
Abstract
Abstract
Background:
Laparoscopic gastrostomy is a widely used interventional procedure in pediatric surgery. We report comparative data for two endosurgical methods for the fixation of the stomach against the abdominal wall, using the U-stitches technique and the Saf-T-Pexy® (Halyard Health Inc., Alpharetta, GA) system.
Materials and Methods:
Within the period from January 2012 to June 2014 we performed 24 operations involving laparoscopic placement of a gastrostomy tube using U-stitches (Group I) and 24 operations using the Saf-T-Pexy system (Group II). The two groups of patients were compared in terms of demographics and intraoperative and postoperative results.
Results:
No statistical difference (P > .05) was found while comparing the patients' demographics and intra- and postoperative results. The mean duration of the surgical procedure in Group I was 23.75 minutes; in contrast, the mean duration of surgery in Group II was 22.71 minutes (P > .05). The time to first feeding (9.96 hours versus 10.63 hours) and time to full enteral feeding (23.13 hours versus 24.5 hours) were consistent for patients from both groups (P > .05). A similar postoperative duration of stay was recorded for the patients from the comparison groups (7.25 days versus 7.21 days; P > .05). Statistical analysis of the two groups demonstrated a significant difference in the parameters of minor postoperative complications (41.67% versus 8.33%; P < .05).
Conclusions:
Use of the Saf-T-Pexy system is a simple and efficient method for gastropexy involving placement of gastrostomy tubes that significantly reduces the number of postoperative complications.
Introduction
A
Materials and Methods
Within the period from January 2012 to June 2014 we performed 24 laparoscopic surgeries involving placement of a gastrostomy tube. The technique with U-stitches was used for the fixation of the stomach in 24 patients (Group I). The innovative gastropexy system using the Saf-T-Pexy system was applied on a further 24 patients (Group II).
Laparoscopic placement of a gastrostomy tube requires a patient to be specially positioned on the surgical table—the reverse Trendelenburg position with the head end of the table raised and inclined to 30°, so that gravity distances the intestinal tract from the surgery site. A correct display position is also important to ensure that the surgeon has an optimal view of the operating area inside the child's body. The portable consoles now in use in integrated operating rooms enable the display to be positioned opposite the surgeon at the hand level. The screen plane was perpendicular to the endosurgeon's visual axis, allowing an image similar to open surgery images to be transmitted. When performing gastrostomy surgery, the surgeon was standing close to the patient's feet, with the screen positioned adjacent to the patient's head. The laparoscopic approach applied in our research involved the use of the MIC-KEY® low-profile gastrostomy feeding tube (Halyard Health Inc.) and the Saf-T-Pexy system available in the Introducer Kits (Halyard Health Inc.) designed for their placement.
In the majority of cases, the sites of laparoscopic ports were determined according to strict guidelines. In this research we favored the two-port laparoscopic gastrostomy technique. The surgical procedure commenced with the umbilical insertion of the optical cannula and the 3.9-mm 30° laparoscope (Karl Storz GmbH, Tuttlingen, Germany) into the abdominal cavity. The laparoscopy confirmed the stomach's size and position, as well as the presence or absence of peritoneal adhesions.
Gastropexy techniques
Gastropexy method using U-stitches
The position of a future gastrostomy tube was determined in the left epigastrium region by external palpation of the anterior abdominal wall. A small skin incision was made in this site. The cutting edge incised all layers of the abdominal wall until the endoscope could be seen. A 3-mm duckbill-type atraumatic fenestrated forceps was inserted into the incision. The forceps fixed the anterior wall of the stomach in the intended stoma placement site. The anterior wall of the stomach was secured with two U-shaped anchor stitches transabdominally, to the right and to the left of the endoscopic clamp. The stomach was filled with air through the preinserted nasogastric tube. The fixing clamp was removed, and the gastric wall was punctured with the 14-gauge needle. A catheter was introduced into the gastric cavity using the Seldinger technique. The gastrostomic opening was dilatated with interchangeable gastric dilatators to the size of the tube being inserted. A MIC-KEY low-profile gastrostomy feeding tube was selected on a strictly individual basis based on an additional tube parameter, the stoma length, being the distance from the internal fixation balloon to its external fixation plate. This length is measured with the stoma measuring device, a graduated balloon catheter, prior to the insertion. Once the feeding tube was inserted in the stomach, the gastrostomy balloon was insufflated with sterile water through the side port. Carbon dioxide was then desufflated from the abdominal cavity, and U-stitches were made above the side supports of the gastrostomy tube.
