
Abstract
Abstract
Background:
There is no consensus for the management of failed laparoscopic pyeloplasty in pediatric surgical patients, and only limited publications are available. We evaluated here the clinical outcomes of re-intervention for failed laparoscopic transperitoneal pyeloplasty in infants and children.
Materials and Methods:
Retrospective review of all children who had undergone laparoscopic transperitoneal dismembered Anderson–Hynes pyeloplasty for ureteropelvic junction obstruction from 2002 to 2013 was performed. Patients' demographics, indications, operative details, and outcomes for primary operation as well as re-intervention were studied.
Results:
There were 42 patients with a median age of 20 months (range, 3–192 months) and a median body weight of 12 kg (range, 6–56 kg) who underwent a total of 46 laparoscopic transperitoneal pyeloplasties during the study period. The median operative time and blood loss were 193 minutes (range, 115–480 minutes) and trace amount (range, trace amount to 400 mL), respectively. No conversion was reported. Ten cases (22%) required re-intervention. No statistically significant risk factor for failed pyeloplasty was identified. Indications for re-intervention included deterioration of differential renal function (n = 6), progressive hydronephrosis (n = 1), urinary ascites (n = 2), and urosepsis (n = 1). Median time of re-intervention was 6.5 ± 38 months postpyeloplasty. Re-intervention was categorized into the redo pyeloplasty group (n = 6) and the urinary diversion group (n = 4) (insertion of double-J ureteral stent or endopyelotomy) with success rates of 50% and 25%, respectively. Among the redo pyeloplasty group, 3 patients underwent redo laparoscopic pyeloplasty, and all of them had drainage restored with a median improvement in differential renal function of 11%. The mean follow-up duration was 77 ± 38 months.
Conclusions:
Laparoscopic transperitoneal pyeloplasty is safe and feasible in children. Redo pyeloplasty is a more favorable re-intervention compared with urinary diversion in our series. Redo laparoscopic pyeloplasty has been shown to improve differential renal function.
Introduction
P
Materials and Methods
A retrospective review of all children who had undergone laparoscopic transperitoneal dismembered Anderson–Hynes pyeloplasty for ureteropelvic junction obstruction from 2002 to 2013 was performed. Patients' demographics, indications for pyeloplasty, operative details and outcomes for the primary operation, type(s) of re-intervention, indication for re-intervention, resolution of obstruction, change in differential renal function, and duration of follow-up were studied. Patients with obstruction of the distal urinary tract or with other nonmechanical causes of renal impairment were excluded.
Operative technique
The patient was positioned supine with the left or right side arched up, and a Foley catheter was inserted. A subumbilical incision was made, and the peritoneum was entered. The splenic flexure was taken down with bipolar diathermy, and the renal pelvis was exposed. A 4/0 polypropylene (Prolene®; Ethicon Inc., a Johnson & Johnson Company, Somerville, NJ) was passed percutaneously to anchor the renal pelvis. The most dependent position of the renal pelvis was identified and opened. The proximal ureter was spatulated across the obstruction, and 5/0 polyglactin 910 (Vicryl®; Ethicon Inc.) was used for pelvic ureteric anastomosis in a continuous fashion. After the posterior wall was anastomosed, a double-J ureteral stent (Boston Scientific, Natick, MA) was inserted depending on the patient's body size. The position of the double-J ureteral stent was confirmed with methylene blue refluxing from the catheter. Postoperatively, the position of the double-J ureteral stent was confirmed by plain X-ray. The Foley catheter was removed on postoperative Day 5, and the patient was discharged on Day 5.
