
Abstract
Abstract
Purpose:
To develop a new approach of endoscopic resection for benign parotid tumor through a cosmetic retroauricular incision with a water sac establishing the operative space.
Materials and Methods:
Fifty-eight patients with benign parotid superficial lobe tumor were randomly assigned to an endoscopic (29 patients) or a conventional (29 patients) surgery group. The maximum diameter of the tumors was 6 cm. The subjective satisfaction scores with the incision scar, incision length, operative bleeding volume, postoperative complications, and recurrence rate were compared between the groups.
Results:
All operations were successfully performed. The endoscopic incision length (4.3±0.5 cm), bleeding volume (26.6±10.4 mL), and incidence of temporary facial paresis (6.9%) differed from the conventional surgery group (P<.05). The scars were almost invisible behind the ear. The mean patient satisfaction score was 8.9±0.7 in the endoscopic surgery group and 6.7±1.8 in the conventional surgery group (P<.05). Otherwise, Frey's syndrome and salivary fistula incidences were 3.4% (1/29) and 3.4% (1/29), respectively, in the endoscopic surgery group, which was not significantly different from the conventional surgery group (P>.05). No tumor recurrence was found during the 3–72 months of follow-up.
Conclusions:
Endoscopic resection through a cosmetic retroauricular incision with a water sac establishing operative space is a feasible method for treatment of benign parotid superficial lobe tumor. Its main advantages are that the small and concealed operative scars improved the cosmetic results, and it provided a novel method for establishing the operation working space that could reduce the operative trauma.
Introduction
B
In this study, we present a new endoscopic resection approach for benign parotid tumor through a small cosmetic retroauricular incision and provide a new method of establishing the operation cavity with a water sac.
Materials and Methods
Patients
From July, 2008 to August 2014, 58 patients with benign parotid tumor were involved in our study. All the patients underwent ultrasound, computerized tomographic or magnetic resonance imaging scan, and aspiration biopsy of the parotid tumor before the operation. The indication for surgery was a benign neoplasm with a maximum diameter of 6.0 cm located in the superficial lobe of the parotid. Suspected cases of malignant parotid tumor, sialadenitis in the acute inflammatory stage, radiotherapy history, preexisting facial paresis, and recurrent tumor were excluded.
Twenty-nine patients were selected randomly to undergo an endoscopic parotid surgery, and it was arranged that the other 29 patients would undergo conventional surgery. The endoscopic parotid surgery method was explained to all patients and their families before the operation, and their consent was obtained. The ethics committee of the Beijing Tongren Hospital had already approved the entire study.
Instruments
The endoscope (angle, 0°; diameter, 4 mm), television monitor, and equipment for endoscopic thyroid surgery were purchased from Karl Storz GmbH (Tuttlingen, Germany). The Harmonic® scalpel was purchased from Johnson & Johnson (Somerville, NJ). The Foley catheter prepared for making the water sac was purchased from Bard Healthcare Equipment (Beijing, People's Republic of China), a subsidiary of Bard (Murray Hill, NJ).
Surgical technique
All operations were done with the patient under general anesthesia. All the patients assumed the supine position with one shoulder padded slightly higher. Their heads were inclined to the healthy side. The whole operation process was performed by the surgeon himself holding the endoscope in the left hand. Figure 1A shows the position of the surgeon, the assistants, and the patient.

A small retroauricular inverted “V”-type serrated incision was performed. The incision went from a position 0.5 cm distant from the trailing edge of the ear lobe ditch, in parallel with the retroauricular groove up approximately 1.5–2.5 cm, and was curved, paralleling to the anterior margin of the sternocleidomastoid and extending approximately 1.5–2.7 cm to the mastoid tip. The incision did not exceed the hairline, and the lowest region was set above the earlobe (Fig. 1B–D).
