
Abstract
Abstract
Objective:
Few studies have evaluated the role of laparoscopic dismembered pyeloplasty in the setting of recurrent ureteropelvic junction (UPJ) obstruction following open dismembered pyeloplasty in the pediatric population. We present our experience at a single institution.
Patients and Methods:
A retrospective analysis was performed of patients treated with laparoscopic pyeloplasty for secondary UPJ obstruction from March 2003 to August 2011 at a single institution. These patients were age and temporally matched with a control group of patients undergoing primary laparoscopic pyeloplasty.
Results:
In total, 5 patients were identified as having undergone laparoscopic pyeloplasty for secondary UPJ obstruction following open dismembered pyeloplasty. Operative time was longer in the secondary repair group compared with the control group (190 versus 141 minutes; P = .24), although this was complicated by 1 patient in the secondary repair group undergoing multiple procedures. Morphine equivalent use and length of stay were similar (4.1 versus 6.6 mg [P = .21] and 1.4 versus 1.2 days [P = .67] in control patients versus secondary repair patients, respectively). All of the 5 (100%) patients undergoing secondary repair had successful outcomes with improved hydronephrosis on ultrasound, and 4 of 4 (100%) had improved or normal T½ times on postoperative mercaptoacetyltriglycine (MAG3) renal scan. One family in each group declined the renal scan for personal reasons. No complications were noted with a mean follow-up time of 13 months in both groups.
Conclusions:
Laparoscopic repair of secondary UPJ obstruction is a well-tolerated and effective option. When this technique is compared with primary laparoscopic pyeloplasty, results appear equivalent even after failed open repair, with comparable postoperative narcotic requirement and length of stay. Further studies are needed to better define the role of secondary laparoscopic pyeloplasty in the pediatric population, especially with regard to cost compared with other open and minimally invasive techniques.
Introduction
A
We report here our outcomes of laparoscopic pyeloplasty for secondary UPJ obstruction following failed open repair with age and temporally matched controls undergoing primary laparoscopic pyeloplasty.
Patients and Methods