The double-J ureteral stent was removed in 6 weeks. All patients then underwent ultrasound of the urinary system and diuretic scintigraphy using Tc-99m mercaptoacetyltriglycine in 12 weeks. Subsequent follow-up in the pediatric urology clinic was arranged. For those with persistent hydronephrosis, ultrasound of the urinary system was arranged at 3-month intervals. Diuretic scintigraphy was arranged if progressive hydronephrosis was present. Failed pyeloplasty was defined as reduced renal differential function of less than 40%, progressive hydronephrosis, or the presence of symptoms caused by pelvic–ureteric junction obstruction. Re-interventions included cystoscopy with double-J ureteral stent insertion, endopyelotomy, and open/laparoscopoic-assisted/laparoscopic/robotic redo pyeloplasty were chosen according to preferences of the individual surgeon or parents. Success of the re-intervention was defined as drainage evidenced by diuretic scintigraphy of the involved kidney.
Unpaired t test and Pearson's chi-squared test were used for comparative analysis, and univariate analysis was done with the one-way analysis of variance test using SPSS software (version 17.0; SPSS, Inc., Chicago, IL). Statistical significance was defined as P < .05.
Results
Forty-three patients were identified. One patient was excluded due to diagnosis of vesicoureteric junction obstruction following pyeloplasty. Thus, 42 patients underwent a total of 46 laparoscopic transperitoneal pyeloplasty procedures during the study period. The median age was 20 months (range, 3–192 months), and the median body weight was 12 kg (range, 6–56 kg). The median operative time and blood loss were 193 minutes (range, 115–480 minutes) and trace amount (range, trace amount to 400 mL), respectively. No conversion was reported.
Ten (22%) patients required re-intervention. The demographics of the patients, indications, and modality of re-intervention are shown in Table 1. The patients were numbered in chronological order. No statistically significant risk factors for failed pyeloplasty were identified. Indications for re-intervention included deterioration of differential renal function (n = 6), progressive hydronephrosis (n = 1), urinary ascites (n = 2), and urosepsis (n = 1). Median time of re-intervention was 6.5 ± 38 months following pyeloplasty. No crossing vessel was present in any patient. The mean follow-up duration was 77 ± 38 months.
