
Abstract
Abstract
Introduction:
An upper gastrointestinal (UGI) series is a standard preoperative test for patients being evaluated for gastrostomy tube placement. We have recently begun to question the value of the radiation-exposing series in patients who tolerate gastric feeds.
Materials and Methods:
A retrospective review was conducted in patients who underwent laparoscopic gastrostomy tube placement between 2000 and 2012. Demographics, indication for gastrostomy tube, comorbidities, preoperative imaging, and nutrition were analyzed. Patients with foregut pathology and those who underwent prior gastrointestinal surgery were excluded.
Results:
Among 695 patients who underwent laparoscopic gastrostomy tube placement, the most common indications were failure to thrive (53%), neurologic disorder (25%), and dysphagia (12%). A UGI series was obtained for 420 patients (60%). Of these, 96 were found to have abnormalities (reflux, aspiration, anatomic). However, only 2 of these patients (0.3%) had a change in management, with 1 patient undergoing the Ladd procedure and 1 having negative diagnostic laparoscopy for suspected malrotation. In the subset analysis of 256 patients tolerating goal gastric feeds, 161 (63%) had a preoperative UGI series with only 2 patients (1.2%) having a resultant change in operative management: 1 undergoing the Ladd procedure and 1 having negative diagnostic laparoscopy. Of the 275 patients who did not have a preoperative UGI series, 1 patient (0.4%) was found to have malrotation postoperatively after two coins became lodged in the duodenum. This patient subsequently underwent an elective Ladd procedure.
Conclusions:
We found minimal impact of an UGI series during evaluation for gastrostomy alone. These studies may be able to be reserved for those with clear clinical indications.
Introduction
T
Two retrospective studies in the past decade examined the utility of UGI series in both fundoplication and gastrostomy tube placements. The first found decreased sensitivity of the UGI series when compared with pH study in the diagnosis of gastroesophageal reflux disease prior to fundoplication; however, approximately 4% of patients had anatomic abnormalities that led to a change in management, such as esophageal stricture and malrotation. 1 The second again confirmed the inferiority of UGI series in the diagnosis of reflux and challenged its usefulness in the diagnosis of unexpected anatomic abnormalities, particularly in patients without chromosomal or foregut pathology. 2
Routine evaluation prior to gastrostomy tube placement outlines the anatomy prior to the operation. However, when the patient is tolerating gastric feeds, particularly as bolus feeds, a meaningful obstructive pathologic finding becomes less likely, and an UGI series may be of little utility.
The value of UGI studies in a large series of gastrostomy patients alone has yet to be evaluated. Therefore, we sought to examine the rate at which UGI series is obtained in our institution and how often the results affect clinical management, particularly in those tolerating gastric feeding.
Materials and Methods
We performed a retrospective analysis on 695 pediatric patients undergoing laparoscopic gastrostomy tube placement after institutional review board approval (protocol number 14040155). All consecutively performed laparoscopic gastrostomy tube placements between 2000 and 2012 were identified by CPT code. Each patient had subsequent individual chart review performed. Gastrostomy placement was performed by general pediatric surgeons at a tertiary children's hospital, generally using the U-stitch laparoscopic technique. 3 Patients were excluded for known foregut abnormalities, conditions known to be associated with malrotation, and prior gastrointestinal operations, which have additional indications for UGI series besides gastrostomy tube placement. We chose to omit patients undergoing concurrent fundoplication as we have previously reviewed the use of UGI series in this population, 1 and the debate about the use of UGI seriesprior to fundoplication is independent of this question.
Data collected included demographics, indications for feeding tube placement, comorbidities, preoperative UGI results, and how they changed management. We also analyzed preoperative nutrition and route of delivery. Descriptive analysis was performed using mean and percentages.
Results
In total, 1196 patients were identified, and 695 were included in the analysis. Five hundred one patients were excluded, including those with concurrent fundoplication (n = 421), prior abdominal surgery (n = 52), and foregut pathology such as duodenal atresia, tracheoesophageal fistula, and congenital diaphragmatic hernia (n = 28) (Fig. 1). Demographics revealed a median age of 1.2 years, ranging from 0.01 years to 24 years, and 53% of patients were male. The median length of stay was 3 days, demonstrating the expected wide range from 1 day to over 1 year depending on the comorbidities (Table 1). The most common indications for gastrostomy tube placement were malnutrition or failure to thrive (54%) and neurologic disease (25%) (Fig. 2).