When the incision was carried down to the subcutaneous tissue, a small tunnel was established at the front of the sternocleidomastoid and the deep surface of the platysma using forceps under the 4-mm-diameter, 0° angle endoscope. Then a Foley catheter was put into this tunnel. As the water was injected into the catheter slowly, the whole skin flaps were separated from the superficial lobe of the parotid (Fig. 2A). After 3 minutes of compression, the water sac was removed, and no bleeding was found. A stable operation space was maintained by pulling the skin flap with thyroid retractors.
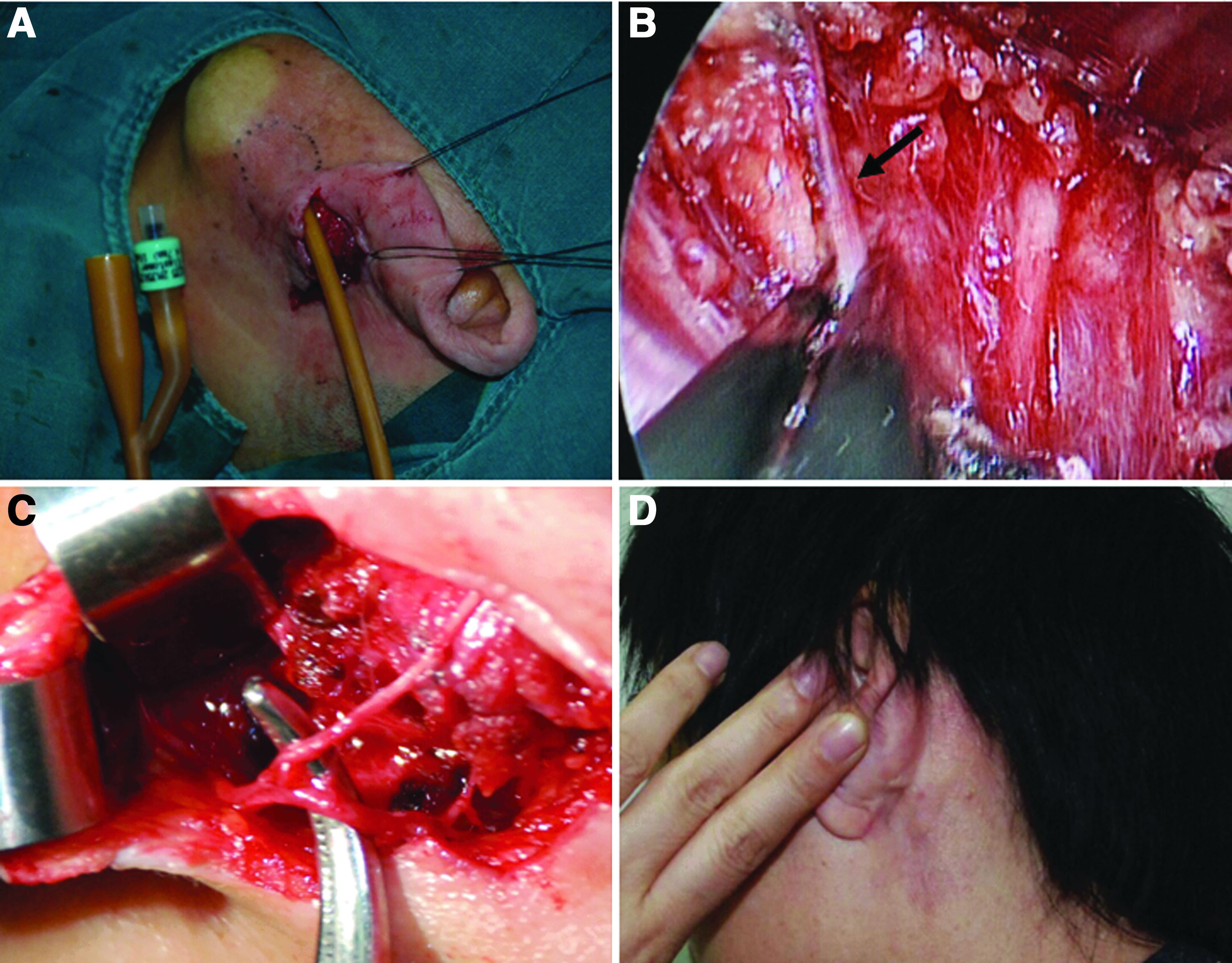
The next step was to identify the main trunk of the facial nerve. The endoscope provided a good illumination and magnified viewing for this procedure. With the illumination and amplification of the endoscope, the space among the anterior margin of the sternocleidomastoid, the lower wall of auditory meatus, and parotid was dissected clearly. The posterior auricular artery and its branches were electrocoagulated (Fig. 2B). The great auricular nerve was protected (Fig. 2C). The main facial nerve trunk and the bigaster branch of facial nerve were found and dissected at the upper end of the bigaster posterior ventral (Fig. 3A and C). Under the guidance of the trunk of the facial nerve, the superficial lobe and deep lobe of the parotid were dissected using the right angle forceps and the ultrasonic scalpel. Good illumination and magnified viewing enabled the whole course of each facial nerve branch to be separated clearly and safely from the glandular and subcutaneous tissues (Fig. 3B–D).
