
Abstract
Abstract
Background:
Laparoscopic pyloromyotomy (LP) is a well-established approach for treating hypertrophic pyloric stenosis. Although grasping the pylorus with forceps is important in LP, it requires a high level of surgical skill. To make this approach easier, in 2008 we introduced the method of Dozier and Kim, in which a vascular clamp (VC) is used for grasping the pylorus (LP with VC). Here, we retrospectively compared results between traditional LP (TLP) and LP with VC.
Materials and Methods:
Forty-three patients underwent LP with VC, whereas 194 patients underwent TLP. Two ports in the umbilicus and the left flank are common in both procedures. Instead of a right flank port, however, in LP with VC, we directly insert a VC to grasp the pylorus.
Results:
Patients' characteristics were not different between the two groups. There was only one wound infection and no major complication associated with LP with VC, whereas there were three major complications in TLP. Our hospital is a pediatric teaching institution in Japan where many surgeons perform their first LP. Twenty-eight surgeons performed their first LP in our hospital in the past 17 years, and LP with VC was the first LP for nine. The operative time for surgeons' first LP was significantly shorter with LP with VC than with TLP, based on Welch's t test (42.8 versus 54.4 minutes; P = .048).
Conclusions:
Our results suggest that LP with VC is an easy and safe technique, and it is recommended for beginners in laparoscopic surgery.
Introduction
T
Materials and Methods
The medical records of all patients who underwent pyloromyotomy for HPS at Saitama Children's Medical Center (Saitama, Japan) between July 1997 and September 2014 (n = 247) were reviewed retrospectively. The study protocol was approved by the ethics committee of the Saitama Children's Medical Center and conforms to the provisions of the Declaration of Helsinki.
We compared intraoperative and early postoperative results between patients treated with TLP and LP with VC.
TLP was performed as follows: with the patient under general anesthesia, a 5-mm trocar was introduced through the umbilicus using an open technique. Carbon dioxide was used to insufflate the abdominal space, and intraabdominal pressure was maintained at 8 mm Hg. Two 3-mm trocars were inserted into each upper quadrant of the abdomen. We used forceps (an atraumatic laparoscopic grasper) to grasp the pylorus with the left hand and a knife and spreader to cut and spread it with the right hand.
For LP with VC, the procedure was the same as that for TLP, except for the left-hand port. Instead of the left-hand port, we directly inserted a neonatal VC (Fig. 1) (V. Mueller® Cooley neonatal VC; CareFusion, McGaw Park, IL) through a 3-mm incision to grasp the pylorus under laparoscopic vision (Fig. 2). This technique facilitates changing the direction and position of the pylorus and bringing it into clear view away from the draping liver. The pylorus was grasped during the operation. Finally, in both procedures, we checked mucosal perforation by intragastric injection of air. The right upper quadrant incision remained unaltered during the operation (length, 3 mm).
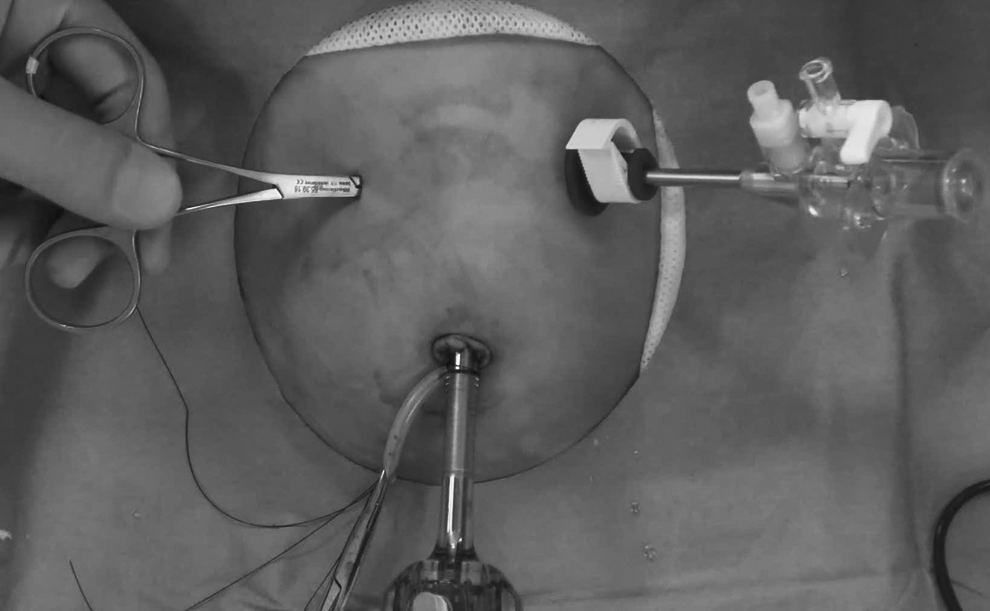
Port design. A 5-mm trocar was introduced through the umbilicus, and a 3-mm trocar was introduced into the left upper quadrant of the abdomen. The vascular clamp was inserted into the right upper quadrant of the abdomen. The hinge of the clamp fits in the level of the abdominal wall.
