
Abstract
Abstract
Introduction:
Traditionally open resection with hepaticojejunostomy (HJ) reconstruction has been the surgical treatment for cases of choledochal cyst. Our center has recently transitioned from open to laparoscopic and HJ to hepaticoduodenostomy (HD) as our preferred method of excision and biliary reconstruction. Our initial experience is presented here.
Materials and Methods:
A single-center retrospective chart review was performed from 2005 to 2014. All patients undergoing surgical treatment for choledochal disease were considered.
Results:
During the study period 18 patients had surgical treatment for choledochal cyst disease. The average age of all patients was 4.7 years (range, 2 months–15.5 years). Eleven of these patients had laparoscopic excision and reconstruction. Of these 11 patients, 7 had an HD anastomosis. Comparing the laparoscopic with the open group and the HD with the HJ group, there was no significant difference in operative time, estimated blood loss, time to regular diet, length of stay, or complication rate. Mean follow-up of 3.1 years revealed no documented cases of bile reflux or cholangitis. A recent adaptation in technique may improve ease of HD anastomosis. In this method, two strands of temporary monofilament suture cut to 8–10 cm each are tied extracorporeally. This knot is then placed on the outside of the medial corner. The anastomosis is then completed in a running fashion with the two strands and then secured intracorporeally at the lateral corner.
Conclusions:
Laparoscopic choledochal cyst resection with both HJ and HD reconstruction appears safe and has equivalent outcomes to open procedures in our series.
Introduction
C
Our center has recently shifted to using laparoscopic HD as the preferred method of biliary reconstruction after resection of choledochal cysts. The purpose of this study was to report the initial experience at our center in transitioning from open to laparoscopic techniques and from HJ to HD for re-establishment of biliary continuity.
Materials and Methods
After institutional review board approval (protocol number 1490405), a single-center retrospective chart review was performed from August 2005 to December 2014. Demographic data included age, gender, height, and weight. Perioperative data included presentation, operative time, type of cyst, anastomotic method, conversion rate for laparoscopic cases, time to regular diet, and complications including bile reflux, cholangitis, and anastomotic stricture. Findings are reported as mean ± standard deviation values.
Comparative analysis was performed using Student's t test for continuous variables and Fisher's exact test for binary variables. Significance was defined as P ≤ .05.
Operative technique: laparoscopic HD
Laparoscopic HD was completed with the patient in the supine position and a 15° reverse Tredelenburg position.
Port placement or stab incisions depending on the size of the patient are made in the following locations: a 5-mm umbilical port is placed to accomodate insufflation and 30° camera placement, a port or stab incision is placed in both the right and left midclavicular line just above the umbilicus as working ports, and a right subcostal retraction port or stab incision is made.
A suture is placed to encircle the falciform to aid in exposure of the porta hepatis. The cystic duct and artery are then dissected circumferentially, clipped, and transected. The gallbladder is then encircled with the suture through the abdominal wall for additional retraction.
The choledochal cyst is then dissected free from the hepatic artery, portal vein pancreas, and duodenum. Once the cyst is completely free, it is opened anteriorly to assess patency of the right and left hepatic ducts as well as the cyst's distal margin in relation to the duodenum and pancreas. The distal margin is then tied or clipped and transected. After the right and left hepatic ducts are probed for patency, the proximal margin of the cyst is transected.
The duodenotomy is made at least 2 cm distal to the pylorus. Two strands of temporary monofilament suture cut to 8–10 cm each are tied extracorporeally. Either strand is then passed outside to inside on the bowel or the bile duct, placing the knot on the outside of the medial corner. The opposite strand is used for lateral retraction while not in use. The posterior wall of the anastomosis is completed in a running fashion. This process is repeated on the anterior wall, and the two strands are then secured intracorporeally at the lateral corner (Fig. 1). This technique is further illustrated in the accompanying video (http://online.liebertpub.com/doi/full/10.1089/vor.2015.0277).
