
Abstract
Abstract
Background:
Various surgical small intestinal anastomosis methods are in current use, but improvements are always desired. Thus, we compared the feasibility, effectiveness, and safety of a new high-frequency electric welding (HFEW) system for sealing the small bowel versus a hand-sewn in vivo pig model.
Materials and Methods:
The 96 bowel segments of three pigs were randomized to be sutured either by the HFEW-300 PATONMED device (E.O. Paton Electric Welding Institute of the National Academy of Sciences of Ukraine, Kiev, Ukraine) or hand-sewn, and mucosa-to-mucosa fusions were subjected in vivo testing in the pigs. Bursting pressures, suture time, thermal damage, and the temperature of sealed ends were measured.
Results:
Segments that had been treated with a hand-sutured ligature or double-sealed with HFEW were compared. Burst pressure was significantly higher in the hand-sutured group than in the HFEW group (136.2 mm Hg versus 75.8 mm Hg, P<.01). All 48 pig small bowels closed by the HFEW-300 generator showed a success rate of 100.0%. The closing time in the HFEW group was significantly shorter (P<.01). The pathological changes of the closed ends were mainly presented as acute thermal- and pressure-induced injuries.
Conclusions:
Outcomes of the current in vivo study suggest that HFEW is an effective and safe method for ligation of the small bowel in pigs.
Introduction
I
High-frequency electric welding (HFEW) is a novel surgical sealing technology for tissues. HFEW uses a bipolar electrosurgical device that produces diathermy between tightly pressed tissues. The high-frequency electric current can be adjusted to act on target tissues, resulting in structural changes to form a common protein space. The sealed intestine is replaced with sound tissue due to fast regeneration processes. Thus, HFEW induces local thermal tissue damage at target tissues only, without damaging adjacent tissues or causing major inflammatory responses. 4 In the Ukraine, HFEW of live soft tissues has been applied widely as a new type of surgical technology in many surgical fields. There are reports that HFEW is clinically available for breast surgery, endocrine surgery, and gastrointestinal resection in the Ukraine.5,6 Although this technique has many advantages, it has not been applied in sealing the small bowel.
The aim of this study is to evaluate the feasibility and effectiveness of an HFEW device (HFEW-300 PATONMED), developed by the E.O. Paton Electric Welding Institute of the Ukrainian National Academy of Sciences (Kiev, Ukraine). Its features regarding burst pressure and histopathological examination in sealing and entero-entero ligation of the small bowel were compared with those of a hand-sewn in vivo pig model.
Materials and Methods
This study was approved by the Institutional Animal Care and Use Committee of Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, China. Three female adult pigs weighing 48.5 kg, 49.2 kg, and 50.3 kg were maintained in individual cages and received water and food ad libitum. After a 14-day adaptation period, food but not water was withdrawn 12 hours before the start of the experiment. The pigs were premedicated with xylazine hydrochloride injection (Military Veterinary Institute, Quartermaster University, Changchun, Jilin, China) (0.1 mL/kg, intramuscularly). Anesthesia was induced with pentobarbital sodium (0.2 mL/kg, intravenously) and maintained with propofol after intubation. Physiological saline (0.9% wt/vol) was infused intravenously at 9.0 mL/kg/hour to maintain homeostasis.
Surgical procedure
After laparotomy, 12 15.0-cm small bowel portions were randomized to be treated with the HFEW-300 PATONMED generator or by hand suture. Hand suture was performed with 2-0 layers of silk in the way of full-thickness continuous suture mucosa-to-mucosa with black silk suture (Johnson and Johnson, New Brunswick, NJ). HFEW was performed with mucosa-to-mucosa fusion single sealing and the HFEW-300 device. 7 The sealed end of each small bowel segment was tested in vivo via a catheter inserted into the unsealed end, which was tightly ligated with 4-0 silk (Fig. 1). The catheter was connected to a syringe pump and a pressure recorder (a hand-held digital manometer [model AZ82100]; AZ® Instrument Corp., Taichung City, Taiwan) via a T-branch connector. A slow continuous infusion (5.0 mL/min) of colored saline was passed through the T-branch connector (Fig. 2). Intraluminal pressure was continuously recorded by a pressure recorder during infusion, and readings were stored for later offline analysis. After surgical sealing, the proximal sealed end of the small bowel was sent for histological evaluation, and the distal end was used immediately to measure bursting pressure. The maximum temperature of the welded intestine was analyzed continuously during sealing. Small bowel segments were considered defective if they failed to hold saline at the beginning of the infusion or showed leakage from the sealed end. Burst pressure was defined as pressure at the point when saline was initially observed from the sealed end and confirmed by visual inspection. The area of small bowel failure was noted.