Gastrostopexy method using the Saf-T-Pexy system (Figs. 1 and 2)
This gastropexy system, used as an alternative method for fixation of the stomach against the abdominal wall, consists of four needles with T-anchor sutures equipped with the Saf-T-Pexy polyurethane external locking mechanism.

Laparoscopic view on gastropexy using the Saf-T-Pexy system (Halyard Health).
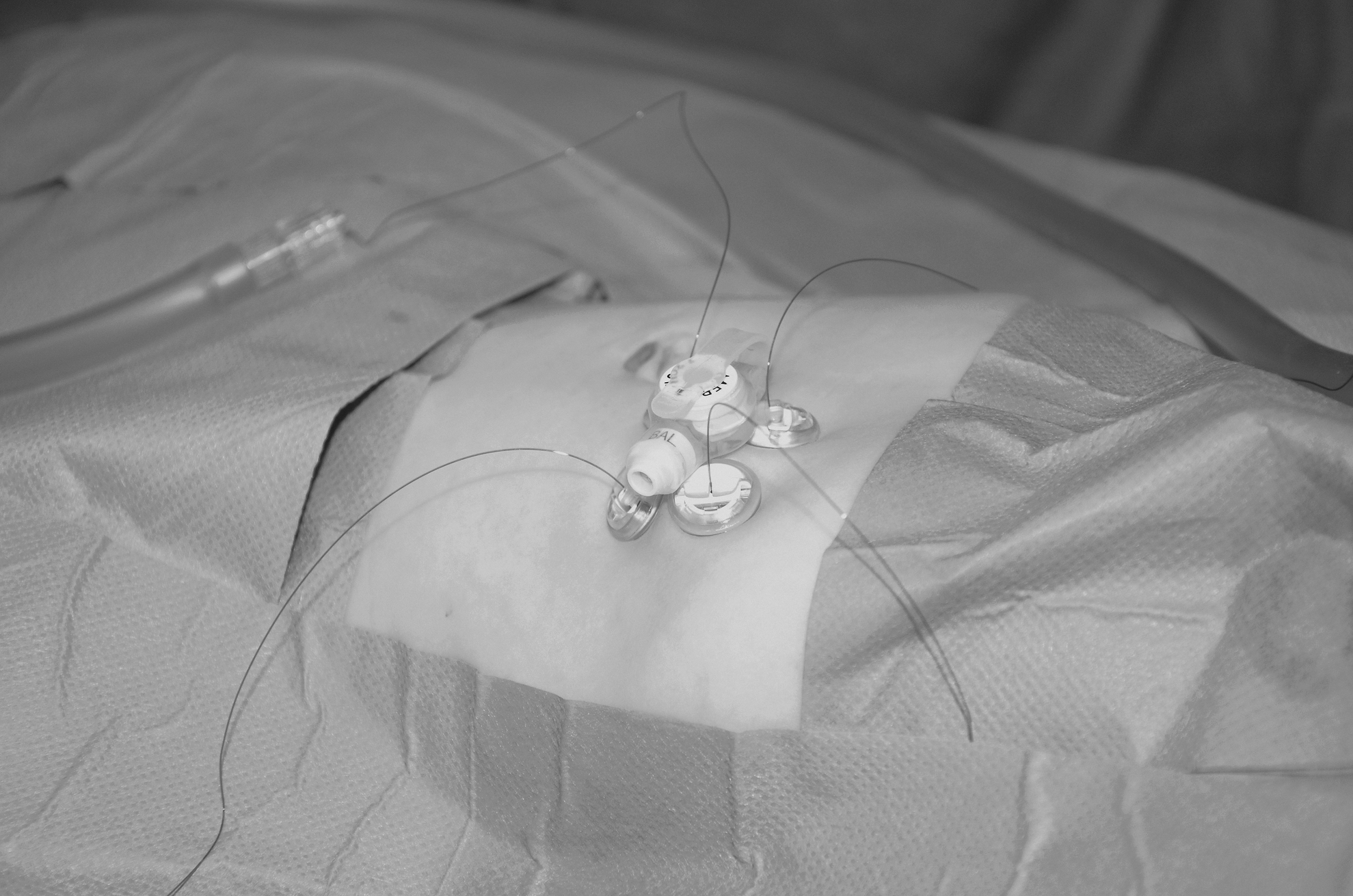
External view on gastropexy using the Saf-T-Pexy system (Halyard Health).