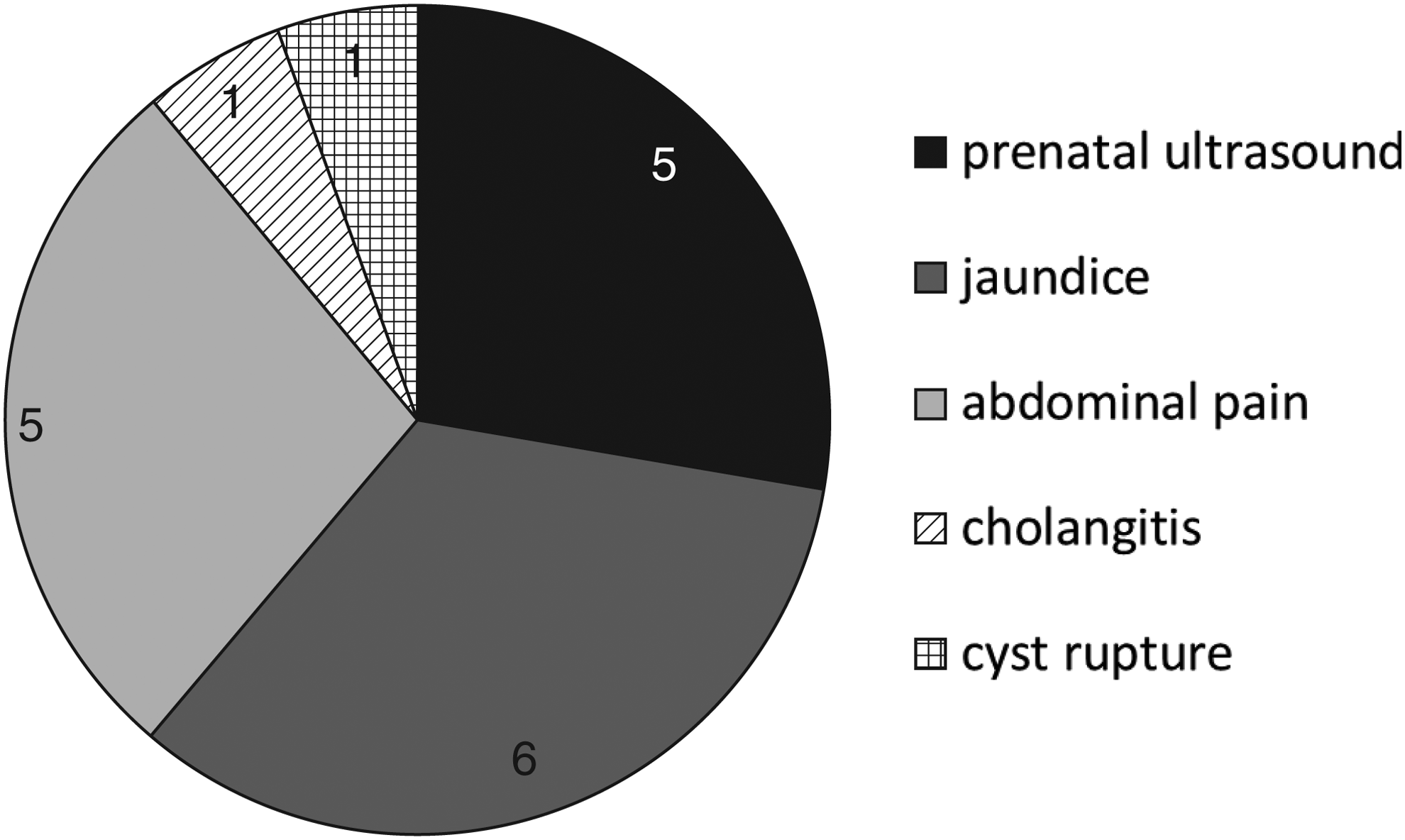
Method of presentation. The number of patients is given for each method.
All cases were performed with the assistance of a pediatric surgery fellow.
Results
During the study period 18 patients were identified who underwent resection of a choledochal cyst with biliary reconstruction at our center. Demographic data are shown in Table 1.
HD, hepaticoduodenostomy; HJ, hepaticojejunostomy.
A breakdown of presentation for these 18 patients is shown in Figure 1. Of note is that 1 patient presented with cyst rupture that was initially controlled with radiologic-guided drainage, and the patient underwent cyst resection 2.5 months later.
Seventeen of the 18 patients were diagnosed with a type 1 choledochal cyst, and the remaining patient's cyst was classified as type IVa. Definitive diagnosis was accomplished through magnetic resonance imaging for 10 patients, computed tomography in 6 patients, and ultrasound in 1 patient, and 1 patient was diagnosed intraoperatively. Thirteen cases were attempted laparoscopically, and 11 were completed laparoscopically. Seven of the biliary reconstructions were completed open. Seven patients (all in the laparoscopic group) had biliary continuity re-established via HD, whereas the remainder of patients had Roux-en-Y HJ reconstruction. Comparing the laparoscopic with the open group, there was no significant difference in operative time, estimated blood loss, time to regular diet, length of stay, or complication rate (Table 2). Although no statistical difference was found, an absolute difference of 1 day shorter length of stay was found in favor of the laparoscopic technique.