The outcomes of patients are summarized in Figure 1. Re-intervention was categorized into the redo pyeloplasty group (n = 6) and the urinary diversion group, either by insertion of a double-J ureteral stent or endopyelotomy (n = 4). The success rates of the redo pyeloplasty group and the urinary diversion group were 50% and 25%, respectively, as demonstrated in Table 2. Among the redo pyeloplasty group, success was observed in 3 patients undergoing redo laparoscopic pyeloplasty. All of them had drainage restored with a median improvement in differential renal function of 11%. Drainage was also observed in 1 patient who had redo laparoscopic-assisted pyeloplasty. Two patients with unsuccessful outcomes had redo pyeloplasty twice. One patient had open redo pyeloplasty and subsequent redo robotic pyeloplasty, whereas the other patient underwent open redo pyeloplasty twice. The urinary diversion group had a less promising outcome: only 1 patient with endopyelotomy achieved drainage.
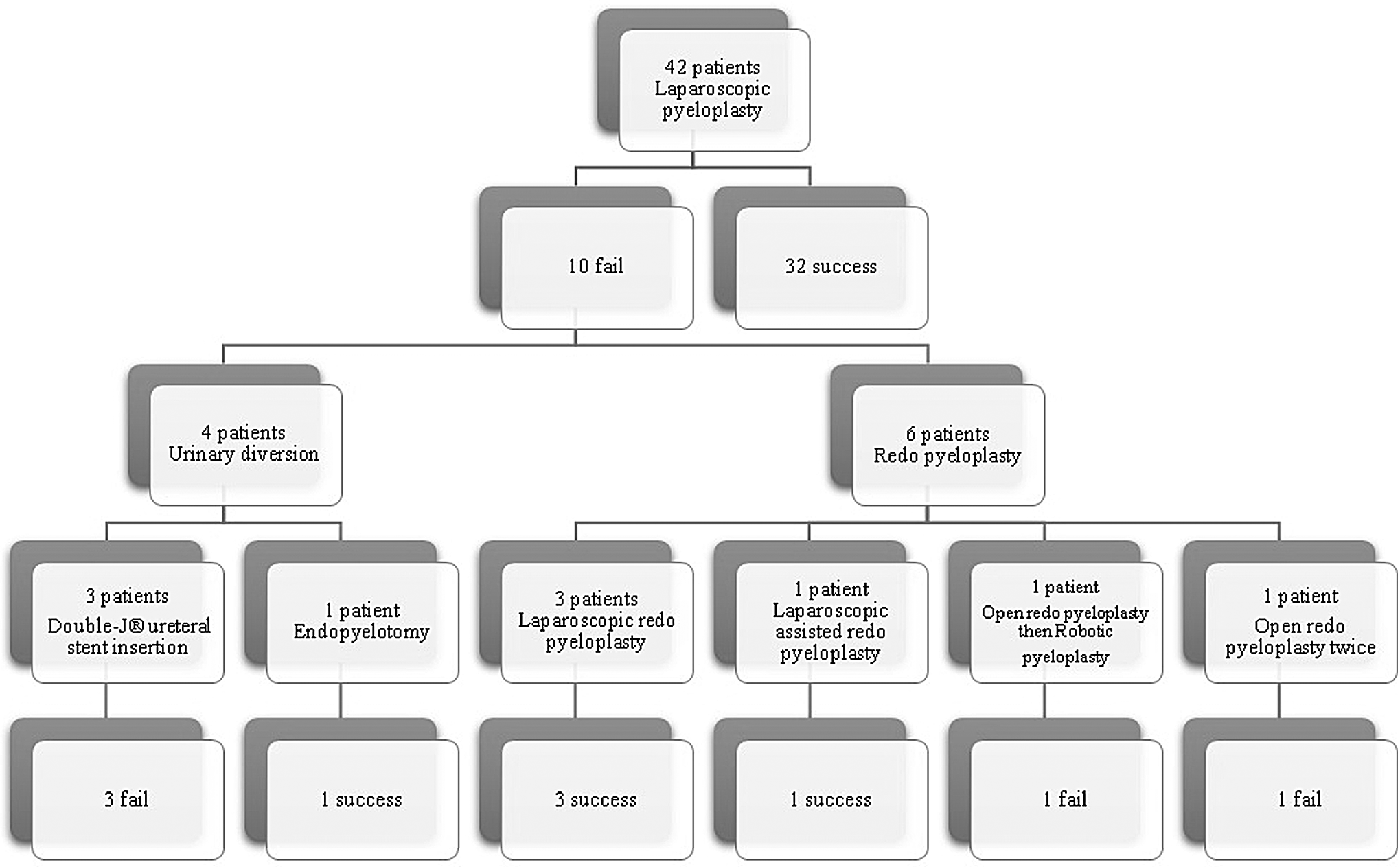
Outcomes of patients who underwent laparoscopic pyeloplasty.
Complications
Complications occurred in 3 re-intervention patients. Patient 3 had the complication of anastomotic leakage from the pyeloplasty site and displacement of the right double-J stent on Day 1. He developed oliguria, urinary ascites, and acute renal failure. Laparoscopic converted to open redo pyeloplasty was done. Three months postoperatively, he was found to have complete obstruction of the right ureteropelvic junction, and a second open redo pyeloplasty was done. Postoperative Tc-99m mercaptoacetyltriglycine scan showed obstruction with renal differential function of 18%. Redo pyeloplasty was offered to the parents.
In Patient 4, open redo pyeloplasty was performed 7 months after the failed pyeloplasty. Extensive fibrosis was noticed intraoperatively. It was complicated with a perinephric abscess, which was treated by intravenous antibiotics. He defaulted reassessment imaging postoperatively and subsequently underwent robotic pyeloplasty 32 weeks later in view of persistent obstruction and a ballotable kidney. Intraoperative findings included a large amount of adhesions around the previous anastomosis, as well as a dilated renal pelvis up to 15 cm, containing more than 500 mL of urine.