The stomach was filled with air through the preinserted nasogastric tube. The intended site of the gastrostomy tube placement was marked using a skin sterile marker. We marked four points forming four sides of a square and an additional central point that was later used to perform an incision and to position the gastrostomy feeding tube. The points intended for insertion of a Saf-T-Pexy needle were projected on the anterior wall of the stomach, which had previously been filled with air via the nasogastric tube. A single-step puncture of the abdominal wall and the anterior gastric wall was made using the Saf-T-Pexy needle. Once the needle is inserted, the suture at the side of the needle hub is released, the blue safety lock is bent aside, and the obturator is pushed further inside the needle. This allows the T-shaped anchor (T-bar) to leave the needle. This T-anchor is still attached with a resorbable suture. Next, the Saf-T-Pexy needle is removed from the abdomen, and the suture ends with a polyurethane locking mechanism remain outside the abdominal cavity. This puncturing with the Saf-T-Pexy needle is repeated four times to create the square-shaped gastropexy.
Further surgery steps (puncture of the stomach, catheterization, dilatation of the gastric opening, and insertion of the gastrostomy feeding tube into the stomach) corresponded to the earlier described laparoscopic gastrostomy placement using U-stitches. After insufflation of the MIC-KEY internal retention balloon, the four gastropexy T-anchor sutures were gently tightened, and the polyurethane fixation discs were closed. In order to limit postprocedural pain, the sutures may not be fixed too tight; it is recommended that a distance of 2–3 mm be kept between the polyurethane fixation discs and the skin.
In the hours following the laparoscopic procedure the gastrostomy feeding tube was kept open to remove all air from the stomach. For this purpose, the end of the gastrostomy feeding tube was connected to a sterile container in order to collect gastric residue. Feeding via this gastrostomy tube usually commenced a few hours after surgery: a newborn would receive 20 mL of breast milk or formula per saltum; infants, 50 mL; and children over 3 years of age, up to 100–150 mL of liquid enteral formula every 2–3 hours. However, seriously ill and debilitated patients might continuously receive enteral feeding with nutritional formulas and solutions through the enteral feeding pump immediately after surgery (initially at a rate of 1 mL/kg/hour, increasing gradually if well tolerated) with interruptions to control stomach emptying (the gastrostomy tube is open for this purpose). On the second day we shifted to the standard feeding protocol.
U-shaped fixing sutures were not removed until Day 6–7 after surgery. Saf-T-Pexy anchor fixing sutures required no special care as the polydioxanone sutures are resorbable, and the sutures usually break after 2–3 weeks. Monitoring of the child's condition included patients' follow-up visits with the operating surgeon at 2 weeks, 1 month, and 3 months. Within this period any postoperative complications were reported: poor sealing capacity with gastric contents leaking to the outside, local infection, peristomal contact dermatitis, or overgrowth of granulation tissues. Complications usually required no recurrent surgical treatment and were corrected with topical treatment of antibacterial creams and tanning agents. Due to the child's growth, the MIC-KEY gastrostomy feeding tube was replaced every 3 months. The tube was chosen by measuring the stoma length with the stoma measuring device.
Analyses
The patient groups were compared statistically. The preoperative parameters (sex, weight at admission, and age on the day of surgery) were analyzed. The following intra- and postoperative parameters were compared: duration of surgery, start of enteral feeding, shift to full enteral feeding, duration of hospital stay, and postoperative complications. The Mann–Whitney U test was used to assess mean values. The level of confident significance was set as P < .05. Yates's corrected chi-squared test was used to assess categorical variables.
Results
The comparative analysis of patients' data revealed no significant differences in the preoperative parameters of the study groups (Tables 1 and 2). The mean weight of the patients from Group I was 3549.35 g, and that of the patients in Group II was 3326.92 g (P = .632). There was no difference in the groups' sex composition (boys/girls, 70.83%/29.17% versus 50%/50%; P = .238). The mean age of the patients in the laparoscopy group on the day of surgery was 51.21 days, compared with 36.0 days among the infants who underwent open gastrostomy tube insertion (P = .078).
Number of cases is given as n.
By Mann–Whitney U test for level of confident significance.