EBL, estimated blood loss.
All procedures with HD reconstruction occurred from April 2013 to November 2014, and all were performed laparoscopically. Reconstruction via HJ took place from July 2005 to June 2014. Comparison of HD with HJ revealed no differences in perioperative outcomes (Table 3). However, the absolute difference in length of stay was 1.5 days.
EBL, estimated blood loss; HD, hepaticoduodenostomy; HJ, hepaticojejunostomy.
Overall, the conversion rate was 15% in the 13 cases attempted laparoscopically. Although no cases were converted in the HD group, two of the six surgeries attempted laparoscopically in the HJ group were converted to open (P = .1). One case was converted for inability to complete the HJ anastomosis to satisfaction, and the other for inadequate mobilization of the Roux limb. Complications in the HJ group included a patient with a subcapsular hepatic hematoma that resolved without intervention. Another patient experienced a code event on postoperative Day 1, most likely secondary to narcotic medication. A third patient was discovered to have hyperbilirubinemia and subsequently required an anastomotic revision for a strictured hepaticojejunostomy 6 months postoperatively. Only 1 patient, who had an open HJ reconstruction, required re-admission in the first 30 days postoperatively. This admission was for nausea and emesis that resolved without intervention. A mean follow-up of 3.1 years revealed no documented cases postoperative cholangitis or bile reflux. Only 2 patients (1 in the HD and 1 in the HJ group) required a postoperative upper endoscopy for postoperative abdominal pain. Neither of these studies showed findings consistent with bile reflux.
Discussion
A recent meta-analysis showed similar outcomes for HD and HJ with a shorter length of stay in the HD population. 4 A single-institution retrospective review of laparoscopic versus open HD showed equivalent outcomes. 5 A large retrospective series comparing laparoscopic HJ to laparoscopic HD revealed near-equivalent perioperative outcomes for these two procedures. 6 Our data are consistent with these findings.
Although none of our perioperative data points reached statistical significance, the laparoscopic group compared with the open group showed an absolute reduction in length of stay of greater than 1 day, as did the HD group versus the HJ group, without a higher complication rate. The difference in the HD versus the HJ certainly may be attributed to the fact that all patients in the HD group had laparoscopic procedures. However, when open cases are removed the HD group still has an absolute reduction of 1.1 days. Estimated blood loss in the open and HJ groups was skewed by 1 case in which the patient had a preoperative diagnosis of cholelithiasis and was initially scheduled for a laparoscopic cholecystectomy.
The feared complications of cholangitis and bile reflux were not apparent in our HD population. A meta-analysis of 679 patients failed to show a difference in the rate of cholangitis between HD and HJ reconstruction but did reveal increased incidence of reflux or gastritis in the HD group. 4 Our series did not reveal any patients in either the HD or HJ group with cholangitis, bile reflux, or bile gastritis. One patient in both groups had an esophagogastroduodenoscopy postoperatively. The patient in the HD group had biopsies that revealed eosinophilic infiltration of the esophagus, stomach, and terminal ileum. The eosinophilic gastritis resolved on a subsequent biopsy. One patient in the HJ group was found to have eosinophilic esophagitis. A distance of ≥2 cm, as performed in this series, between the duodenotomy and the pylorus may confer some protection from bile reflux, but this has yet to be proven definitively.
Proponents of HD cite simplicity of operation given the one anastomosis and limited dissection needed to perform the anastomosis as advantages. We have found this to be true in our experience. Also, the method of tying together two strands of monofilament suture cut to about 8 cm extracorporeally prior to starting the anastomosis and exposure has expedited this step by making the strands more manageable intraabdominally.
Limitations of the study include its small sample size, making the results difficult to generalize. This is also a retrospective series, making selection bias a possibility. In addition, the mean follow-up of just over 3 years is short in comparison with a life expectancy postoperatively of 60–80 years.
Conclusions
Transition of surgical methods from open to laparoscopic and HJ to HD for the treatment of choledochal cysts is safe. The laparoscopic method and HD reconstruction may decrease the length of stay without increasing the complication rate. A recent modification in surgical technique has simplified HD at our center.
Footnotes
Disclosure Statement
No competing financial interests exist.
B.G.A.D. acquired data, supervised data acquisition and analysis, wrote the initial manuscript, critically reviewed and revised the manuscript, and approved it in its final form. K.W.G. and J.J.D. acquired data, critically reviewed and revised the manuscript, and approved it in its final form. W.S.A. critically reviewed and revised the manuscript. R.J.H. conceptualized the study, supervised data acquisition and analysis, critically reviewed and revised the manuscript, and approved it in its final form.