Pig small intestine after welding.

Connecting device for measuring pressure.
Equipment
The medical electrical equipment HFEW-300 PATONMED is a high-frequency electrosurgical system designed to perform surgical operations, such as welding of soft live biological tissues using high-frequency currents.
Time to close the small bowel by the welding device and hand suture
Ninety-six pig small bowel portions were randomized to either the experimental group (welding) group or the control (hand-sutured) group, and each group included 48 intestinal samples. In the experimental group, small bowel closure was done using the automatic mode of the HFEW-300 PATONMED device. The automatic welding process begins with a pulse current of 440 kHz to test such physical parameters as impedance among tissues and tissue types, followed by setting the appropriate welding power and welding time in accordance with the results of the test. The current frequency of welding usually reaches 440 kHz or 66 kHz. Time to close the small bowel was defined as the total time required for complete closure of the intestine, as measured by an electronic stopwatch. In the control group, closure was performed by the traditional hand-sutured method operated by one surgeon.
Welding organization temperature and thermal damage
During sealing, in situ dynamic thermography was performed with a thermal infrared imaging camera (model NEC AVIO TVS-500EX; Shanghai Huifeng Electronic Technology Company Ltd., Shanghai, China); recordings were continuous during sealing and were stored for later analysis. The highest temperature measured by the thermal infrared imager during the process of closing the small bowel was defined as the maximum temperature for the sealed end of the intestine. After completing the closure, we used an optical microscope to determine the extent of pathological thermal damage—a measure of the damaged area extending from the welding line to its injured vicinity.
Burst pressure measurement
Burst pressure of the intestinal seal was assessed immediately after closure of the small bowel in both groups. Burst pressure was measured using an infusion device (model SY-1200 single syringe pump; Smiths Medical, Beijing, China). The unsealed end of the harvested intestine was secured to one side of the T-branch pipe and connected to an infusion pump and a pressure recorder via a pressure conversion device. Gas was infused into the intestine lumen at a stable speed (10.0 mL/minute), and intraluminal pressure was continuously recorded.
Burst pressure was defined as the pressure when gas leakage was initially observed from the intestinal seal. A successful closure was defined as burst pressure greater than 15.4 mm Hg,8,9 the highest pressure exerted in the human intestine. Successful rate of closure was defined as the ratio of successful closures to total closures.
Pathological examination
Specimens for pathological examination were obtained by cutting bowel tissue a distance of 1.0 cm from the sealed end, fixing samples in formaldehyde buffer solution, embedding in paraffin, generating sections, and later staining with hematoxylin–eosin dye. Slides were analyzed to assess involution and pathological changes tissue.
Statistical analysis
Data are presented as mean±standard deviation values. Differences between groups were analyzed with Student's t test using SPSS version 13.0 statistical software (SPSS, Inc., Chicago, IL), and statistical significance was set at P<.05.
Results
Feasibility of closing the small bowel with the HFEW-300 PATONMED
The success rate of intestinal closure in the 48 small bowels in the experimental group was 100.0%. The results of closure are shown in Table 1. The minimum and maximum durations of closure were 63.0 seconds and 196.0 seconds (108.8±30.8 seconds), respectively. The minimum and maximum time of thermal damage extent and temperature on closure were 3.2 mm and 5.4 mm (4.4±0.6 mm) and 71.9°C and 91.4°C (85.9±9.1°C), respectively. According to the coefficient of variance of closure, thermal damage extent, and temperature on closing, we found that the degree of variation was greatest for temperature on closing, whereas it was smallest for duration of closure.
