarized in Table 1. There were 12 women and 8 men with a median age of 43.5 years (range, 20–71 years). In all cases, enucleation was not feasible because of proximity to the main pancreatic duct. The surgical margin was negative in all cases.
CT, computed tomography; EUS, endoscopic ultrasound; F, female; IPMN, intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; MEN-1, multiple endocrine neoplasia syndrome type 1; MRI, magnetic resonance imaging; NET, neuroendocrine tumor; SCN, serous cystic neoplasm; SPN, solid pseudopapillary neoplasm; US, ultrasonography.
We treated 10 neuroendocrine tumors, and all except one (in patient 4) were small, nonfunctioning tumors with preoperative signs of a low-grade neoplasm. The exception presented a large tumor (35 mm in diameter) with signs of vascular invasion, and therefore this patient underwent left pancreatectomy with splenectomy, lymphadenectomy, and removal of peripancreatic tissue. Final pathology disclosed a grade 2 neuroendocrine tumor (Ki-67 of 6%) with free surgical margins and no lymph node involvement. One patient was operated on for having a suspected neuroendocrine tumor, but the final diagnosis was a solid pseudopapillary neoplasm.
Ten cystic tumors were resected. Two patients in whom mucinous cystic neoplasm and intraductal papillary mucinous neoplasm were, respectively, suspected before surgery were definitively diagnosed with serous cystic neoplasm.
Data on the surgical aspects and results are shown in Table 2. Patients 4 and 5, in whom splenectomies were performed, required the longest operative times. An associated procedure, cholecystectomy, for cholelithiasis, was performed in patient 15. In all cases, the surgical specimen was retrieved through the single-port platform. The overall median operative time was 176 minutes (range, 110–340 minutes).
DP, spleen-preserving laparoscopic distal pancreatectomy using single-port platform; DP+C, laparoscopic distal pancreatectomy with cholecystectomy using a single-port platform; DP+S, laparoscopic distal pancreatectomy with splenectomy using a single-port platform; PF, pancreatic fistula.
Blood loss was less than 100 mL in all patients, except cases 4 and 5. None required blood transfusions, however. Four patients developed pancreatic fistula, all grade A, with no need for further treatment other than delayed removals of the drains. Median hospital stay was 2 days (range, 1–5 days). At a median follow-up of 11 months (range, 2–21 months) all patients are alive, but 1 patient developed exocrine and endocrine pancreatic insufficiency. No umbilical hernia or other late complications were observed during follow-up.
Discussion
Laparoscopic pancreatic surgery has experienced significant development in the last few years. Our experience with laparoscopic pancreatic resections began in 2001 with a distal pancreatectomy. 11 Similar to what other authors experienced, improvements in our expertise in advanced laparoscopic surgery allowed us to perform more complex operations such as central pancreatectomies, pancreatoduodenectomies, and resections of uncinate processes. 12 However, only laparoscopic distal pancreatectomy is considered a gold standard, primarily because techniques have been standardized. Based on the available data, laparoscopic distal pancreatectomy has an adequate safety profile, equivalent or better perioperative outcome, and noninferior oncologic outcome.2–4,13–16
Single-incision laparoscopy is less invasive than standard multiport laparoscopy but has unique difficulties for the laparoscopic surgeon. One is the significant limitation of retraction. Another issue is triangulation of instruments. The introduction of a camera and several instruments parallel to each other can result in decreased range of motion and collision of instruments. Another important issue is the drainage of the pancreatic stump. There are some findings that intraperitoneal drainage should not be eliminated after pancreatic resection.17,18 Therefore, we use routine drainage after pancreatic resections, especially in patients with a soft pancreas. 18 Some authors use the umbilical wound to exteriorize the drain.5,7 We prefer to exteriorize the drain in the left quadrant, which to our view is easier to manage and causes less discomfort than in the umbilicus. In order to make single-port laparoscopic distal pancreatectomy easier, we decided to use the future site of drainage, inserting an additional 5-mm trocar in the left quadrant. This trocar is used by the surgeon's right hand, decreasing triangulation problems and avoiding collisions. Another important maneuver is to suture the stomach to the abdominal wall to expose the pancreas. With these simple modifications in the original technique, we could perform this operation in all cases of distal pancreatectomies for low-grade pancreatic neoplasms since its introduction in our service.
Moreover, the adoption of a novel single-incision platform allowed the use of standard instruments because self-retaining sleeves maximized the internal working diameter. We were able to use a high-definition 10-mm laparoscope during all steps of the operation. Some authors have reported the use of a 5-mm camera, which in our opinion does not have the same quality of a 10-mm camera. Even during introduction of a 12-mm intraoperative ultrasound probe or a 12-mm flexible stapler, there was no need to replace the main laparoscope with a 5-mm one.
The two patients requiring splenectomy had increased operative time, blood loss, pancreatic fistula, and length of stay. Therefore, it is not clear if the single-port technique is advisable for such patients.
In the English literature, we found few cases of single-port pancreas resections reported.5–10 Most articles were case reports, and the largest series compiled 5 cases. 10 The main reason may be the need for special articulating instruments that require special skills. We believe that this alternative technique for single-incision surgery may reduce the learning curve for skill acquisition. Our initial experience with laparoscopic distal pancreatectomy using a single-port platform showed no exposure or triangulation difficulties, and operative time was not greater than our other laparoscopic cases.
The present series is, to our knowledge, the largest one published to date for pancreatic resection using a single-port platform. Although several issues such as cost and the learning curve remain to be studied, the cosmetic benefits of a limited-incision approach are obvious. In conclusion, the present series suggests that the alternative laparoscopic distal pancreatectomy using a single-port platform is feasible and safe and can be successfully performed by surgeons with experience in pancreatic and advanced laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.