After obtaining approval from the Children's Mercy Hospital Institutional Review Board (protocol 12020108), we retrospectively reviewed the charts of patients having undergone pyeloplasty for UPJ obstruction from March 2003 to August 2011. Patients undergoing open dismembered pyeloplasty and those undergoing repair of primary UPJ obstruction were excluded.
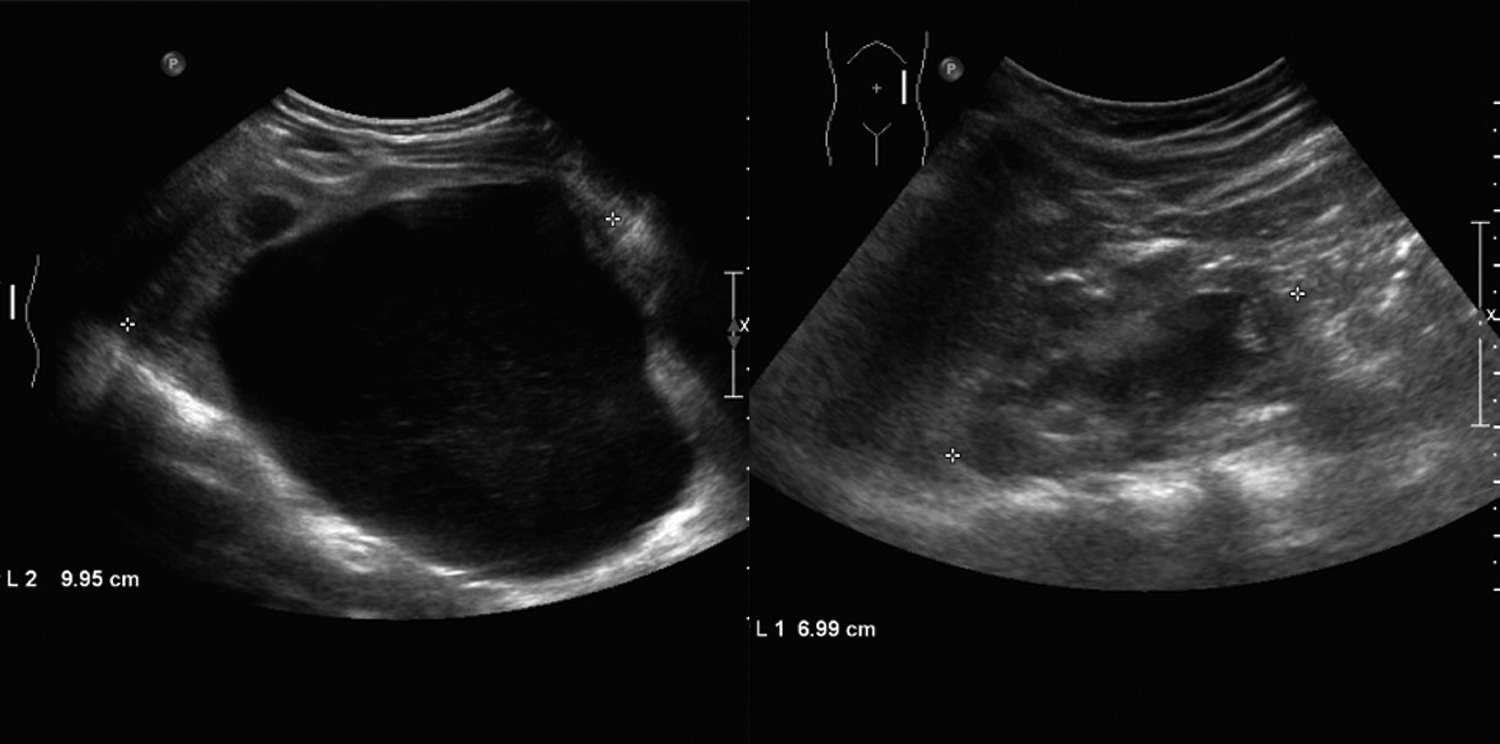
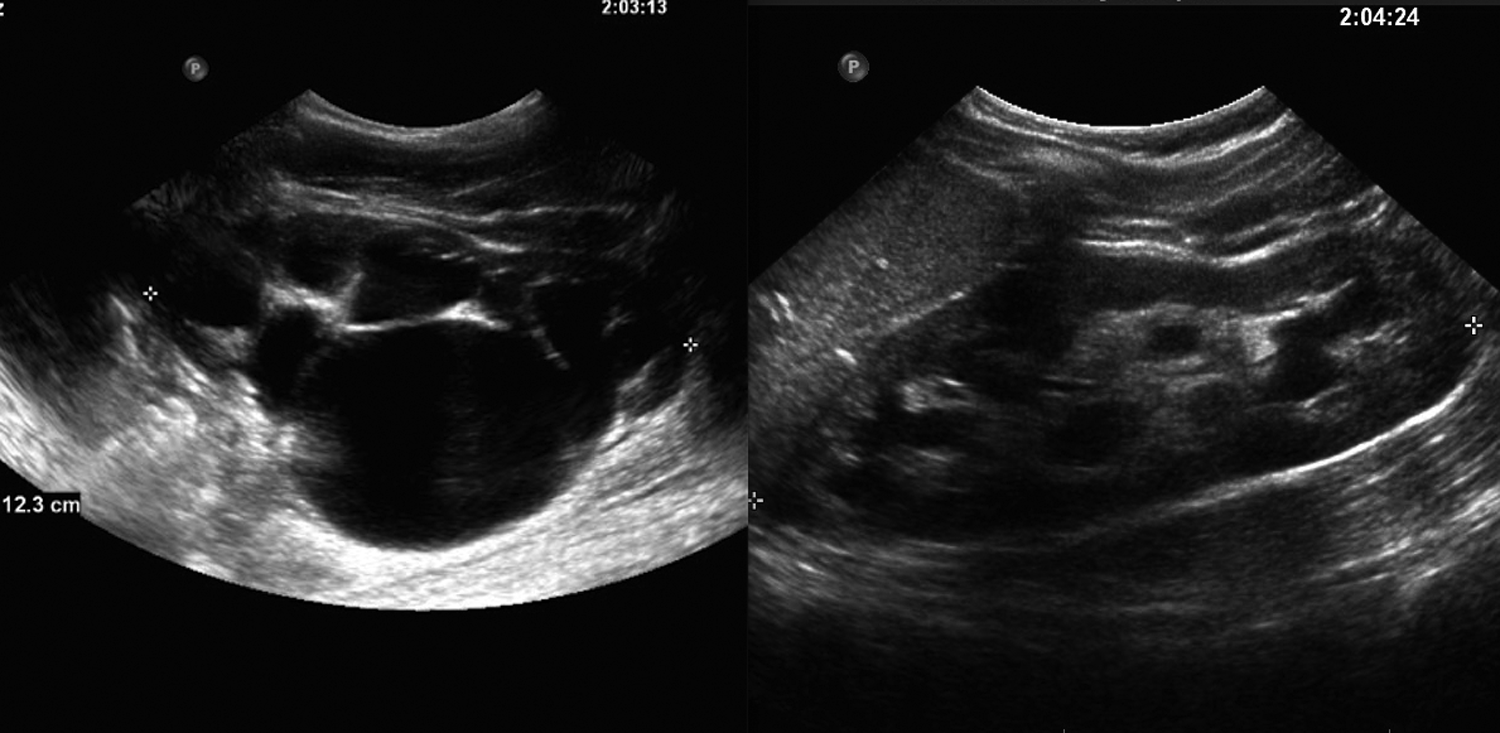
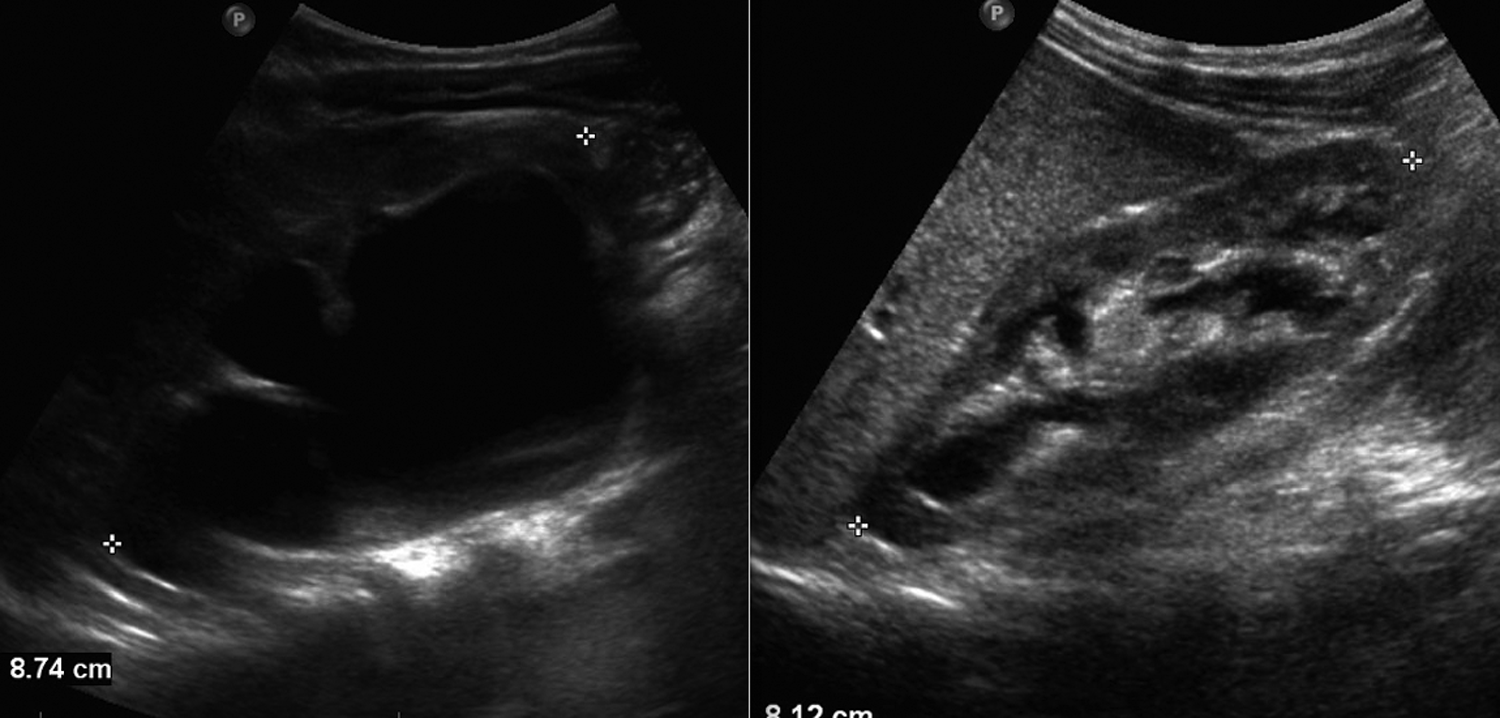
In total, 5 patients were identified as having undergone laparoscopic pyeloplasty for secondary UPJ obstruction following open dismembered pyeloplasty. Candidates for secondary UPJ repair included patients with increasing hydronephrosis and symptomatic obstruction proven on mercaptoacetyltriglycine (MAG3) renal scan preoperatively. Data collected included month and year of procedure, type of procedure, length of procedure, concurrent procedures, length of hospital stay, amount of narcotic pain medication used during inpatient stay, pre- and postoperative imaging, pre- and postoperative functional studies, and length of follow-up time. Narcotic pain use was converted to morphine equivalent and compared with that of age-matched patients to standardize data points. Preoperative imaging consisted of renal/bladder ultrasound scans (Figs. 1–5), and functional imaging was obtained by MAG3 renal scan.