CV, coefficient of variance.
Comparison between the experimental and control groups
The results of duration of closure and burst pressure in both groups are given in Table 2. Burst pressure in the experimental group was significantly lower than the pressure obtained in the control group (75.8±19.5 mm Hg versus 136.2±36.7 mm Hg, P<.01). Moreover, the duration of intestinal closure in the experimental group was significantly shorter than in the control group (108.8±30.8 seconds versus 285.1±52.2 seconds, P<.01). No significant difference in the diameter of the small bowel was found between the two groups.
Data are mean±standard error values.
NS, not statistically significant.
Temperature measurement with the HFEW-300 PATONMED
In the experimental group, the highest welding temperature ranged from 71.9°C to 91.4°C, with a mean temperature of 85.9°C. A thermal infrared image following the closure procedure in pig small bowel is shown in Figure 3a. Using the HFEW-300 generator in a welding area of 3.0 cm, the highest temperature reached ranged from 29.7°C to 88.4°C (mean, 37.5°C). The mean temperature of the welding area was 72.2°C. Furthermore, Figure 3b illustrates the temperature measurement using a thermal infrared imager. Temperature of the welding organization changed with time, initially rising and reaching a peak at about 4.5 seconds and then falling over time.

Temperature measurement by using the thermal infrared imager.
Degree of thermal damage during small bowel closure with the HFEW-300 PATONMED
Using an optical microscope, the pathological changes observed at the closed ends were mainly acute thermal- and pressure-induced injuries. The results of HE staining of the two layers of small bowel mucosa that were tightly welded by the HFEW-300 PATONMED device are shown in Figure 4. Pathological changes of the sealed ends mainly presented as albuminous degeneration and coagulative necrosis; however, two layers of small bowel mucosa within the welding area were tightly closed.
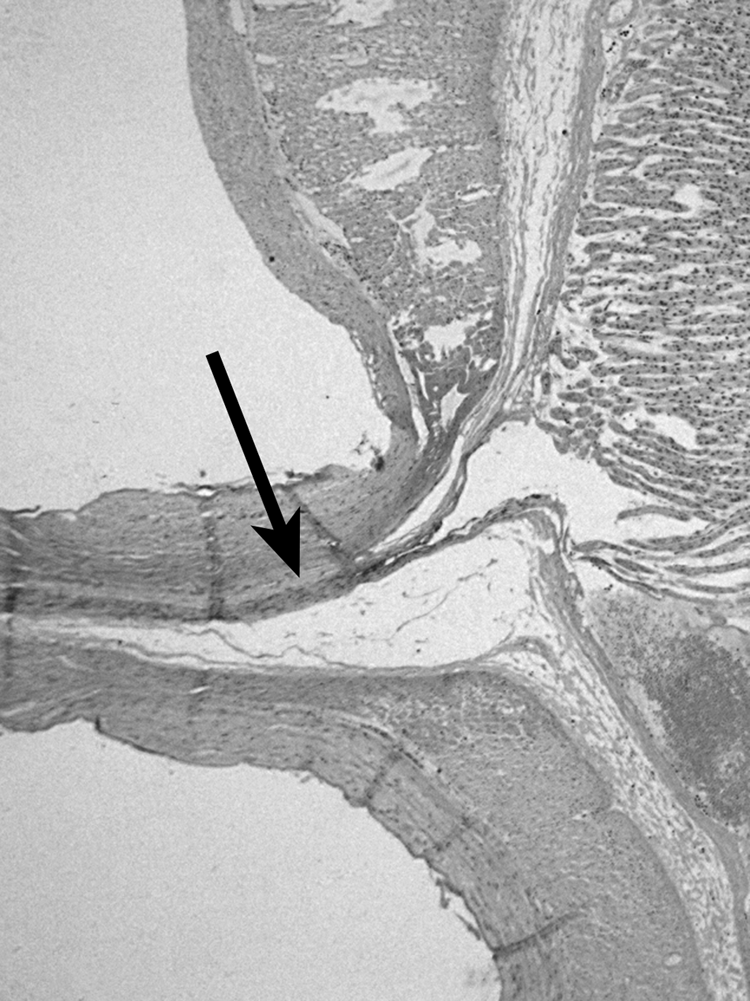
Histological examination of the sealed structure (original magnification ×40).
