
Abstract
Abstract
Objectives:
To determine the long-term outcomes and quality of life (QoL) following laparoscopic mesh repair of inguinal hernias using the hernia-specific Carolinas Comfort Scale® (CCS) questionnaire (Carolinas Laparoscopic and Advanced Surgery Program, Carolinas HealthCare System, Charlotte, NC).
Materials and Methods:
All patients who underwent elective primary or recurrent laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair from January 2005 to May 2010 were identified from a prospectively maintained clinical database. Baseline patient characteristics were recorded, including occupation, in addition to mean operating time, hernia recurrence rates, and postoperative CSS.
Results:
Four hundred fifty-nine patients underwent surgery during the study period. The median follow-up interval from the date of operation to the date the questionnaire sent was 23 months (interquartile range, 32 months), and the total number of valid responses was 250. The median age of patients was 58 years (interquartile range, 21 years). The median operating time was 42 minutes (interquartile range, 21 minutes). Thirty-five patients (15%) and 15 patients (12%) had bilateral and recurrent hernia repairs, respectively. Three patients (1.1%) were confirmed to have hernia recurrence. Analysis of the CSS scores revealed that 41 patients (16%) reported pain, 44 (18%) reported mesh sensation, and 25 (10%) reported movement limitation. However, severe or disabling mesh-related symptoms were present in 5 patients (2%) for the pain category, in 8 patients (3%) for the mesh sensation category, and in 9 patients (3%) for the movement limitation symptom. The number of patients who were completely asymptomatic in all three symptom categories was 190 (24%). The only significant risk factor for developing mesh-related symptoms was young age at the time of surgery.
Conclusions:
Patient-reported medium-term symptoms following laparoscopic inguinal hernia repair appear common; however, the prevalence of severe or disabling symptoms is low.
Introduction
I
The Carolinas Comfort Scale (CCS) better assesses QoL and satisfaction of patients who have undergone surgical hernia repair than the generic 36-item Short Form. 4 The CSS questionnaire is a 23-item validated questionnaire that measures the severity of pain, sensation of the mesh, and movement limitations due to the mesh in the following eight activities: laying down, bending over, sitting up, activities of daily life, coughing or deep breathing, walking, stairs, and exercise. Patients are asked to rate the symptoms on a 6-point Likert scale for each activity, with 0 corresponding to no symptoms and 5 to disabling symptoms (see Supplementary Data; Supplementary Data are available online at www.liebertpub.com/lap). The CCS score is derived by totaling the scores from each of the 23 items, where the best possible score is 0 and the worst is 115. The primary objective of this study was to determine the incidence of chronic pain and QoL after laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair using the short and hernia-specific CCS questionnaire.
Materials and Methods
All patients who underwent elective surgery with the TAPP technique with mesh fixation from January 2005 to May 2010 at our center were included in the study. Following local Research and Developmental approval, data were retrieved from the operating room's database and the patient's clinical records.
All the repairs were carried out by three consultant surgeons using the standard technique and lightweight 10-×15-cm polypropylene mesh fixed with titanium staples. Patients were asked to fill out the CCS questionnaire and a general questionnaire asking about the recurrence, overall satisfaction with the procedure, and whether their occupation involves heavy lifting. Patients were mailed the questionnaires and provided with stamped, self-addressed envelopes to be mailed back. Telephone interviews, clinical notes review, and outpatient assessments were carried out to confirm the positive replies regarding the recurrences. The final follow-up date was determined on the basis of the most recent contact by survey, telephone, or outpatient review.
Statistical analysis
Data analysis was performed using Statistical Package for Social Sciences (SPSS) for Windows version 17 software (IBM, Armonk, NY). Chi-squared tests were used to compare and assess correlation between categorical variables and patients with or without symptoms. Continuous variables were compiled with medians and interquartile ranges and tested for their normality. The Mann–Whitney U test was used to compare symptomatic and asymptomatic patients. P<.050 was considered statistically significant. When assessing QoL, patients were classified as asymptomatic (no symptoms or not bothersome) or symptomatic (mild to disabling symptoms) based on each symptom's (pain, mesh sensation, and movement limitation) maximum score from all eight activities.