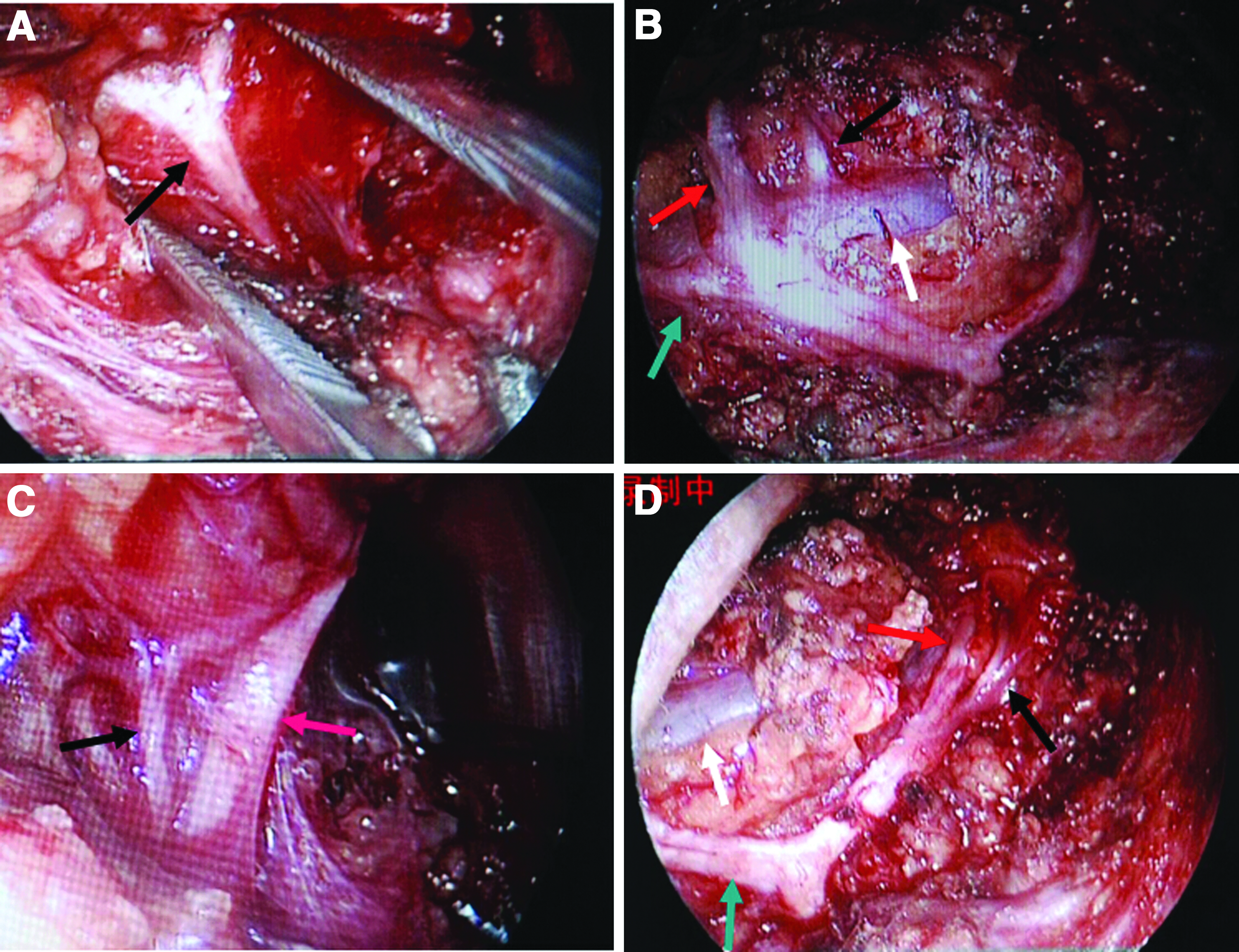
The main trunk and each peripheral nerve branch of the facial nerve, as well as the external jugular vein, are dissected step by step.