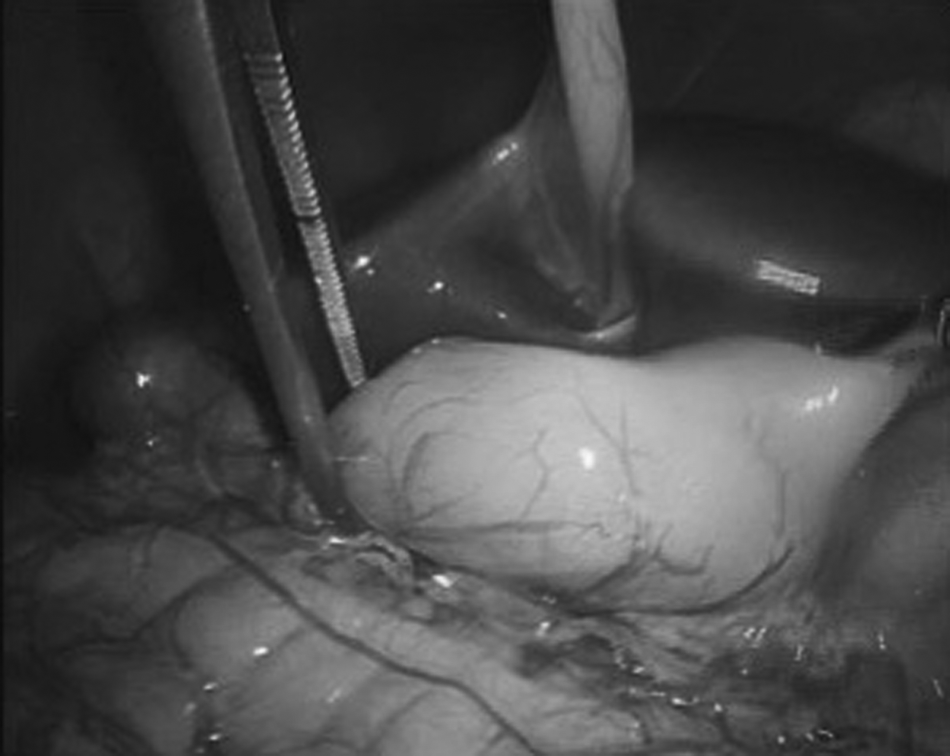
The whole pylorus is grasped using the vascular clamp.
Statistics
The chi-squared test, Student's t test, Fisher's exact test, and Welch's t test were used to compare clinical data between the TLP group and the LP with VC group. Values of P < .05 were considered statistically significant.
Results
Demographic data, including age and body weight at the time of operation, are shown in Table 1. Forty-three patients (36 males, 7 females) underwent LP with VC between April 2008 and September 2014, whereas 194 patients (156 males, 38 females) underwent TLP between July 1997 and March 2008.
Traditional laparoscopic pyloromyotomy (TLP) was performed from July 1997 to March 2008. Laparoscopic pyloromyotomy with vascular clamp (LP with VC) was performed from April 2008 to September 2014. The age and weight of patients treated with LP with VC did not differ from those of patients treated with TLP (P = .50 and P = .15, respectively).
Age and body weight at LP with VC ranged from 16 to 81 days (median, 38 days) and 2.5 to 5.3 kg (median, 3.5 kg), respectively, with no significant differences between groups (P = .50 and P = .15, respectively).
There was only one complication associated with LP with VC, which was a wound infection, and no major complication. “Major complications” were unsuccessful procedures and complications that needed immediate intervention, such as incomplete pyloromyotomy, mucosal perforation, and duodenal injury. The major complication rate was lower for LP with VC than for TLP (n = 0 versus n = 3; P = 1.0), although this difference was nonsignificant (Table 2). “Other complications” were wound infections (3 cases in the TLP group, 1 case in the LP with VC group) and incisional hernia (1 case in the TLP group).
Major complications included incomplete pyloromyotomy, mucosal perforation, and duodenal injury. The major complication rate was lower for laparoscopic pyloromyotomy with vascular clamp (LP with VC) than for traditional laparoscopic pyloromyotomy (TLP), although this difference was nonsignificant.
Fisher's exact test was used to compare the clinical data between the two groups.
In the TLP group, incisional drainage was needed to treat the wound infection in 1 case, and operative treatment was needed for the incisional hernia. Conservative treatment was successful for the other cases of other complications.
Postoperative length of stay was not significantly different between groups (4.46 days versus 4.08 days; P = .24).