Discussion
With the development of surgical technology, a series of advanced anastomosis modalities are applied in clinical settings, including the use of mechanical compression devices, adhesives, and tissue fusion by heat. Therefore, the possibility of fusing biological tissue using sealing devices that incorporate bipolar energy and mechanical compression is desirable and warrants further exploration.10,11
HFEW of soft tissues is an innovative and advanced application for intestinal closure and offers tight temperature control generated from high-frequency electronic current. 4 The HFEW-300 PATONMED generator is a novel energy-delivering bipolar electric surgical device based on HFEW of a live soft tissue technology. The present study was designed to evaluate the feasibility and efficacy of using the HFEW-300 device for sealing the small bowel accomplished through bowel mucosa-to-mucosa anastomosis. We compared this technique with the conventional hand-sewn procedure in an experimental in vivo pig model. With this in mind, we analyzed bursting pressures, suture time, thermal damage, the temperature of sealed ends of these ligation techniques, and their physical and histological characteristics. In this study, the working principle of HFEW is that it can destroy the secretion function of glandular structures in mucous layers, achieving anastomosis of two bowel ends through intercellular adhesion proteins. That is why we chose mucosa-to-mucosa closure with suture or welding and opted for a control group with mucosa-to-mucosa suture closure with black silk. We used 2-0 layers of silk with full-thickness continuous suture because it is commonly used for anastomosis in China. In future experiments, we plan to study seromuscle-to-seromuscle intestinal closure with HFEW and will add serosa–smooth muscle sutures when the strength of full-thickness suture is not sufficient.
Due to the success in welding small vessels with a laser, as performed by Huang et al., 12 there are multiple ongoing related animal experiments and clinical trials. The technology of laser welding is applied to such tissues as small nerves, bile ducts, intestines, and skin specimen.13,14 However, the difficulty in controlling the temperature of welding leads to lots of shortcomings, including that it is easier to produce burn injuries in soft tissues, as well as lack of repair of injured intestine because the laser can only affect the intercellular protein. According to a previous study 13 showing there is correlation between laser wavelength and absorption of hemoglobin or coagulation zone for safe vaporization, so there is correlation between laser wavelength (intensity) and degree of surgical anastomosis effect. Therefore, more feasibility results are needed before the laser-medium welding technology can be used in practice.
In general, there exists some gas in the intestine of a normal person to keep the intraluminal pressure under a stable level ranging from 6.2 to 7.7 mm Hg. Fink 8 showed that the basal pressure in the ileum of a normal person is 6.9 mm Hg, with the highest peak pressure being less than 50.0 mm Hg. 9 In our study the burst pressure of the experimental group was less than the control group. The significant advantage in the amount of the burst pressure over the peak pressure of the small bowel in a normal person greatly ensures the quality of anastomosis. So although the HFEW anastomoses were significantly weaker than the hand-sewn anastomoses, the burst pressure of HFEW is strong enough to withstand the highest peak pressure in the human intestine.
The comparison between the two groups shows the benefits of the welding device in shortening the duration of ligature of the intestine, simplifying some surgical operations. Santini et al. 7 used the LigaSure™ (Covidien, Norwalk, CT) vascular closing system and a linear cutting closing device to close pig small bowels, with the burst pressure measured as 74.1±5.5 mm Hg and 75.8±5.9 mm Hg, respectively. With the use of the cutting closer assisted with the endoscope by Sodergren et al., 15 the tested burst pressure ranged from 22.0 to 70.0 mm Hg, and the median reached 37.5 mm Hg. 13 Arnold and Shikora 16 performed another experiment in which two groups, one of which added a layer of biological protein glue after the closure, whereas the other one was done with simply closure, were compared with a linear cutting closer. The burst pressures measured were 125.0±24.0 mm Hg and 58.4±28.0 mm Hg, respectively. In this article, the burst pressure shows a great advantage by 75.8±19.5 mm Hg in comparison with the experimental data mentioned above.