Study patients were age and temporally matched with a control group of patients undergoing primary laparoscopic pyeloplasty in an attempt to eliminate bias derived from patient age or improved surgical efficiency over time. All procedures were performed by a single surgeon (J.M.G.).
Redo laparoscopic pyeloplasty was approached transperitoneally using a single 5- or 10-mm port umbilical port for the camera and two small 3-mm stab incisions without ports to accommodate two working instruments in the ipsilateral upper quadrant. The UPJ was dismembered, and a primary end-to-end anastomosis was performed prior to placing a double-J ureteral stent in antegrade fashion. The anastomosis was then completed over the stent. Flexible cystoscopy was performed immediately following the pyeloplasty without repositioning in order to confirm the appropriate distal stent position within the bladder. The incisions were infiltrated with local anesthesia, and a Foley catheter was placed at the end of the procedure. No wound or perinephric drain was placed at the time of surgery. Surgical time began with the initial incision and concluded with the placement of dressings and did include the time associated with cystoscopy. Postoperative labs were not routinely obtained. Foley catheters were removed on postoperative Day 1. Scheduled ketorolac was routinely used for postoperative pain control, and intravenous narcotics or oral oxycodone was provided for breakthrough pain as determined by the nursing staff according to standard pediatric nursing practice.
Postoperative evaluation consisted of a renal ultrasound with the ureteral stent in place at 3 weeks. Ureteral stents were removed at 6 weeks. Suppressive antibiotics were discontinued following removal of the ureteral stent. Repeat renal ultrasound was performed at 10 weeks, and a MAG3 renal scan was performed at 14–16 weeks postoperatively.
Success was defined as resolution of symptoms with stable or improved hydronephrosis on ultrasonography or an improvement in the drainage curve with a downward slope on a MAG3 renal scan. All patients underwent postoperative imaging and were followed up for a minimum of 5 months postoperatively. Statistical analysis was performed using two-tailed Student's t test.
Results
In total, 5 patients were identified as having undergone laparoscopic repair of secondary UPJ obstruction following failed open repair. Mean age of the study patients was 45.6 months (range, 13–111 months). These study patients were age-matched with patients who underwent laparoscopic primary UPJ obstruction repair with a mean age of 52 months (range, 16–114 months). All study procedures were temporally matched as well, and no matched procedure was separated by more than 6 months. Elapsed time between index case and revision for study Patients 1–5 was 8, 11, 23, 6, and 4 months, respectively. Individual patient data are summarized in Table 1.
Multiple procedures.
L, left; LOS, length of stay; OR, operating room; R, right; US, ultrasound.
Mean operative time in the secondary repair group was 190 minutes (range, 118–282 minutes). One outlier patient, included in the final analysis, underwent multiple procedures including cystoscopy, ureteral stent exchange, extensive ureterolysis, and laparoscopic repair of secondary UPJ obstruction (operative time, 282 minutes). Mean operative time in the primary repair group was 141 minutes (range, 114–208 minutes). Mean operative time was not statistically different between the two groups (P = .24).
Mean postoperative inpatient morphine equivalent usage was 6.6 mg, versus 4.1 mg in the primary repair group (P = .21). Patients were not routinely discharged with narcotic pain medication. Mean length of stay was 1.4 days in the control group versus 1.2 days in the study group (P = .67). No patients were re-admitted for complications associated with urologic treatment during the study period.
Mean follow-up time was 13 months in both the secondary and primary repair groups. No surgical complications were noted during the study period. All patients had resolution of symptoms following repair. All patients underwent postoperative imaging (Figs. 1–5). Follow-up ultrasound revealed unchanged or improved hydronephrosis in all primary and secondary repair patents. All patients undergoing postoperative MAG3 renal scan had normal or improved and descending diuretic T½ washout time curves. One family in each group declined the study for personal reasons but continued to be followed up by the noninvasive imaging in the clinic setting. Renal scan data are summarized in Table 2.
Renal scan refused.
NA, not available.
Discussion
Schuessler et al. 7 and Kavoussi and Peters 8 originally described laparoscopic pyeloplasty in the adult population in 1993. Since that time, laparoscopic pyeloplasty has been shown to have a shorter convalescence period and decreased morbidity compared with open surgery in the adult population. 4 Secondary laparoscopic pyeloplasty has been shown to have the same benefit and has been proven a viable treatment option for adults. Both Eden et al. 2 and Sundaram et al. 9 have previously described the success of secondary laparoscopic pyeloplasty following varying types of primary treatment, including endoscopic and open procedures.