Patient 7 developed severe urinary ascites resulting from malposition of the double-J ureteral stent. She required pediatric intensive care unit admission for treatment of hyponatremia and seizure. She underwent cystoscopy on postoperative Day 4, and the ureteric stent was found to have migrated into the dilated renal pelvis. Upon laparotomy, the anastomosis was found to be intact and patent, and there was moderate ureteric narrowing at the pelvic brim level. Open pyelotomy was done, and a new ureteric stent was inserted, with a pigtail nephrostomy being placed temporarily. Cystoscopy and a retrograde pyelogram showed a persistently dilated renal pelvis, and the double-J ureteral stent was exchanged. Diuretic scintigraphy after removal of the double-J ureteral stent showed a gross hydronephrotic right kidney with differential function of 49% and persistent obstruction with a prolonged half-life following furosemide of 173 minutes. Re-insertion of the double-J ureteral stent was performed.
Discussion
Despite a high success rate of pyeloplasty in treating ureteropelvic junction obstruction in children, a small proportion of patients has persistent obstruction. An early study by Persky et al. 17 found scarring and peripelvic fibrosis in patients with failed initial pyeloplasty, which might lead to urinary extravasations and urosepsis. Other studies had identified anatomical findings such as ureteral kink, redundancy of the renal pelvis, and a long ureteral stricture in failed pyeloplasties.9,10 Lim and Walker 9 suggested that prolonged urinary drainage and younger patient age (less than 6 months) might be risk factors for persistent obstruction. In our series no statistically significant risk factor was identified.
Re-interventions for patients with failed pyeloplasty can be classified into the endourologic approach, via pyelotomy or double-J ureteral stent insertion, and redo pyeloplasty. Pyelotomy can be done in an antegrade or retrograde fashion using electrocautery, a cold knife, or a holmium laser. Faerber et al. 8 performed four successful percutaneous antegrade cold knife endopyelotomies on 5 patients who failed open pyeloplasty; the failed patient eventually underwent a successful ureterocalicostomy. The authors concluded endopyelotomy was a minimally invasive alternative to conventional repeat open pyeloplasty.
Veenboer et al. 14 reported a less successful outcome with endopyelotomy. Ten endopyelotomies using electrocautery were performed on patients with failed open/laparoscopic pyeloplasty or ureterocalicostomy. In 10 patients endopyelotomy was done percutaneously, and in 1 patient it was done in a retrograde fashion. The procedure was successful in 70% of the patients. In 4 patients, re-intervention had to be considered. One redo pyeloplasty was performed. The authors concluded endopyelotomy could not be considered as a gold standard.
Braga et al. 11 also reported a lower success rate of retrograde endopyelotomy than redo pyeloplasty in 32 patients with failed pyeloplasty. The retrograde endopyelotomy technique consisted of a holmium laser in 10 patients and cautery/balloon dilation in 8. Retrograde endopyelotomy was successful in 39% of the patients, whereas redo open laparoscopic pyeloplasty had a 100% success rate (P = .002). Only 1 of 8 children (13%) had a successful retrograde endopyelotomy using cautery followed by balloon dilation.
A more recent study by Kim et al. 18 reported a 94% successful rate of endopyelotomy in 35 patients with failed pyeloplasty at a median 5-year follow-up. Perinephric hematoma/urinoma developed in 2 patients, and postoperative ileus occurred in 1; all resolved under conservative management.
Published studies on open redo pyeloplasty had reported success rates of 75%–100%.9–11,13 Lim and Walker 9 reported a salvage rate of 75% by repeat open pyeloplasty on 10 patients. Six patients who had recurrent ureteropelvic junction obstruction were younger than 6 months at the time of the original pyeloplasty. A strong association between a crossing vessel and ultimate failure was observed. A 100% success rate by redo open pyeloplasty had been reported in the comparative analysis of Braga et al. 11 Thomas et al. 10 also reported a favorable outcome with redo open pyeloplasty; 6 failed cases had a 100% success rate with little postoperative morbidity. Only 1 patient underwent endopyelotomy after a failed balloon dilation, which eventually failed and had to be redone with a pyeloplasty. Helmy et al. 13 also shared their experience on redo open pyeloplasty in 14 patients with a salvage rate of 89% and excellent functional results.