Moreover, the duration of the closure in the experimental group is shorter than in the control group. In this study, we used the welding-1 automatic welding mode of the HFEW-300 device in operation. First, the welding-1 automatic welding mode instantaneously detects electrical impedance and other physical parameters in the soft tissue at 440 kHz, and then the device sets the appropriate welding power and time automatically in order to achieve the best effect of welding; the frequency of the device is generally between 66 and 440 kHz when welding is done. Due to the efficient operation of the program and the automatic control program of the HFEW-300 generator, its speed of closing the intestine is much faster. In addition, the intestine diameter of our animal model (Tibetian pig) is slightly smaller than that of normal Chinese adults and is much smaller than those of European and American adults. Also, in this study we used 2-0 layers of silk with full-thickness continuous suture, and we did not add seromuscle-to- seromuscle suture. As well, the suture operator is a surgical attending doctor who is familiar with the clinical gastrointestinal anastomosis, so the suture time is much shorter.
A variety of energy devices could simplify the process of surgery and to some extent reduce thermal damage to tissue. In the research undertaken by Landman et al., 17 it was reported that a bipolar electric knife generates a thermal damage of 2.0–6.0 mm. Meanwhile, Campbell et al. 18 found the average thermal damage owing to LigaSure extends to 4.4 mm. The experimental group in this article shows an average thermal damage of 4.4±0.6 mm (3.2–5.4 mm). The average thermal damage in our experimental group is lower than in the control group. A comparison analysis of the thermal damage among three vascular closing devices conducted by Kim et al. 19 came to the conclusion that the Harmonic® ACE® shears (Ethicon Endo-Surgery, Cincinnati, OH) generated the highest temperature (195.9±14.5°C), whereas the highest temperature of the LigaSure was 96.4±4.1°C, and that of the plasma trisector was 87.0±2.2°C. The experimental group in this article demonstrated the highest temperature ranging from 71.9°C to 91.4°C, with an average of 85.9°C, indicating a lower working temperature of the high-frequency welding device than any of the other three mentioned above. As we know, protein seems to become denatured with a temperature of 80.0°C; when the temperature rises to 100.0°C, cells turn to necrosis. Thus the data of this experiment indicate feasibility and effectiveness of ligature for the small bowel with the high-frequency welding device.
Limitations of this study include the fact that we only compared the clinical effectiveness of HFEW with a hand-suture technique (the gold standard for suturing the small bowel). Furthermore, we did not assess the short-term prognosis of intestinal closure with HFEW, as well as the impact on adjacent tissue. We propose further comparisons should be made between HFEW and the stapler method and that short-term prognosis should be addressed in additional studies. We assessed two methods of mechanical safety of this intestinal anastomosis modality in the same manner. It seems possible to consider that the results of our study remain valid because our research provides a good foundation for further animal study or clinical trials of the HFEW device. Postoperative follow-up results are needed to verify our findings.
Conclusions
HFEW safely and effectively seals and divides the small bowel. This is an important step towards the development of a new bipolar radiofrequency-induced anastomotic laparoscopic instrument combining dissecting and reconstructive properties within one single modality. HFEW may replace or be used in addition to the traditional hand suture and stapler technique.
Footnotes
Acknowledgments
This study was supported by the Science and Technology Planning Project of Guangzhou (grant 201508030035), the Strategic Emerging Industry Core Technology Research Projects of Guangdong Province (grant 2011A081402004), and the National College Student Innovative Entrepreneurial Training Program of 2013 (grant 1212113012).
Disclosure Statement
No competing financial interests exist.
Z.L., Z.H., and J.C. conceived the project. H.Z. and D.H. designed the study. P.Z. analyzed the data. S.H. drafted the manuscript. Z.C., X.N., and L.H. revised the manuscript.