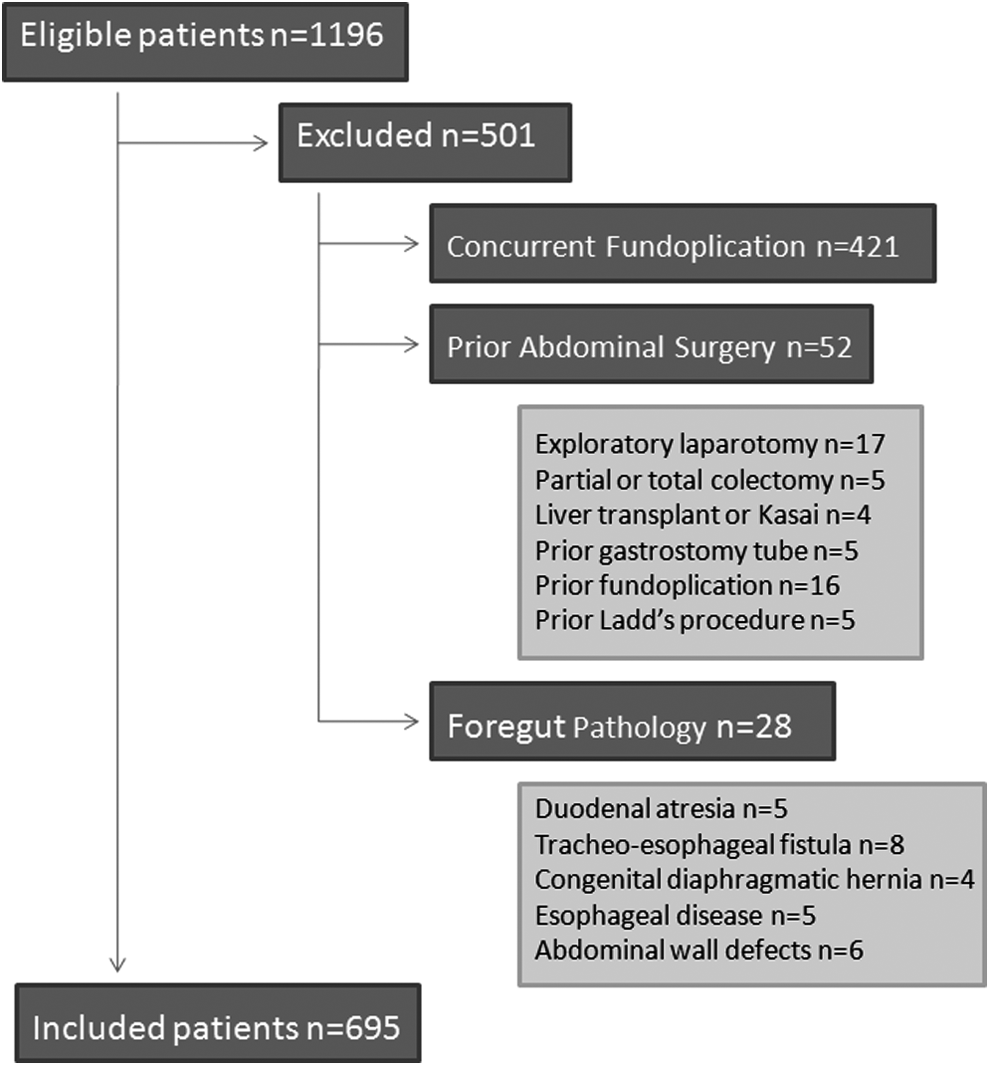
Reasons for excluding patients.

Indication for gastrostomy.
Data are median (range) values or number (%) as indicated.
In total, 420 patients underwent a preoperative UGI series (60%). Of these, 96 demonstrated abnormalities: reflux (n = 83), aspiration (n = 7), and anatomic (n = 7). Three studies revealed both reflux and aspiration. Of the anatomic abnormalities, four were concerning for malrotation, one for duodenal dilation, one for aberrant subclavian artery, and one for situs inversus. Two of these patients had a change in management due to concern for malrotation, representing 0.3% of the total patient population. One patient underwent a Ladd's procedure for confirmed malrotation, and the other had a negative diagnostic laparoscopy as the patient was found to have normal rotation. Although 1 patient had situs inversus, this did not significantly affect operative management.