There are limited published data on laparoscopic redo pyeloplasty in the pediatric population. Success rates reported in adults ranged from 75% to 92%.19–21 Piaggio et al. 12 compared laparoscopic with open redo pyeloplasty in 10 patients and reported an 80% success rate in each group.
The newer technique of robotic surgery facilitated dissection, intracorporeal suturing, and knot tying. Lindgren et al. 15 performed redo robotic-assisted laparoscopy in 13 patients and redo robotic-assisted laparoscopic ureterocalycostomy in 3. The mean age of the patients was 6 years. Thirteen of the 16 patients had a history of other interventions after the initial failed pyeloplasty, including endopyelotomy with stent placement, percutaneous nephrostomy, and stent placement with or without balloon dilation. Improved radiological findings were seen in 88%. One patient underwent transfusion and conversion to an open procedure due to bleeding. Hemal et al. 22 reported successful robotic-assisted laparoscopic redo pyeloplasty in nine adolescents and young adults.
In a recently published series on 27 failed pyeloplasties by Romao et al., 16 therapeutic procedures were offered at the discretion of the attending surgeon, which included cystoscopy with double-J ureteral stent insertion, endoscopic endopyelotomy, open or laparoscopic redo pyeloplasty, and ureterocalicostomy. The authors found that more invasive and definitive techniques, such as redo pyeloplasty and ureterocalicostomy, were more successful than minimally invasive ones.
Our series also demonstrated redo pyeloplasty to be more favorable compared with urinary diversion. One of the limitations of our study was that the re-intervention procedure was chosen according to preferences of the individual surgeon or the parents. In our urinary diversion group, Patients 9 and 10 had double-J ureteral stent insertion in view of equivocal drainage following initial pyeloplasty. Both had regular ultrasound reassessments, and the double-J ureteral stent was changed at 6–8-week intervals. In Patient 1, open redo pyeloplasety was unsuccessful due to dense fibrosis, and thus endopyelotomy was performed. Management of Patient 7 has been discussed in detail in Results. The unsuccessful outcome of open and robotic pyeloplasty in Patients 3 and 4 could be explained by the complications mentioned earlier. Another limitation of our study was the small number and heterogeneity of the re-intervention group.
Our series, when compared with the very few published on laparoscopic redo pyeloplasty in children, 12 demonstrated a reasonably satisfactory outcome. A possible explanation might include an increased laparoscopic experience resulting from the larger number of laparoscopic pyeloplasties in our center compared with other techniques. Our study did not demonstrate a benefit of earlier re-intervention as the interval to re-intervention was the longest in our laparoscopic subgroup, compared with other modalities.
We would like to make the following recommendations from our experience on laparoscopic pyeloplasty. A suitable size of double-J ureteral stent was first prepared according to the body measurements made before the operation was started. A double-J ureteral stent with inadequate length might lead to the detrimental consequence of migration and coiling inside the dilated renal pelvis, whereas an excessively long catheter would lead to easy slipping via the urethra. We found that it was easier to identify a dilated renal pelvis and thus insertion of the double-J ureteral stent was usually performed during anastomosis after mobilization. A correctly placed double-J ureteral stent was essential to facilitate postoperative drainage and to prevent the complication of leakage; methylene blue was injected via a Foley catheter, and furthermore fluoroscopy was used intraoperatively to confirm the position of the two ends of the catheter. A plain X-ray was performed postoperatively to ascertain the position of the double-J ureteral stent after removal of the Foley catheter, before discharge of the patients.
Conclusions
Laparoscopic transperitoneal pyeloplasty is safe and feasible in children. Redo pyeloplasty is a more favorable re-intervention compared with urinary diversion in our series. Redo laparoscopic pyeloplasty has been shown to improve differential renal function.
Footnotes
Disclosure Statement
No competing financial interests exist.