Results
In total, 459 patients underwent surgery during the study period. The total number of responses received was 274 (60%). Twenty-four responses were excluded (Table 1). The median follow-up duration was 23 months (interquartile range, 32 months). The majority of patients (>90%) underwent day-case surgery. Five patients (2%) had postoperative complications that were managed conservatively: 2 patients had scrotal hematoma, 1 patient had port-site wound infection, and 2 patients developed urinary retention. Table 1 shows the baseline characteristics of the patients. Three patients (<1%) developed recurrent hernias and had undergone further surgery at the time of completing the general questionnaire. Three responders who reported that the hernia might have recurred were further evaluated as outpatients and were not found to have recurrence.
Data are number, mean (interquartile range), or number (%), as indicated.
The total number of patients in the asymptomatic group was 190 (76%) compared with 60 (24%) in the symptomatic group. In the symptomatic group, 29 patients (11.6%) reported mild and bothersome symptoms, 19 (7.6%) moderate and/or daily symptoms, 9 (3.6%) severe symptoms, and 3 (1.2%) disabling symptoms. Both groups showed similar characteristics in terms of operating time, occupation involving heavy lifting status, and site or type of hernia repair between symptomatic and asymptomatic categories. Only younger age (53 versus 58 years; P=.025) seemed to predict development of symptoms (Table 2).
By Mann–Whitney U test.
By chi-squared test.
Pain
There were 209 patients (84%) who were asymptomatic for pain, 23 (9%) with mild but bothersome pain, 13 (5%) with moderate and or daily pain, 3 (1%) with severe pain, and 2 (<1%) with disabling pain. Comparison of variables between the asymptomatic and symptomatic groups showed that younger age (median of 60 versus 54 years; P=.045) was predictive of developing chronic pain. Percentage of pain symptoms in each activity of the CSS was as follows: laying down, 6%; bending over, 8%; sitting up, 6%; activities of daily life, 8%; coughing or deep breathing, 6%; walking, 8%; stairs, 6%; and exercise, 9%. The highest incidence of pain was in exercising activity, a more rigorous and physically demanding activity, followed by bending over.
Mesh sensation
Responding to the question of sensation of mesh as an isolated symptom, 18% of patients reported symptoms during any CSS activity. There were 19 (8%) patients with mild but bothersome symptoms, 17 (7%) with moderate and or daily symptoms, 7 (3%) with severe symptoms, and 1 (<1%) with disabling symptoms. No predictive features for developing symptoms of mesh sensation were identified. Eighteen patients (7%) were only symptomatic for mesh sensation without being symptomatic to pain or movement limitation. This suggests that patients tend to experience the sensation of mesh in a way that is not necessarily related to pain and movement limitation. Percentage of mesh sensation symptoms in each activity of CSS was as follows: laying down, 9%; bending over, 10%; sitting up, 7%; activities of daily life, 9%; coughing or deep breathing, 7%; walking, 7%; stairs, 8%; and exercise, 10%.
Movement limitation
Only 25/250 (10%) patients reported symptoms in this category for any CSS activities. Severe movement limitation and a disabling symptom were experienced by 3% of patients (9/250). Similar to the pain and mesh sensation category, more patients (19/250, 8%) experienced symptoms during a “bending over” activity, a common everyday activity that stretches the abdominal wall, compared with the rest of the activities.
Discussion
In this study, the majority of patients (76%) who returned a completed CSS questionnaire were asymptomatic after a median follow-up of 2 years. There was no significant association between mesh-related symptoms and the type of hernia (primary or recurrent, unilateral or bilateral), operating time, or patient's occupations. Younger patients, however, were more likely to develop mesh-related symptoms, especially chronic pain. This is in agreement with findings from a large Danish epidemiological study where significantly less chronic pain was observed in patients over 65 years of age undergoing open hernia repair. 5 Similarly, in a separate study of laparoscopic inguinal hernia repairs, age of <50 years was significantly correlated (P<.001) with chronic postoperative pain. 6 In our study, although 16% and 18% of patients developed pain and mesh sensation symptoms, respectively, fewer than 3% reported severe or disabling symptoms (Fig. 1).