Adoption of laparoscopic pyeloplasty in the pediatric population was the natural progression for a minimally invasive, less morbid procedure. Laparoscopic repair of primary UPJ obstruction in children was originally described in 1995 by Peters et al. 10 and is now well established. Although laparoscopic pyeloplasty was originally reserved for patients older than 5 years of age, it is now routinely performed on children of all ages. 11 Despite evidence revealing the efficacy and safety of laparoscopic pyeloplasty, many pediatric surgeons reserve this procedure for primary UPJ obstructions, fearing that intraabdominal adhesions and postoperative changes following primary repair failure may prevent safe renal hilar dissection or result in excessive operative times. To date, we have not identified what we would consider firm exclusion criteria for this approach, although multiple prior laparotomies would warrant concern.
Tan 12 first described successful laparoscopic repair of secondary UPJ obstruction in the pediatric population in 1999. All patients undergoing successful secondary laparoscopic procedures in this study previously failed a primary laparoscopic repair. Data regarding secondary laparoscopic pyeloplasty following failed open repair have been limited. The most compelling data are derived from a study by Piaggoi et al., 11 who reported an 80% success rate in 5 pediatric patients of varying ages. No surgical complications were noted in the study, and the success rate was equivalent to that of a matched secondary open pyeloplasty cohort.
To our knowledge, no study has compared patients undergoing secondary laparoscopic pyeloplasty following failed open repair with an age- and temporally matched cohort of primary laparoscopic repair patients. Comparing primary versus secondary laparoscopic pyeloplasty outcomes allows one to directly compare the effect of a failed open repair on the difficulty of secondary laparoscopic procedures. Although our sample size is limited, data from this study suggest that outcomes of secondary and primary laparoscopic pyeloplasties are equivalent and that failed open primary repair should not dissuade the surgeon from performing a minimally invasive procedure. Although operative times were longer in the secondary repair population, there was a trend toward comparable times, indicating improved efficiency with increased surgeon experience. As previously noted, ureteral stents were placed in an antegrade manner, and position was confirmed visually with flexible cystoscopy at the end of the procedure. This technique is timelier than retrograde stent placement and requires no radiation exposure or repositioning before beginning the laparoscopic portion of the procedure. In addition, retrograde placement of a ureteral stent prior to the procedure decompresses the renal pelvis, which can render the dissection more challenging.
Recently robotic-assisted laparoscopic procedures have provided an alternative minimally invasive option to managing both primary and secondary UPJ obstruction. Lindgren et al. 13 recently published an article in which they reviewed 14 patients who underwent robotic-assisted laparoscopic pyeloplasty for secondary UPJ obstruction. Results were equivalent to published success rates of both open and laparoscopic secondary UPJ repair. Mean operative time was 303 minutes in all patients; however, this included 3 patients who underwent ureterocalycostomy. Patients undergoing pyeloplasty had a mean operative time of 269 minutes, 89 minutes longer than the mean operative time in the current study. No information was provided regarding a trend toward decreased operative time. Recent national concern over increased healthcare costs has called into question the cost-effectiveness of robotic-assisted laparoscopic procedures. 14 At our institution, patient charge for procedures is based on a flat operating room time charge billed at $185 per minute, but all disposable instruments are included and do not command an extra charge. Prolongation of the procedure time by 89 minutes would equate to a $16,465 increase in the charge of the operation per patient based on time alone. That does not account for any additional disposable instrument, maintenance, or start-up costs associated with the robotic approach.
Given the relative rarity of pyeloplasty failure, the major limitation of this study is the small sample size, thereby limiting our ability for meaningful statistical analysis and universal recommendations. Although patients were age matched and theoretically similar in weight, morphine equivalent use was recorded as total milligrams used and not weight based. This documentation technique is unlikely to change the outcome of the study. Not all patients underwent a pre- and/or postintervention MAG3 renal scan (80%). Consistent with previous studies, success was defined as symptom resolution with unchanged or improved hydronephrosis. 11
Conclusions
Laparoscopic repair of secondary UPJ obstruction is a well-tolerated and effective option. When compared with primary laparoscopic pyeloplasty, results appear equivalent even after failed open repair, with comparable postoperative narcotic requirement and length of stay. Further studies are needed to better define the role of secondary laparoscopic pyeloplasty in the pediatric population, especially with regard to cost compared with other open and minimally invasive techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.