Group I, laparoscopic U-stitches gastropexy; Group II, laparoscopic Saf-T-Pexy gastropexy; SEM, standard error of mean.
Data are number of cases.
By Yates's corrected chi-square test for level of confident significance.
By Fisher's test for level of confident significance.
ARP, antireflux procedure; Group I, laparoscopic U-stitches gastropexy; Group II, laparoscopic Saf-T-Pexy gastropexy.
The study showed no significant difference in surgery duration (P > .05). The mean surgery duration for the patients in Group I was 23.75 minutes, whereas that for patients in Group II was 22.71 minutes. The same proportion of children in both groups underwent simultaneous laparoscopic Nissen fundoplication (50%).
Postoperative recovery was also consistent in both groups. Enteral feeding after laparoscopic gastrostomy with U-stitches commenced on average within 9.96 hours; this was similar for patients who had undergone gastrostomy using the Saf-T-Pexy system, where feeding commenced within 10.63 hours (P > .05). Full-scale enteral feeding of the infants from Group I was possible within 23.13 hours of the surgery versus within 24.5 hours for the children from Group II (P > .05). Group I patients were discharged from the hospital on average 7.25 days after surgery. Group II patients were hospitalized for 7.21 days. There were no significant differences between the groups (P > .05).
In the early follow-up period after surgery minor complications were reported, which, however, required no recurrent surgical repairs. Postoperative problems were reported in different proportions for the patients, with statistically significant predominance in Group II (41.67% versus 8.33%; P = .036) (Table 2). The main postoperative complications were the development of symptoms of contact dermatitis, overgrowth of granulation tissues, and gastric contents leaking. Topical treatment with antibacterial ointments and coagulating agents helped to halt and reverse the development of minor peristomal problems. Contact dermatitis occurred with significantly higher frequency in the patients who had undergone the gastropexy with U-stitches. Growth of granulation tissues was reported more often in Group I.
The long-term follow-up monitoring for patients in the period from 3 to 24 months revealed no differences in disease outcomes. Respective mortality rates during the long-time follow-up after the surgery were 10% and 11%. However, none of the deaths was associated with the tube placement procedure but was instead caused by serious nervous system disorder. Five children from Group I and seven children from Group II no longer needed a gastrostomy as time passed. Gastric fistulas closed without any intervention; consequently, a surgical fistula closure procedure was not performed. The cosmetic outcome of the laparoscopic gastrostomy was the same in the comparison groups. Hidden in the fold of the umbilical ring, the traces of laparocentesis incision became indiscernible during a routine examination.
Discussion
At present, gastrostomy is routine surgery performed on both adult and pediatric patients. The range of pathologies that require placement of a gastrostomy tube includes serious neurological disorders, swallowing problems, esophageal obstruction, and nutritional disorders caused by underlying cardiovascular, oncological, and metabolic diseases. Gastrostomy was previously performed using the open method of Stamm and Kader as detailed by Murayana et al. 13 The idea of performing gastrostomy without the laparotomy, or PEG, was first proposed in 1980 by Gauderer et al. 4 After three decades of using the PEG procedure, significant numbers of complications were reported.3,5,8,14–16 The majority of these were due to a “blind” stomach puncture and the risk of large and small bowel trauma. Other complications of this procedure, such as peritonitis and the poor sealing capacity of the gastric stoma, were caused by the lack of sufficient stomach fixation to the anterior abdominal wall without internal sutures.
Rothenberg et al., 10 Georgeson,6,7 and Sampson et al. 17 strove to solve the biggest laparoscopy problem of the “blind” puncture that risked causing trauma to internal organs and made it possible to control all intraoperative steps of this procedure, although the number of minor complications remained rather high. The reported frequency of laparoscopy gastrostomy complications (18%–23%) demonstrates the relative safety of endosurgical procedures7,11,18–20 in comparison with the failure level of 25%–40% after use of other mini-aggressive methods of placement of gastrostomy tubes, such as PEG gastrostomy.3,5,8,14–16 Elimination of the serious consequences of an “intuitive” stomach puncture helps to distinguish the scope of new laparoscopy problems, the most frequent of which are peristomal contact dermatitis, poor sealing of the gastrointestinal stoma, and granulation formation.
Peristomal contact dermatitis manifests as redness and tenderness of the skin around the stoma and can be caused by gastric contents leaking outside. Accurate control of the filling of the internal fixation balloon and topical treatment with anti-inflammatory creams containing antibacterial agents are necessary to treat this complication.