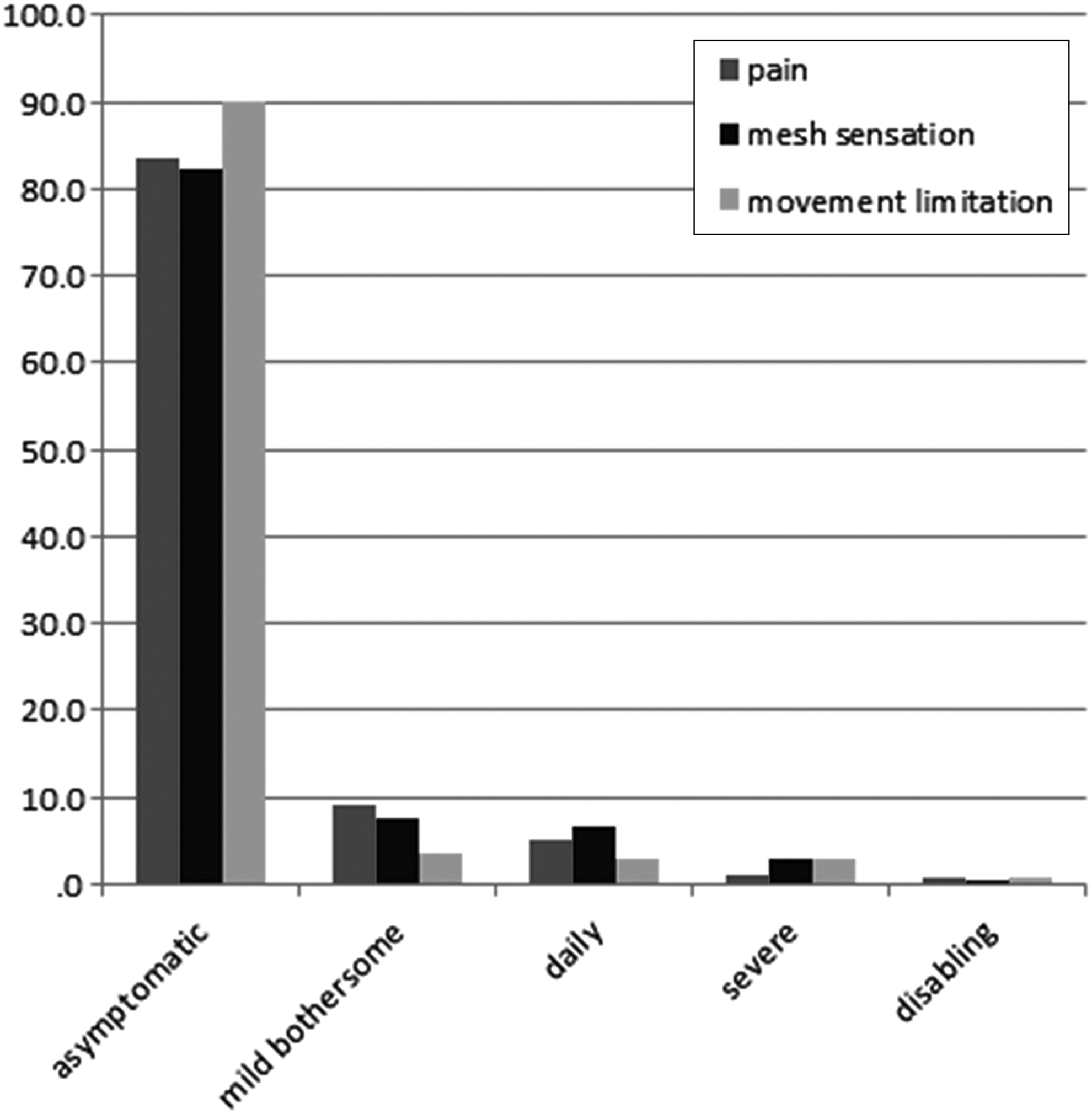
Percentage of patients with severity grades for mesh-related symptoms.
In a meta-analysis of randomized controlled trials, the incidence of chronic pain was reported to be 13.8% in the laparoscopic group. 7 The slight increase in the incidence of chronic pain in our study could be attributed to use of titanium staples to fix the mesh. The use of fibrin glue provides distinct advantages in laparoscopic repair of inguinal hernia by lowering the incidence of postoperative pain. 8 Despite this, the incidence of severe or disabling symptoms in our study is less than previously reported rates of up to 6%.5,9 In addition, 89% of patients reported overall satisfaction with the procedure by rating ≥8 on the visual analog score, with a range from 0 (highly dissatisfied) to 10 (delighted). In this study the questionnaire response rate was 60% (n=274), but in order to have a 95% confidence levels with a 5% margin of error in our results, we would have required at least 212 patients to analyze outcomes from a representative sample from our population.
Conclusions
Laparoscopic TAPP hernia repair offers good outcomes for patients in the medium term. The CCS questionnaire is a useful tool for analyzing patient-reported outcomes following inguinal hernia repair, in particular for the effects of the prosthetic mesh on quality of life while performing routine daily activities. Further prospective randomized trials based on CSS are needed to confirm the findings in our study.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.