The tissue specimens were sent for frozen sectioning, and the results demonstrated that all tumors were benign. The tumor was excised together with a normal parotid parenchyma margin of 1–2 cm. For the final histopathological examination, all the specimens were sent for paraffin section. Finally, the wound was closed using subcuticular suture with 4-0 glycolic acid homopolymer suture (Dexon™; Covidien, Mansfield, MA), and a small Hemovac® (Zimmer, Warsaw, IN) drain was placed for drainage.
In the conventional group, surgery began with an “S”-shaped preauricular and submandibular incision. 12 The endoscope and the water sac were not used. The other steps were similar to the endoscopic group.
After the operation, belladonna tablets were taken orally in order to reduce the secretion of the parotid. Sutures were removed 7 days after the operation.
Four weeks after surgery, we evaluated the subjective satisfaction of patients with the incision scar using a self-made scale that depended on the satisfaction on the appearance of incision (length of incision and hiding degree), Frey's syndrome, facial numbness, facial pain, and facial itching with scores of 0, 1, or 2 for each item. For the satisfaction on the appearance of incision, 0 represents unsatisfied, 1 represents satisfied, and 2 represents very satisfied. For the other items, a score of 2 represents without, 1 represents mild, and 0 represents severe.
Statistical analysis
Statistical analyses were performed using SPSS version 17.0 software (SPSS, Inc., Chicago, IL). The data for each group were expressed as mean±standard deviation values. Statistical comparisons between the two groups, such as age, tumor diameter, operation time, operative bleeding, incision length, and subjective satisfaction with incision scar, were performed with Student's t tests. Statistical comparisons of the age constituent ratio and the incidence of complications between groups were performed with the chi-squared test. P<.05 was considered as statistically significant.
Results
Table 1 shows the comparison of endoscopic and conventional surgeries. The endoscopic group consisted of 9 males and 20 females ranging in age from 19 to 72 years (mean age, 45.1 years). The conventional surgery group consisted of 10 males and 19 females with a mean age of 45.7 years (range, 20–75 years). Both groups of patients were similar for age, sex, and tumor volume.
Data are mean±standard deviation values or ratio, unless otherwise specified.
P<.05.
In endoscopic surgery, all incisions healed fast and well and were hidden in the postauricular area (Fig. 2D). From the front, the incision could not be seen, and thus a cosmetic result was achieved. The lengths of endoscopic surgery incisions were much smaller than those of conventional surgeries (P<.05), and the bleeding volumes were smaller than those observed in the control group (P<.05). Both groups of patients were similar for age, sex, and tumor volume (P>.05). The incidence of temporary facial paresis in the endoscopic group was lower than in the conventional group (P<.05); otherwise, the incidence of Frey's syndrome and salivary fistula was not significantly different between the two groups (P>.05). On the self-made scale of subjective satisfaction with incision scar, the mean patient satisfaction score was much higher in the endoscopic group (mean, 8.9±0.7) compared with the control group (mean, 6.7±1.8) (P<.05).