Of the patients with preoperative nutrition data, the majority received gastric feeds orally, via gastric feeding tube, or a combination of both. Significantly fewer were receiving postpyloric feeding and parenteral nutrition (Fig. 3). A subset analysis was performed on the 256 patients tolerating goal gastric feeds preoperatively. Of these patients, 161 (63%) had an UGI series. Two (1.2%) of these patients (the same 2 patients mentioned above) had a change in operative approach.
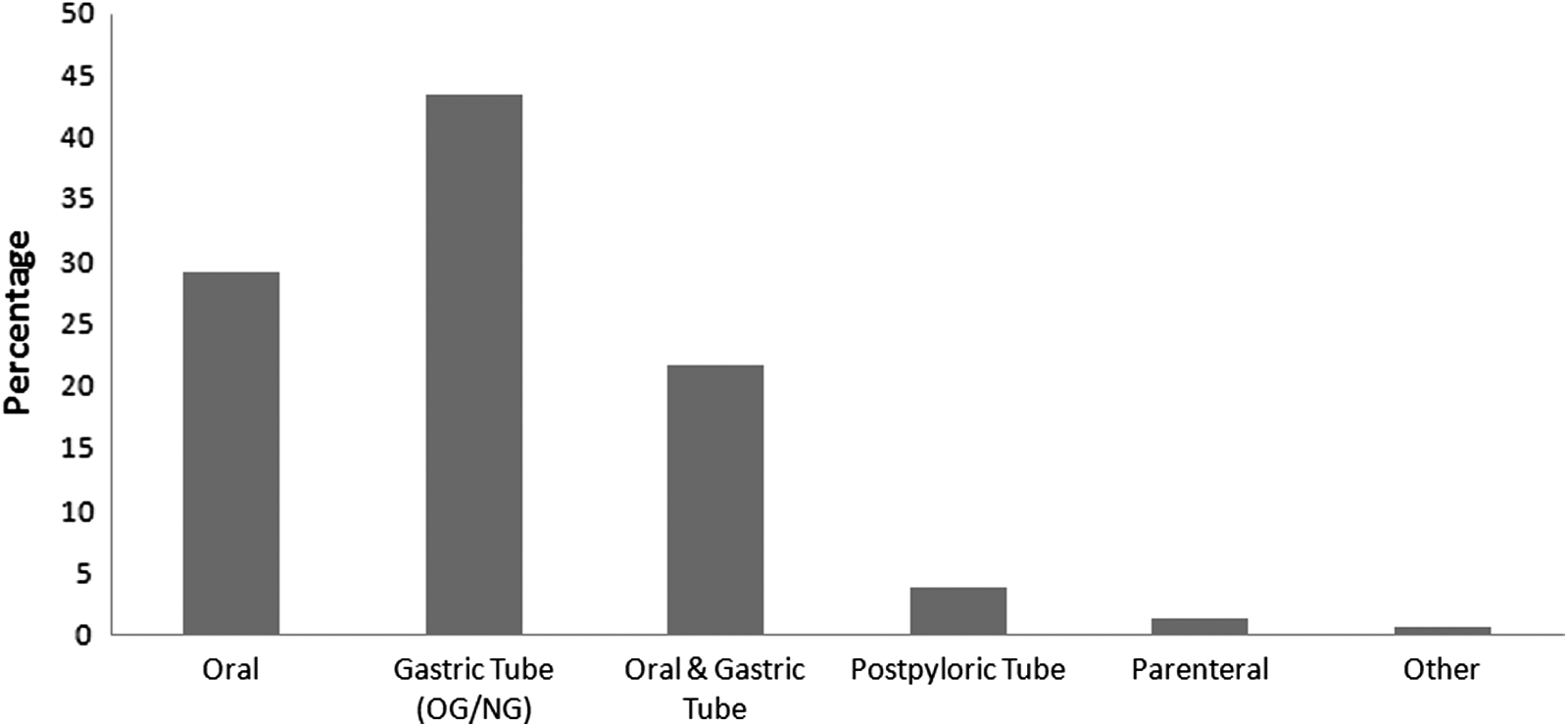
Route of preoperative nutrition. OG/NG, orogastric/nasogastric.