Poor sealing placement is associated with gastric contents leaking around the feeding tube. That is the most frequent source of anxiety for patients and their parents. In most cases this phenomenon is associated with the stomach's overfilling with nutritional masses and/or air. The increased risk of gastric contents leaking around the gastrostomy tube is associated with high abdominal pressure against a background of muscular hypertension in patients with neurological disorders.
Granulations are the result of a local reparation process in the gastric stoma region. The area of granulations can increase over time and cause tissue bleeding. If this occurs, chemocautery (using potassium permanganate strong solutions or silver nitrate stick) is recommended. If granulation tissues continue growing and increasing in size, interfering with proper gastrostomy tube handling, an electrical excision of these lesions might become necessary.
Data relating to the onset of these complications and their causes are controversial. The most probable cause of the reported level of failures is a gastropexy method and fixation of a gastrostomy feeding tube. The following methods of fixation of the stomach to the abdominal wall tissues are distinguished: intracorporal (internal purse-string suture), 9 extracorporal (external purse-string suture), 10 and use of anchor U-shaped transparietal sutures.11,12 However, none of them ensures a good sealing capacity of the gastropexy, which further leads to contact dermatitis, an external leakage causing chronic inflammation in the external orifice region, and the formation of granulations. We chose four sutures in the form of a square, for more secure attachment of the gastric and abdominal walls around the gastrostomy tube. As a result, we received a reliable gastropexy that prevented external leakage of contents of a stomach and development of postoperative complications.
Another gastrostomy issue is associated with development of gastroesophageal reflux after placement of a gastrostomy tube. A retrograde flow of gastric content into the esophagus is often described as one complication of this surgery. According to Aprahamian et al., 11 24% of children require a fundoplication after the gastrostomy placement. Opinions about the development of gastroesophageal reflux in patients who underwent the gastrostomy are controversial. The study of Thomson et al. 21 demonstrates the increase of gastroesophageal reflux episodes in children with neurological disorders after the gastrostomy. However, the research of Plantin et al. 22 refutes this statement. The authors believed that the main problem is proper placement of the gastrostomy tube so that it does not provoke a reflux of gastric content into the esophagus. Thus, the proper visually controlled placement of the tube into the stomach prevents the development of gastroesophageal reflux. Our study showed that the discussed methods of gastropexy were not followed by an increased risk of formation of gastroesophageal reflux. The reflux was reported in the same proportion of the children from both groups (1 patient from each group) on average within 3 months of surgery.
Based on the known treatment outcomes, we introduced a new surgical technique for gastrostomy tube fixation. In order to diminish the risk of complications, we applied an innovative gastropexy method using the Saf-T-Pexy anchoring system. This new procedure has special features that helped us to improve postoperative results by decreasing the frequency of complications. These features are as follows:
• use of the laparoscopy providing control over all intraoperative steps, eliminating the risk of trauma to internal organs and vessels • use of four fixing sutures instead of one or two. We find this gastropexy variant the most reliable as it ensures the stomach's adhesion to the abdominal wall around the gastrostomy tube over a larger distance. • preventing trauma to the stomach posterior wall. We always tighten the first stomach's anchor suture to the abdominal wall, which provides an increased lumen of the stomach. Furthermore, the gastrostomy feeding tube placement can be controlled using a “double” endoscopy: the stomach's lumen is examined using the flexible endoscope, and the abdominal cavity is viewed using the laparoscope.
The results of our research demonstrate that gastrostomy with T-shaped anchor sutures can be conducted with fewer complications in comparison with gastrostomy tube placement using the U-stitch anchoring. We obtained the long-term results of this gastropexy method proving that this new procedure could be a promising technique ensuring the stable and reliable fixation of gastrostomy tubes of any type.
Conclusions
The laparoscopic placement of a MIC-KEY balloon type of gastrostomy tube is a preferable method for long-term access to the gastrointestinal tract for enteral feeding. The conclusions obtained in this study demonstrate that laparoscopic gastrostomy in young children can be efficient and safe, as well as significantly improves patients' future growth and development. This new method of gastropexy using the Saf-T-Pexy anchor system is simple and safe and reduces the number of postoperative complications based on stable and firm fixation of the stomach and abdominal wall in the form of a square.
Footnotes
Disclosure Statement
No competing financial interests exist.