All 29 operations of the endoscopic surgery group were successfully performed endoscopically, and no conversions to a conventional open resection were necessary. Postoperative histopathologic examination showed pleomorphic adenoma in 13 cases, basal cell adenoma in 5 cases, Warthin's tumor in 8 cases, lymphangioma in 1 case, lymphatic hemangioma in 1 case, and lipoma in 1 case in the endoscopic group. There was no significant difference from the conventional group, with pleomorphic adenoma in 14 cases, basal cell adenoma in 5 cases, Warthin's tumor in 7 cases, lymphangioma in 1 case, lymphatic hemangioma in 1 case, and lipoma in 1 case (P>.05). The tumor removal was intact in all the 58 cases with free resection margins from tumor invasion. All the patients were disease free at the follow-up visit in 3–72 months.
Discussion
In the present study, we not only created a new minimally invasive operation for the parotid gland by using an endoscopic technique and establishing working space with a water sac, but also obtained a more cosmetic result with a postauricular invisible incision.
Currently, the recommended treatment for small benign tumors located in the superficial lobe of the parotid gland is partial-superficial parotidectomy. 12 Conventional surgery for a benign parotid tumor is performed using an S- or Y-shaped skin incision to allow for complete tumor resection with safe facial nerve dissection. However, it involves a long incision and a high degree of trauma and leaves an obvious scar, which does not conform to the principles of minimally invasive surgery. Also, this visible and prominent scar troubled many patients, especially young patients. Many surgeons have tried to improve the cosmetic result by modifying the surgical technique, such as the superficial musculoaponeurotic system-lifting technique or facelift incision with reconstructive techniques.13,14 But, the scar is still obvious, and the degree of surgical trauma is still high.
Endoscopic surgery has many advantages, such as minimal morbidity and significantly decreased scarring, and it also enhances the surgeon's ability to view the area, decreasing the danger of injuring anatomic structures.7,8,15 It has been used in thyroid, submandibular gland, thyroglossal duct cyst, and branchial cleft cyst surgeries, as well as similar operations in the head and neck region. They all resulted patient satisfaction.16–19 Lin et al. 9 reported the first endoscope-assisted parotidectomy with a 60–81-mm modified “S”-incision, which, however, was still visible. In recent years, some researchers have developed the endoscope-assisted parotidectomy, with a more subtle incision for benign parotid disease.1–3,10,11 All these developments of parotid surgery focus on a cosmetic incision. At present there is no unified incision standard for endoscopic parotidectomy. Also, the maximum tumor diameter in all these investigations was less than 4 cm. In addition, no attempt has been reported on development of establishing the operation cavity until now. This is a difficulty for an endoscopic operation on the neck. In the previous endoscope-assisted parotidectomy, the endoscope was held by an assistant, which yielded a lack of flexibility in the operation. If the operation cavity could be made easily, the endoscope could be used flexibly by the surgeon him- or herself, which would be convenient to the operation process. In our study, we developed a new method of endoscopic resection for a benign parotid tumor not only in the cosmetic skin incision, but also in the operation for establishing the cavity.
In our study, we used a retroauricular incision located 1.5–2.5 cm above the earlobe behind the ear that was curved and extended approximately 1.5–2.7 cm. The incision length was 3.0–5.2 cm, and the lowest point of the incision was never lower than the earlobe. Considering that it is easier to cause a scar-making incision at the retroauricular groove than at other postauricular skin, we started the postauricular incision at a position 0.5 cm distant from the trailing edge of the ear lobe ditch. In addition, we introduced a serrated incision into our study. This type of incision can reduce the tension of incision skin, which reduced scar incidence and expanded the operation visual field. Through this serrated incision, larger tumors could be resected. Compared with the control group, this incision was much shorter and more subtle, with no scar formation on the face and neck. In other words, we achieved a better cosmetic result with a better operation visual field.