In the analysis of the 275 patients who did not receive an UGI series preoperatively, 1 patient (0.4%) was diagnosed with malrotation postoperatively when two coins became lodged in the duodenum. This patient underwent an elective Ladd procedure. There were no incidences of volvulus or adverse outcomes in the patients who did not receive a UGI series.
The rate of obtaining a preoperative UGI study did not change significantly during the study period. Between 2000 and 2012, 35%–77% of patients undergoing laparoscopic gastrostomy received a UGI series. The highest percentage (77%) was recently in 2011 (Fig. 4).

Rate of obtaining upper gastrointestinal (UGI) series over time.
Discussion
Healthcare costs within the United States are known to exceed their European counterparts at an estimated 15% of gross national product. And yet, health outcomes such as infant mortality have fallen behind. 4 Diagnostic testing has been approximated at 25% of the total expenditure and often challenged as largely unnecessary. 5 Multiple theories have been proposed to explain the high rate of radiologic testing, particularly preoperative tests.4,6 However, history and physical examination will often divulge critical preoperative information without the need for these tests. 7
In this study, we sought to examine the impact of the routine and well-accepted preoperative UGI series in patients considered for gastrostomy. The UGI study adds time and expense to the hospital course. The patient's comfort is compromised because a period of fasting is required, and small children may need to be restrained or have a nasogastric tube placed. In addition, the UGI study requires 60% of the ionizing radiation of a computed tomography exam of the abdomen and pelvis. 8 Ongoing initiatives are now widespread in reducing the amount of radiation in children/patients. Surgeons and emergency room physicians are working to decrease the use need for computed tomography scans to make a decision about performing an operation for appendicitis. Therefore, it is out of place that we routinely obtain an UGI study to provide anatomic information that fails to change the operative plan in 99% of cases. Patients who are tolerating gastric feeds without significant comorbidities associated with UGI abnormalities present a low-risk population if a laparoscopic gastrostomy is performed without a UGI series.
A counterargument to justify the need for an UGI series would be that even one missed asymptomatic malrotation may lead to a devastating complication; however, this line of argument would need to be extended to the entire population, and we do not routinely use a screening UGI study as part of the well child exam. In this report, of those without a preoperative study, only one malrotation was later diagnosed and without poor outcome. Of those with a UGI series, malrotation was radiographically documented in 4 cases and surgically confirmed in 1, consistent with what would be expected from the general asymptomatic population, the management of which is a separate debate.
We do not intend to suggest the UGI series should be abolished in this population. Patients with a known UGI abnormality or who are being worked up for vomiting may need a UGI study to rule out an obstruction or other associated abnormality. However, those patients who are not being considered for fundoplication that are tolerating gastric feeds are unlikely to benefit from a UGI series.
Limitations of this study include the retrospective nature at a single institution. There is also little risk to physicians and patients when reviewing the use of the UGI study retrospectively. Our data resonate with prior smaller studies challenging the usefulness of UGI series prior to feeding tube placement1,2 and justifies a prospective protocol to limit the number of UGI studies ordered.
There are several proven methods to reduce low yield preoperative testing. Some institutions have established guidelines regarding requirements prior to surgery in adults; these recommendations have substantially decreased cost without worsening outcomes.7,9 The first step is education of both surgeons and referring physicians. This article serves to further the discussion regarding necessary radiologic testing in the pediatric population.
Conclusions
Results of preoperative UGI series rarely changed operative management in patients undergoing laparoscopic gastrostomy tube placement. Clinicians should consider reserving this radiologic exam for patients with clear indications, such as foregut pathology. However, those tolerating gastric feeds without comorbidities may avoid the extra cost and radiation exposure with minimal effect.
Footnotes
Disclosure Statement
No competing financial interests exist.
K.W.G. is responsible for literature search, study design, data collection, analysis, interpretation and writing, and critical revision of the manuscript. B.G.A.D. is responsible for literature search, study design, and data collection and analysis. S.B. is responsible for data collection and analysis. P.A. and R.J.H. are responsible for study design, analysis, and critical revision of the manuscript. S.D.St.P. is responsible for the original question, literature search, study design, data analysis, interpretation and writing, and critical revision of the manuscript. D.J. is responsible for literature search, study design, data analysis, interpretation and writing, and critical revision of the manuscript.