Operative time is shown in Table 3. Twenty-eight surgeons performed their first career LP at our hospital in the past 17 years, and LP with VC was the first LP for nine surgeons. Although these surgeons had years of surgical experience, almost all started training in pediatric endoscopic surgery at our institution. The overall operative times for LP with VC and TLP were 43.9 and 40.3 minutes, respectively (P = .17). However, the operative time for surgeons' first LP was significantly shorter for LP with VC than for TLP, based on Welch's t test (42.8 versus 54.4 minutes, respectively; P = .048).
In calculating average postoperative length of stay, hospitalization for other conditions such as cerebromalacia, hypoplastic left heart syndrome, and chronic lung disease were excluded.
LP, laparoscopic pyloromyotomy; LP with VC, laparoscopic pyloromyotomy with vascular clamp; TLP, traditional laparoscopic pyloromyotomy.
Discussion
Extramucosal pyloromyotomy is the standard procedure for treating HPS. 1 In 1912, Ramstedt 6 described his technique for pyloromyotomy. After that, other approaches have been reported. With the development of surgical techniques, minimally invasive surgery (e.g., video-assisted surgery) is increasingly accepted in pediatric surgery. Initially, the approach for conventional pyloromyotomy was through a transverse right upper quadrant incision, which provides a good view of the pylorus. However, this incision does not have a good cosmetic appearance, and over time, the scar often increases in length and breadth as the patient matures. 7 Later, an approach through the umbilicus (circumumbilical incision) was introduced. Although the umbilical incision provides good cosmetic results, the visual field of the pylorus is not ideal, which can be associated with problems with pylorus delivery that necessitate further manipulation of the stomach followed by longer gastric atony. 8 Moreover, this incision has a higher infection rate than the conventional incision.9,10 Additionally, one study suggested that patients with an umbilical incision might experience more postoperative pain. 11
Another approach for minimally invasive surgery was the laparoscopic approach. TLP was first reported by Alain et al. 2 in 1991. After that report, TLP gained favor and became the preferred approach. A prospective, randomized trial comparing open versus laparoscopic pyloromyotomy was reported. 12 This trial showed that there was no difference between the open group and the TLP group in terms of operating time or recovery period. On the other hand, the TLP group required significantly fewer doses of analgesia than did the open group. In another meta-analysis, however, the TLP group was reported to have an increased risk of tearing or perforating the duodenum. 3 Therefore, the only merits of TLP may be its more favorable cosmetic results and less postoperative pain.
In our institute, we had an experience in which grasping forceps with the left hand crushed and perforated the duodenum. Grasping the pylorus with forceps in the left hand is important in TLP but requires high-level surgical skill. Teaching new surgeons to handle the forceps is arduous. It has been reported that TLP has a steep learning curve, especially for the first 15 cases, and decreased operative times were seen with increased experience. 13 Additionally, some reports showed that the occurrence of complications increased when the operation was performed by a general surgery resident in a teaching hospital.14,15
Recently, single-incision LP was described. 7 However, increased numbers of perforations were noted on the initial analysis of single-incision LP, and this method requires a “cross-handed” technique,7,16 which is very difficult for beginners of endoscopic surgery.
In Asia, the use of intravenous or oral atropine treatment is currently widespread. 1 Operations have been replaced by atropine therapy, and the number of HPS operations is decreasing. This trend is the same in our institution. In the past, we performed TLP at a rate of about 18 cases/year and LP with VC at a rate of about 6.6 cases/year. Moreover, because our hospital is the teaching institution of pediatric surgery in Japan, many surgeons perform their first LP in our institution. Twenty-eight surgeons performed their first career LP at our hospital in the past 17 years. Although they had years of surgical experience, almost all started training in pediatric endoscopic surgery at our institution. Thus, we required easy and safe methods for some operations suitable for beginners. For that reason, we introduced the method of Dozier and Kim, 5 in which a VC is used for grasping the pylorus. This method increases the stabilization of the pylorus, making it easier to grasp and change its direction and position. Moreover, grasping the pylorus with the VC is less traumatic because the pressure is applied over a wider surface, and the pylorus does not slip off from the clamp. 5
Although the overall operative times for LP with VC and TLP were not significantly different, the operative time for surgeons' first LP was significantly shorter for LP with VC than for TLP (P = .048).
Therefore, we believe that this method is an easy and simple technique even for beginners of endoscopic surgery with the same incision for TLP (Fig. 3). As a matter of course, there is a learning curve for the evaluation of this method.

Surgical scars 9 months after laparoscopic pyloromyotomy with vascular clamp.
However, because of the overall decrease in surgical cases for HPS, it is difficult for one surgeon to perform many cases; one surgeon performed a maximum of 7 cases in recent years. Therefore, today we decided this method as the first choice of LP for not only beginners but also experts.
Conclusions
Among the several methods available for treating HPS, each hospital should choose the best method based on its own characteristics. Because LP with VC is an easy and safe procedure for LP, this procedure could be recommended for a teaching institution where there are not many cases of HPS.
Footnotes
Disclosure Statement
No competing financial interests exist.