For endoscopic surgery, to make a good working space rapidly and successfully is an important step. In the previous reports, working spaces were all established through blunt dissection using forceps. This method has many adverse points, such as vascular injury, normal tissue injury, and the long time needed to make the working space. It also limited the size of the tumor that could be resected. Also, the endoscope must be held by an assistant in this process, which limited the flexibility of the operation. In the current study, we designed and made a water sac using a Foley catheter to establish the working space. Through expansion of the water sac, the flap above the parotid superficial lobe could be separated from the parotid as an intact tissue with little trauma. With this method, the assistant could be liberated from holding the endoscope. The endoscope could be used flexibly by the surgeon him- or herself in the whole operation. In a word, our operation was a real endoscope surgery. Holding the endoscope him- or herself, the surgeon can adjust the position and the direction of the endoscope according to the operation need. Thus, compared with the endoscope-assisted parotidectomy, the operation's visual field exposure was clearer, and the operation was more fluent with this method. After several minutes of compression with the water sac, little blood loss was found. This procedure reduced the operative bleeding and the tissue injury, relaxed the surgeon to a certain degree, and was convenient for performing the operation. Using this method, a tumor with a diameter of 6 cm was excised completely.
The endoscopic technique provides good illumination and magnification of parotid surgical procedures under the video monitor. With the endoscope, tissues, including the facial nerve trunk and branches, were identified and visualized clearly and dissected efficiently, and the great auricular nerve was also dissected efficiently and preserved. Damage to tissues during the surgery is minimized also by use of the Harmonic scalpel. The Harmonic scalpel-assisted superficial parotidectomy had been reported as a safe technique and associated with reduced surgical time and incidence of temporary postoperative facial nerve paresis compared with conventional techniques.20,21 It can cut and coagulate via ultrasonic blade vibrations at 55,000 Hz, which denatures proteins and forms a coagulum that seals the vessels. Vessels up to 5 mm in diameter can be sealed by coaptation. 22 In our study, with the help of the endoscope and the Harmonic scalpel, the operative field was clean and bloodless, and accidental injury or facial nerve branch and great auricular nerve abrasions were avoided.
Compared with the conventional group, the bleeding volume was less, the incidence of facial nerve paresis was lower, and the subjective satisfaction with the incision scar was higher in the endoscopic group. Because of the learning curve of the endoscopic operation, the whole operation time in the endoscopic group was not shorter but instead just similar to that of the control group. But, with more study and application of the endoscopic parotidectomy, its operation time is hoped to be shortened and may even be lower than the traditional operation time of paratoid gland in the future.
In 2005, Witt 23 reported that a 1-cm area of normal parotid parenchyma around a benign pleomorphic adenoma was a safe margin. In our study, we cut the parotid tumor with a 1–2-cm normal margin (1–2 cm of normal parotid tissue). Histopathological results showed that tumors in all the patients of our study were benign, including pleomorphic adenoma, basal cell adenoma, Warthin's tumor, lymphangioma, lymphatic hemangioma, and lipoma and no tumor invasion was found at the margin. Compared with the conventional group, during the following-up period, no recurrence was found in the endoscopic group.
Nowadays, endoscopic parotid surgery is still in its infancy. To master the skill of this operation, shorten the operation time, and reduce the operation's complications, more learning and practice on this surgery are needed. We have provided a good method for minimally invasive operation of the parotid gland in our study.
Conclusions
Endoscopic resection for a benign parotid tumor through a cosmetic retroauricular incision with a water sac establishing the operative space is a feasible technique for treatment of benign tumors located in the superficial lobe of the parotid. The advantages of this improved approach include an almost invisible scar with no scar formation occurring on the face and neck, superior visualization, magnification of key structures, and improvement of establishing the working space by using a water sac, which reduced tissue damages and the bleeding volume. It may extend the current realm of parotid surgery.
Footnotes
Acknowledgments
This work was supported by the Beijing City Health Personnel “Thou” 100 Level Candidates Project (number 2012-0053) and the training project of high-level medical technical personnel in the health system in Beijing City (number 2013-03-054).
Disclosure Statement
No competing financial interests exist.